

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Vasospastic angina (VA) is characterized by acute chest pain at rest that is caused by contraction of the vascular smooth muscle tissue in large coronary arteries leading to coronary spasm (12). According to the current guidelines, invasive coronary angiography (iCAG) with either an acetylcholine or ergonovine provocation test (EPT) is required for a conclusive diagnosis in patients with clinically suspected VA (1). However, the iCAG with provocation test is invasive and, thus, inherently poses some risks to the patient, such as myocardial ischemia or infarction, serious arrhythmia, and puncture-site related complications (3). The introduction of coronary computed tomography angiography (cCTA) has had a significant effect on clinical practice, especially in the diagnosis of coronary artery disease. Owing to its high sensitivity and negative predictive value (NPV), cCTA is now accepted as a powerful noninvasive tool not only for identifying anatomic features of coronary arteries (i.e., luminal stenosis or the presence of plaques), but also for predicting long-term outcomes (456). To accomplish this purpose, the acquisition of high-quality images is critical, which can be realized by pre-cCTA administration of beta-blockers and sublingual nitroglycerin (SL-NG) for coronary artery dilation and heart rate reduction (7). Although cCTA has been widely used in the evaluation of patients with chest pain, there is a paucity of data regarding the impact of the use of beta-blocker and SL-NG on the diagnostic accuracy of cCTA in patients with suspected VA. Thus, the purpose of this study was to investigate the ability of cCTA to diagnose VA relative to the gold-standard iCAG-EPT. We also attempted to reveal the potential influence of pre-cCTA-administered beta-blockers and SL-NG on any discrepancy between iCAG-EPT and cCTA when assessing coronary vasospasm.
Go to : 
MATERIALS AND METHODS
Study Population
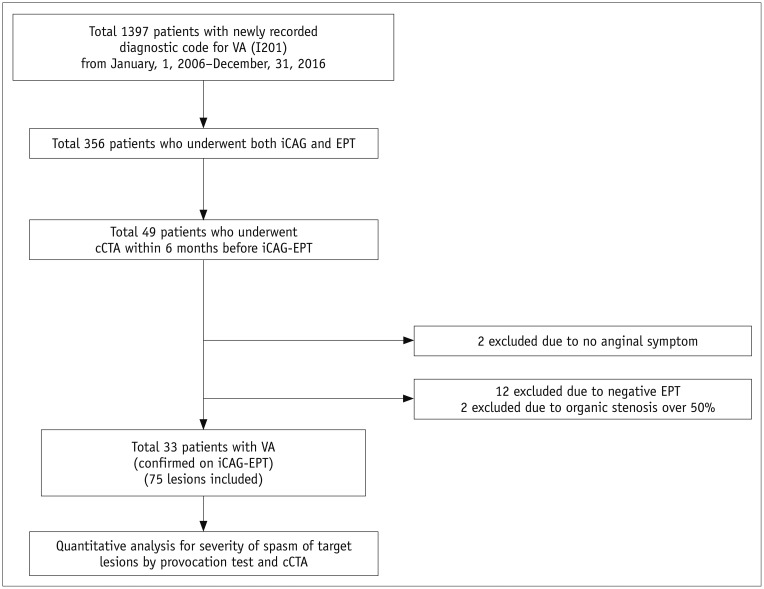
The selection process for the study population is presented in Figure 1. In brief, from January 2006 to December 2016, a total of 1397 patients who had a newly recorded diagnostic code of VA (I201) based on the International Classification of Disease, Tenth Revision, Clinical Modification were identified. Of them, 356 patients had undergone iCAG-EPT. Forty-nine of the 356 patients had undergone cCTA within 6 months before iCAG. Of them, patients with no anginal symptoms (n = 2) were excluded. After iCAG-EPT, those with no spasm in any coronary trees upon the provocation test (n = 12) and with coronary spasm on lesions with significant stenosis (% diameter stenosis [%DS] ≥ 50%) (n = 2) were further excluded. Finally, a total of 33 patients were included in the final analysis. Information regarding age; sex; body mass index (BMI); comorbidities including diabetes mellitus (DM), hypertension (HTN), dyslipidemia, and smoking; and administration of pre-cCTA medication including beta-blockers and SL-NG was collected by careful review of the electronic medical records. This study protocol was approved by the Institutional Review Board of Seoul National University Hospital and was conducted in accordance with the Declaration of Helsinki. The requirement for written informed consent was waived owing to the retrospective nature of the study.
