

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebral microbleeds (CMBs) are a chronic accumulation of small blood products in the brain tissue.1 When brain magnetic resonance imaging (MRI) began to apply a high magnetic susceptibility technique in the mid-1990s, CMBs became well known.2 With further development of MRI techniques, the detection rate of CMBs increased significantly, and it has become of great interest and importance to certain conditions, such as dementia and stroke, as well as normal aging.
The prevalence of CMB varies according to the subject and disease being investigated. In an extensive study of community-dwelling middle-aged or older adults,34 the prevalence of CMB was 11.1%–15.3%. The incidence of CMB was 6% in the late 40s, and 38% after age 80.56 The CMB prevalence has been reported to be 18%–32% in Alzheimer's disease, 20%–43% in mild cognitive impairment, and 68%–85% in subcortical vascular dementia.789 And, it occurred in 20%–70% of patients with cerebral hemorrhage, and 30%–40% of patients with cerebral infarction.10
CMBs have been considered to be asymptomatic lesions that may be found incidentally on the brain MRI.1112 Recently, CMBs were associated with an increased the risk of cognitive decline, dementia, intracerebral hemorrhage (ICH), cerebral infarction, or recurrence of transient ischemic attack,713 and mortality rate.14 And it has been shown to play the role of a biomarker in small vessel disease (SVD), such as hypertension, cerebral amyloid angiopathy (CAA), and chronic kidney disease.515
Despite the growing interest and investigations in CMB, many issues remain to be clarified, such as the precise developmental mechanism, clinical significance, prognosis, and treatment of CMBs. In this paper, we review clinical research on CMBs and discuss the future directions for study.
DEFINITION OF CMB
CMB is a small circular or elliptical lesions with a size of 2 to 10 mm in a gradient-recalled echo (GRE) image or susceptibility-weighted image (SWI) (Fig. 1).216 Histopathologically, CMB shows hemosiderin accumulation in the surrounding blood vessels, in the same region that appears as a hypointense lesion on brain MRI.17 Greenberg suggested criteria (Table 1) to differentiate among diseases that are easily confused with the neuroimaging features of CMBs.2 In addition, Wardlaw et al.16 proposed a standardization neuroimaging definition of CMBs, to be used for SVD studies.
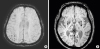 | Fig. 1CMBs on gradient-recalled echo imaging in brain magnetic resonance imaging. (A) Multiple CMBs in the parietal lobe (B) multiple deep CMBs in bilateral basal ganglia and thalamus.CMB: cerebral microbleed.
|
Table 1
Recommended criteria for cerebral microbleed identification

| Greenberg's criteria1 | |
| - Black on GRE T2*-weighted MRI | |
| - Round or ovoid (rather than linear) | |
| - Blooming on T2*-weighted MRI | |
| - Devoid of signal hyperintensity on T1- or T2-weighted sequences | |
| - At least half surrounded by brain parenchyma | |
| - Distinct from other potential mimics such as iron/calcium deposits, bone, or vessel flow voids | |
| - Clinical history, excluding traumatic diffuse axonal injury | |
| Wardlaw's definition16 | |
| Small (generally 2–5 mm in diameter, but sometimes up to 10 mm) areas of the signal void with associated blooming seen on T2*-weighted MRI or other sequences that are sensitive to susceptibility effects. | |
![]()
CMB requires differentiation from other hypointense lesions in GRE and SWI. For instance, calcium or iron depositions appear as hypointensities in the bilateral basal ganglia, choroidal plexus, and pineal gland. It can be distinguished from CMB by the location and very high-signal intensity on computed tomography. The blood flow of the pial vessels also is seen with the same signal intensity of CMB, with round shape on the T2-weighted image and GRE. It is possible to discriminate the 2 by continuity with other slices.2 Artifacts in the frontal or temporal lobes, due to the orbital or mastoid bone7 and cavernous malformations, occur in the curved space in which stagnant blood and multiple stages of blood products produce various signals.18 Melanin can be confused with CMB because of its hemorrhagic tendency, but melanin can be distinguished by high signal intensity on T1-weighted images and edema around the lesion.19
CMB DETECTION USING BRAIN MRI
Findings of CMBs are affected by echo time, spatial resolution, and intensity of the magnetic field.2021 As the MRI magnetic field strength increases and the cross section becomes thinner, the blooming effect, which produces an image larger than the actual amount of accumulated blood iron, becomes so large that the CMB can be confirmed with greater sensitivity.2022 GRE and SWI are commonly used in clinical practice to detect microbleeds in the brain. SWI is recommended for quantifying numbers of CMBs because it showed more inter-rater reliability and higher sensitivity for detection CMB, than GRE in previous studies.132223
For evaluating CMB, visual scoring systems and an automated or a semi-automated brain imaging analysis method are used.2425 Visual scoring systems include the Microbleed Anatomical Rating Scale (MARS)26 and the Brain Observer MicroBleed Scale (BOMBS).27 In both methods, CMB is scored by location, such as right or left infra-tentorial, deep, and cerebral hemisphere; and by certain or ambiguous. The MARS scale is different in that the cerebral regions are divided into each lobe, whereas the BOMBS is divided into the cortex and subcortical regions (Fig. 2). Reliability of the assessed number and location of CMBs is low without the use of an evaluation tool, and these visual scoring systems do not show any significant difference in results, even when applied to other MRIs with different echo times.