iCAG-EPT
Experienced cardiologists performed iCAG via a transradial or transfemoral approach based on the current guidelines (8). Patients were instructed to stop using vasodilators, such as calcium channel blockers, nitrates, and potassium channel openers (i.e., nicorandil), 48 hours prior to the provocation test with the only exception of SL-NG administration, if needed. First, diagnostic coronary angiograms for the left and right coronary arteries were obtained. Coronary lesions with an organic stenosis of %DS ≥ 50% were excluded from the provocation test. The provocation test was then subsequently performed for the left and right coronary arteries using intracoronary ergonovine administration. Incremental doses of 30 (E1), 60 (E2), and 90 µg (E3) were injected into the left coronary artery and incremental doses of 20 (E10), 40 (E2), and 60 µg (E3) were injected into the right coronary artery (9). Care was taken to investigate both coronary arteries after the provocation test. After the provocation test was completed, intracoronary nitrate was injected to reverse coronary vasospasm.
Multi-Detector cCTA Image Acquisition
All CT examinations were performed using a dual-source CT scanner (SOMATOM Definition; Siemens Healthineers, Forchheim, Germany). Patients with a pre-scan heart rate of 65 beats per minute (bpm) or higher were given 50–100 mg of oral metoprolol (Betaloc; AstraZeneca, Sweden) 45–60 minutes prior to the CT examination, unless the subject had a contraindication to beta-blockers. Additional beta-blockers were not administered to subjects who underwent CT scanning 45–60 minutes after administration of beta-blockers, even if the heart rate did not fall to below 65 bpm. SL-NG (0.6 mg; Nitroquick; Ethex, St. Louis, Mo, USA) was administered if the patient had no contraindications to nitroglycerin for coronary vasodilation immediately before scanning. Sixty mL of a nonionic contrast medium (iopromide, Ultravist® 370; Bayer Healthcare, Berlin, Germany) was injected into the antecubital vein at 5 mL/sec, followed by an additional 20 mL of a nonionic contrast medium, and 50 mL of 8:2 mixture of normal saline and contrast medium, at a flow rate of 4 mL/sec using a dual power injector (Stellant; Medrad, Indianola, PA, USA). The bolus triggering method was used to determine the starting point of CT acquisition by monitoring the signal density of contrast medium in the mid-ascending aorta. CT scans were initiated 8 seconds after a threshold trigger of 150 HU above baseline was achieved. Details of the CT scan protocol have been described in previous studies (1011).
Image Interpretation of iCAG-EPT and cCTA
All iCAG-EPT and cCTA images were carefully reviewed by two independent investigators who were blinded to patients' clinical information. All conflicting results were resolved by consensus (κ = 0.781). For target lesions on iCAG images, the degree of stenosis was evaluated using quantitative coronary analysis (QCA) (CAAS QCA; Esaote, Genova, Italy) at baseline and after the provocation test to calculate the %DS in the iCAG-EPT. QCA analysis was conducted with blinding to the clinical information and cCTA results.
The degree of stenosis on cCTA was assessed semi-automatically using a dedicated cardiac workstation (Syngo. via; Siemens Healthineers). Corresponding sites to each spastic lesion identified on iCAG-EPT were evaluated for severity of stenosis, presence of atherosclerotic plaques, and vascular remodeling. Because negative vascular remodeling was reported as a main finding of spasm on cCTA (12), its presence at the spasm sites was investigated. Negative remodeling was considered present when the vessel area at the site of plaque was smaller than the distal reference (12). Analysis of cCTA images was also performed blinded to the baseline clinical characteristics and results of iCAG-EPT.
Statistical Analysis
To evaluate the influence of pre-medication on discrepancies between the two modalities, the lesions were categorized into groups based on pre-test administration of beta-blockers and SL-NG, and the difference in %DS (Δ%DS) of each lesion as measured iCAG-EPT and cCTA was compared between the groups. Subgroup analysis was performed to evaluate the impact of pre-medication on discrepancies in relation to accompanying cardiovascular risk factors such as old age (age ≥ 60 years), obesity (BMI ≥ 25 kg/m2), DM, HTN, dyslipidemia, and smoking. To determine whether temporal variance exists in diagnostic discrepancies, the lesions were further divided into groups according to when the cCTA was performed (from midnight to 10 AM or 10 AM to midnight) and compared for %DS assessed by iCAG-EPT and cCTA.
To assess the diagnostic performance of cCTA compared to iCAG-EPT, lesions with %DS more than 50% after the provocation test or on cCTA were defined as a significant spasm (13). The lesions were then subsequently classified into four groups according to the spasm seen on iCAG-EPT and cCTA: 1) Matched-Insignificant: concordant insignificant spasm, 2) Matched-Significant: concordant significant spasm, 3) Mismatched-Significant: significant spasm only on iCAG-EPT, and 4) Mismatched-Insignificant: significant spasm only on cCTA without spasm on iCAG-EPT. To ensure matching of spasm sites on cCTA images with those on iCAG-EPT, great care was taken to identify the adjacent side branches and lumen ostia that were used as landmarks (12). The diagnostic performance of cCTA was determined using the sensitivity, specificity, positive predictive value (PPV), NPV, and accuracy compared with iCAG-EPT on both a per-patient and per-lesion basis.
All probability values were two-sided, and a p value of < 0.05 was considered statistically significant. The statistical package SPSS, version 22.0 (IBM Corp., Armonk, NY, USA) and R version 3.3.3 (R Development Core Team, Vienna, Austria) were used for statistical analyses.
Go to :
RESULTS
Study Population
Baseline characteristics of the study population are presented in Table 1. There were 27 men with a mean age of 59.3 years. The median time difference between cCTA and iCAG-EPT was 11 days. Of the 33 patients, nine underwent cCTA between midnight and 10 AM (21 lesions). Prior to cCTA, both beta-blocker and SL-NG were administered to 19 patients (57.6%), beta-blocker alone to 5 (15.2%), SL-NG alone to 6 (18.2%), and neither beta-blocker nor SL-NG to 3 patients (9.1%). Fifteen patients (45.5%) had multi-vessel coronary spasm. Of the 75 lesions identified using iCAG-EPT, most were located in the right coronary artery (42.0%) and 45.3% showed diffuse spasm. The mean %DS recorded using iCAG-EPT and cCTA were 48.7 ± 14.7 and 14.4 ± 17.2, respectively. Plaque was visible in 22 lesions (29.3%), and only 6 (8.0%) lesions showed negative remodeling.
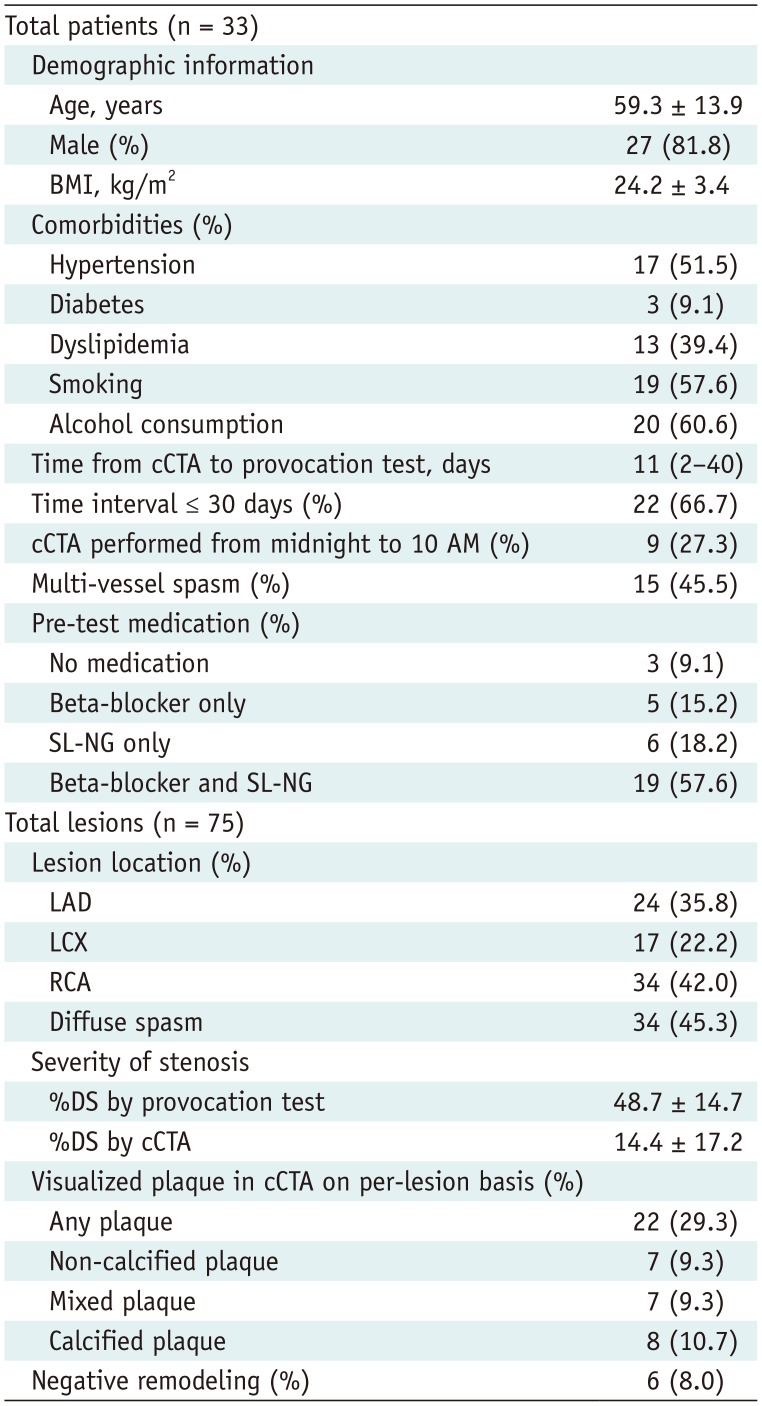
Table 1
Baseline Characteristics of Study Population and Related Coronary Lesions
Values given as mean ± standard deviation, median (interquartile range, 25th and 75th percentile), or number (percentage). BMI = body mass index, cCTA = coronary computed tomography angiography, LAD = left anterior descending coronary artery, LCX = left circumflex artery, RCA = right coronary artery, SL-NG = sublingual nitroglycerin, %DS = % diameter stenosis
![]()
Effect of cCTA Pre-Medication on the Discrepancies of Spasm Severity Assessed by iCAG-EPT and cCTA
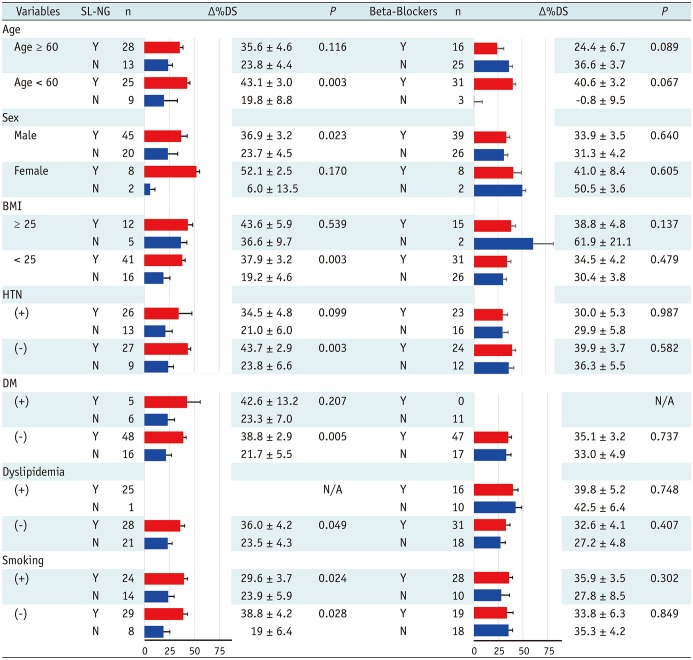
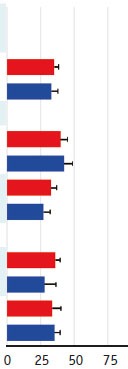
In terms of SL-NG use, the Δ%DS was significantly higher in lesions with pre-cCTA SL-NG (39.2% vs. 22.1%, p = 0.002) (Fig. 2). In contrast, there were no significant differences in Δ%DS according to the administration of pre-cCTA beta-blockers (35.1% vs. 32.6%, p = 0.643). Administration of SL-NG was associated with a significant difference in Δ%DS among those who were aged < 60 years; were male; had BMI < 25 kg/m2; and had no history of HTN, DM, or dyslipidemia, regardless of smoking history (Table 2). However, beta-blockers exerted no significant influence on discordance in Δ%DS regardless of the presence or absence of any cardiovascular risk factors. Although %DS assessed using iCAG-EPT was higher compared to that obtained from cCTA regardless of when it was performed, there was no significant Δ%DS (50.5% vs. 48.3%, p = 0.560 by iCAG-EPT and 14.0% vs. 15.0%, p = 0.814 by cCTA) and in Δ%DS (36.6% vs. 33.2%, p = 0.488) between lesions from cCTA performed from midnight to 10 AM or 10 AM to midnight (Fig. 3).
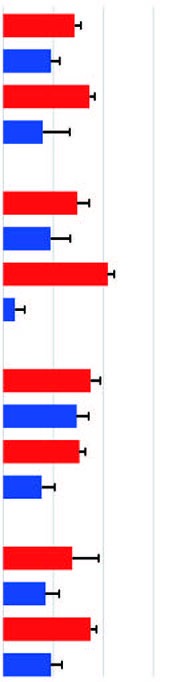
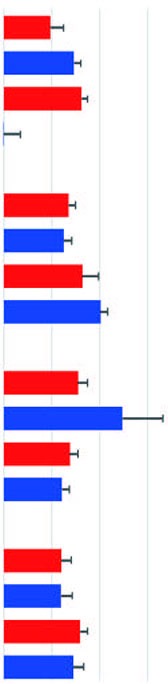
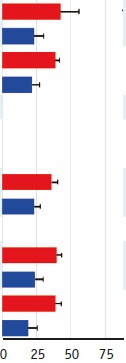
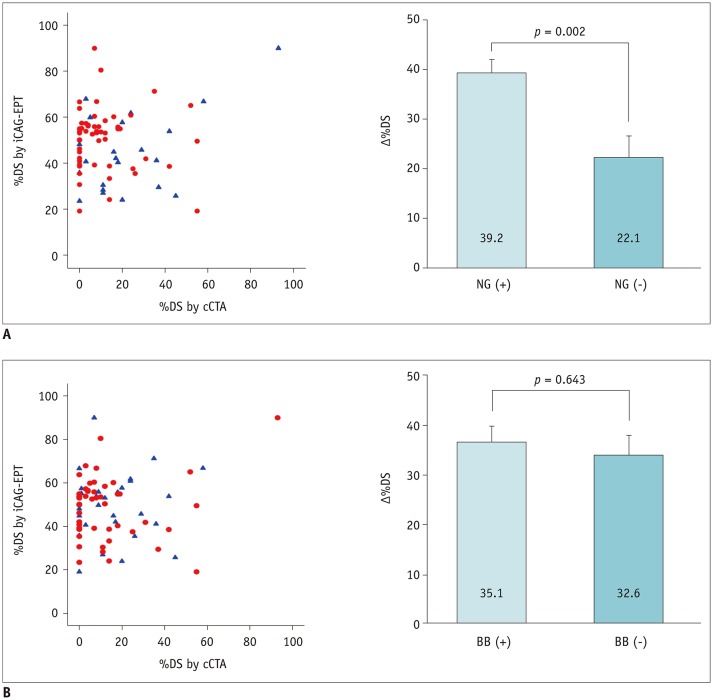 | Fig. 2Effect of pre-medication on difference in detecting severity of spasm between cCTA and iCAG-EPT.
A. SL-NG. B. BBs. BB = beta-blocker, iCAG-EPT = iCAG with EPT, SL-NG = sublingual nitroglycerine, %DS = % diameter stenosis, Δ%DS = difference in %DS
|
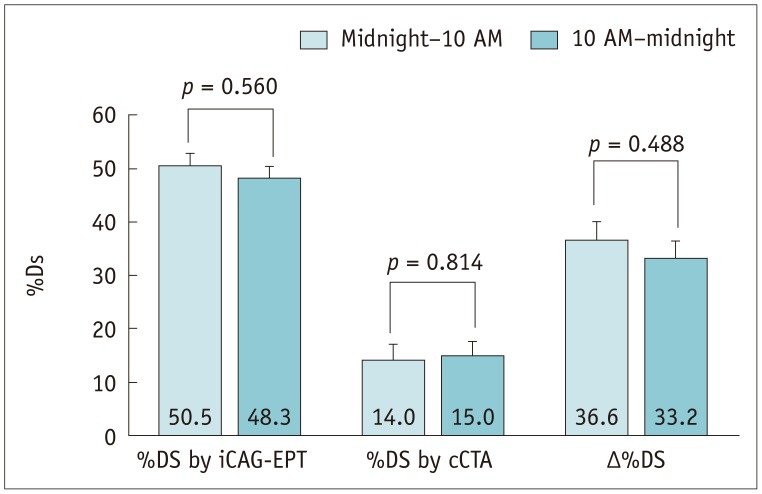 | Fig. 3Difference in severity of spasm between lesions according to time (from midnight to 10 AM or 10 AM to midnight) when cCTA was performed.
|
Table 2
Influence of cCTA Pre-Medication on Discrepancies of Spasm Severity Assessed by iCAG-EPT and cCTA According to Accompanied Cardiovascular Risk Factors
![]()
Diagnostic Performance of cCTA for Significant Spasms Compared to iCAG-EPT
Of the 75 lesions, 40 (53.3%) showed significant spasms on iCAG-EPT, whereas only five (6.7%) did so on cCTA. Overall, the discrepancy rate between the two diagnostic modalities was 52.0% (three [4.0%] Matched-Significant, 33 [44.0%] Matched-Insignificant, 37 [49.3%] Mismatched-Significant, and two [2.7%] Mismatched-Insignificant lesions) (Figs. 4, 5). With iCAG-EPT as the reference standard, the sensitivity, specificity, PPV, NPV, and accuracy of cCTA for the diagnosis of VA were 7.5%, 94.0%, 60.0%, 47.1%, and 48.0%, respectively on a per-lesion analysis, and 11.5%, 100.0%, 100.0%, 23.3%, and 30.3%, respectively on a per-patient analysis (Table 3).

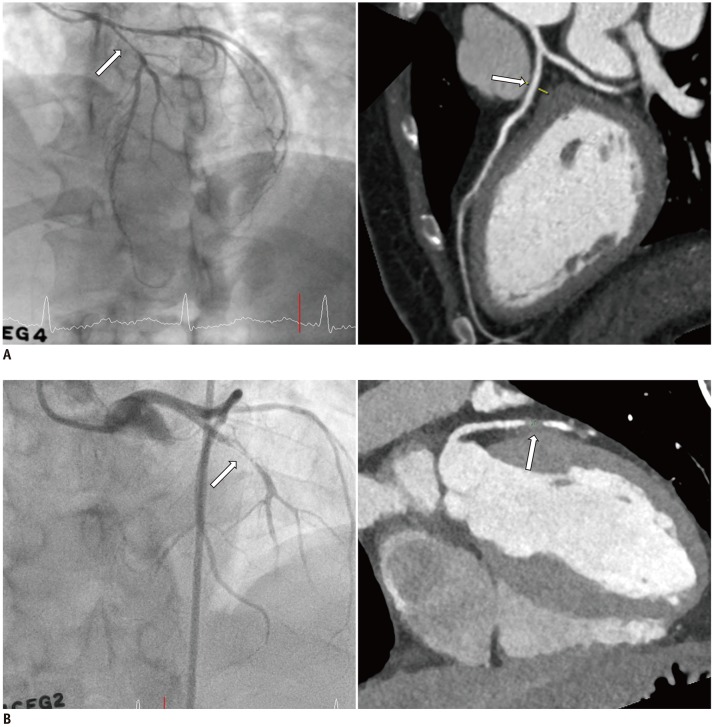 | Fig. 4Representative cases of Matched-Insignificant (A) and Matched-Significant (B) vasospasm between cCTA and iCAG-EPT.
|
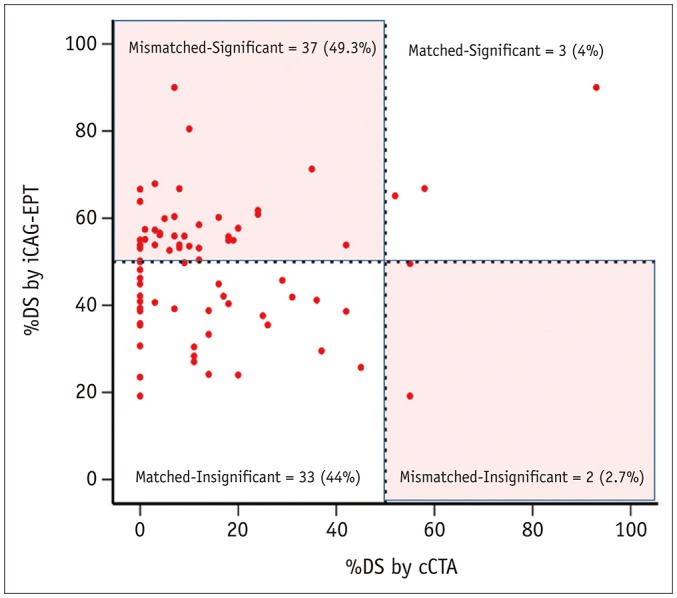 | Fig. 5Concordance or discordance between cCTA and iCAG-EPT in differentiating significant from insignificant vasospasm with use of 50% cutoff value.
|
Table 3
Diagnostic Performance of Coronary CT Angiography in Patients with Vasospastic Angina
| Per-Lesions Analysis Significant Spasm | ||||||
|---|---|---|---|---|---|---|
| iCAG | cCTA | Sensitivity | Specificity | PPV | NPV | Accuracy |
| 41 (54.7%) | 5 (6.67%) | 7.5% | 94.0% | 60.0% | 47.1% | 48.0% |
| Per-Patient Analysis Significant Spasm | ||||||
|---|---|---|---|---|---|---|
| iCAG | cCTA | Sensitivity | Specificity | PPV | NPV | Accuracy |
| 26 (78.8%) | 3 (3.81%) | 11.5% | 100.0% | 100.0% | 23.3% | 30.3% |
![]()
Go to :
DISCUSSION
The greatest clinical utility of cCTA is to reliably exclude fixed, obstructive coronary stenosis in patients with chest pain (5). Owing to its high NPV, cCTA was suggested to be a safe gatekeeper for iCAG (1415). Therefore, it is generally accepted that cCTA is the most accurate non-invasive imaging tool for screening anatomically “fixed” coronary artery stenosis in patients with chest pain. Apart from obstructive and fixed coronary stenosis, coronary spasm also plays a pivotal role in creating acute chest pain. Coronary spasm as a predominant cause of acute chest pain is clinically referred to as VA, and this unique type of angina pectoris is frequently found in East Asian populations, including Korean (12). According to guidelines (1), the confirmative diagnostic modality of choice for VA includes iCAG with ergonovine or acetylcholine provocation test, which can also provide anatomical information on the presence or absence of a high degree of fixed atherosclerotic stenosis. Further, as iCAG may induce rare but potentially life-threatening complications (3), effort has been made to develop a non-invasive imaging modality for the diagnosis of VA, such as ergonovine stress echocardiography (16). However, ergonovine stress echocardiography requires a non-invasive treadmill test or nuclear myocardial scan to pre-exclude significant coronary stenosis (14). In contrast, given its high accuracy and NPV (1614), it has been suggested that cCTA would be an ideal imaging modality to simultaneously evaluate both anatomically fixed and vasospasm-induced stenosis. Several studies have suggested the possible role of cCTA as a gatekeeper to iCAG-EPT (12171819). However, cases with false positive results of cCTA in VA have also been reported (2021), leaving the position of cCTA in the diagnosis or exclusion of VA in doubt. This may be attributed to differences in the characteristic findings in cCTA suggesting VA between studies and time-varying presentation of symptomatic vasospasm. To overcome this practical limitation, Kang et al. (17) and Jin et al. (19) proposed a new protocol dedicated to the diagnosis of VA. In brief, twenty patents clinically suspected of having VA underwent baseline cCTA in the early morning without administration of a vasodilator before the test followed by repeated cCTA within 3 days with a continuous intravenous infusion of nitrate. With this new proposed protocol, they showed significant improvements in the diagnostic performance of cCTA for the detection of significant coronary vasospasm (73%, 100%, 100%, and 56% for the sensitivity, specificity, PPV, and NPV of cCTA in a per-patient-based analysis, respectively). Application of this new protocol, however, is practically limited because of the double administration of contrast agent, dual radiation exposure, and availability of CT scanners early in the morning. In contrast, the current study reports disappointing results; the concordance rate in the detection of significant vasospasm between iCAG-EPT and cCTA (i.e., true positive or true negative lesions) was found in only 36 out of 75 spastic lesions, resulting in low sensitivity of 7.5%, NPV of 47.1%, and accuracy of 48.0% on a per-lesion-based analysis. We also found that there was no significant difference in the severity of vasospasm on cCTA regardless of the time when the test was performed. Taking these results together, the approaches that omit vasodilator (i.e., SL-NG) administration prior to cCTA, especially in the early morning, could be more informative in diagnosing vasospasm. However, further studies with a large number of patients would be required to validate this suggested protocol for the diagnosis of vasospasm.
Previously, Ito et al. (12) found that atherosclerotic plaques, mostly those that were non-calcified, were observed at all spasm sites by cCTA. In the present study, however, we could not confirm their findings; 23 (28.4%) lesions had atherosclerotic plaques and only seven lesions (8.6%) involved non-calcified plaques, while most spasm sites were free of atherosclerotic plaques. It is not clear why the discrepancy arises, but we speculate that the discrepancy may be related to the spatial/temporal resolution of CT scanners (17). This speculation is based on a previous intravascular ultrasonographic study (a modality with a high spatial/temporal resolution) showing the presence of non-calcified plaques at the spasm sites (22). In this respect, it is possible that further improvement in cCTA scanner technology with a higher spatial/temporal resolution may increase the diagnostic implication of non-calcified plaques at the spasm sites. To improve the diagnostic performance, previous studies (171822) combined various lesions characteristics including non-calcified plaques and negative vascular remodeling with significant stenosis, showing modest improvements in specificity and PPV. However, only six (8.0%) of the spasm lesions showed signs of negative remodeling in the current study, suggesting a limited role for this finding in the detection of spasm sites.
Beta-blockers and SL-NG are routinely administered before acquisition of cCTA images to improve the quality of coronary artery images, if no contraindications exist (7). As both pre-medications can exert a significant influence on coronary vasoactivity, the diagnostic accuracy of cCTA can be affected by their use. One scenario that clinically matters is the situation where SL-NG administration leads to normal cCTA results in VA; based on negative cCTA results, timely referral of the patient to iCAG-EPT could be delayed, leading to delayed optimal treatment. In fact, 11 (33.3%) patients in our series underwent iCAG-EPT more than 30 days after cCTA image acquisition. In addition, as beta-blockers can induce arterial spasm, their prescription in VA is discouraged among physicians. However, in the current study, we observed no significant association between pre-cCTA administration of beta-blockers and diagnostic discordance between cCTA and iCAG-EPT. This could be explained by the fact that beta-blockers, such as metoprolol, used for pre-medication mostly cause heart rate reduction via selective beta-1 receptor blockage without inducing coronary vasoconstriction mediated by beta-2 receptor blockage (23). Furthermore, regarding the impact of pre-cCTA medication according to the presence of coronary risk factors, SL-NG showed a consistent effect on discordance between iCAG-EPT and cCTA among patients who were aged < 60 years; were male; had BMI < 25 kg/m2; and had no history of HTN, DM, and dyslipidemia, which was not observed for beta-blocker usage. As endothelial dysfunction is known to be a major mechanism underlying coronary vasospasm (2425), those with a higher burden of cardiovascular risk factors may lead to endothelial dysfunction more severely, attenuating the effect of SL-NG on coronary vasodilation (2627).
Several limitations need to be acknowledged. First, this is a retrospective, observational study in a relatively small number of patients, and thus, a selection bias may be present. Therefore, further larger prospective studies need to be performed to consolidate the current findings. Second, the interval between cCTA and iCAG-EPT was over 1 month in 11 patients (33.3%). Third, there might be a possibility of mismatch between the exact spasm sites on cCTA and those on iCAG-EPT. However, we tried our best to ensure matching of the spasm lesions on cCTA with iCAG-EPT lesions by using side branches and ostia as landmarks. Fourth, as we analyzed only single cCTA results in patients with VA, temporal variation of vasospasm could not be analyzed in the current study. Lastly, although we used the EPT as a gold standard method to diagnose VA, a previous report showed a false negative result on iCAG-EPT (28).
In conclusion, for patients with clinically suspected VA, a final diagnosis made based on iCAG-EPT needs to be considered without excluding the diagnosis of VA simply based on insignificant results on cCTA, although further prospective studies in a large number of populations are required for confirmation. If confirmed, the development of a new cCTA protocol dedicated to the diagnosis of VA would be an interesting topic and of clinical importance.
Go to :
 XML Download
XML Download