 | Fig. 2Visual rating of cerebral microbleeds. (A) The Microbleed Anatomical Rating Scale,26 (B) The Brain Observer MicroBleed Scale.27B: brain stem, Bg: basal ganglia, C: cerebellum, Cc:corpus callosum, DPWM: deep periventricular white matter, Ec: external capsule, F: frontal lobe, I: insula, Ic: internal capsule, O: occipital lobe, P: parietal lobe, T: temporal lobe, Th: thalamus.
|
Therefore, it is helpful to identify the presence, number and location of CMB systematically to provide more clinical information on microbleeds.
RISK FACTORS OF CMB
Age is an important risk factor for the development of microbleeds in the brain, and an increase in CMBs is associated with advancing age, white matter hyperintensities, and lacunar infarction. A recent cohort study of more than 2,500 community-dwelling people, done over a 5-year period, showed a 2.6-fold increase in the risk of lobar microbleeds in participants with brain atrophy.28
Hypertension is the most reliable risk factor for CMB. It causes increasing vascular endothelial cell damage, and inflammation due to tumor necrosis factor.2930 It is also associated with lacunar infarction, white matter hyperintensities and left ventricular hypertrophy. When two or more retinal microvascular signs, such as retinal arteriovenous stenosis due to hypertension are observed, the risk of microbleeds in the brain is increased 3-fold.28 Therefore, it can be assumed that vascular injury due to hypertension causes CMBs.22231
Cholesterol, diabetes mellitus, and smoking have also been reported as risk factors for microbleeds, but the results differ according to the study. Although some studies have shown hypercholesterolemia lowered the risk of microbleeds and statin therapy increased the risk of cerebral hemorrhage,3233 meta-analysis results showed the opposite.34 Cystatin C, a new renal function indicator, has been associated with deep and infratentorial CMB, as well as chronic kidney disease, implicating it as a risk factor for CMB.35
The incidence of microbleeds is less than 1 per year, but it is high in cases of: 1) more than 5 CMBs in the early stage of disease, 2) severe SVD pathology, or 3) CAA with apolipoprotein ε2 or ε4 genotype.323637 Of the apolipoprotein E genotypes, ε2 is associated with fibrinoid necrosis, and ε4 is characterized by accumulations of β-amyloid, absence of smooth muscle fiber, and vessel wall thickening, resulting in microbleeds.638 In a pathology study, more than 50 counts of CMBs in a patient were associated with thicker amyloid-deposited vessels than with less than 3 number of CMBs.39 This indicates that the number of CMBs reflects the underlying vascular disease state and is a biomarker of future microbleed occurrence.
PATHOPHYSIOLOGY OF CMB
The pathophysiology of CMB has not yet been fully elucidated. However, hypertensive microangiopathy and CAA could damage the blood-brain barrier and neurovascular unit, to cause CMBs with blood leakage and hemosiderin deposits in the brain parenchyma. Hypertension causes lipohyalinosis, and fibrohyalinosis which affect the deep penetrating arterioles and accumulation of Aβ in the cortical and leptomeningeal arteries, resulting in inflammation, oxidative stress, and apoptosis. Also, cerebral amyloid disease, chronic kidney disease, and cardiac disease, commonly damage arteriolar smooth muscle cells and capillaries, which comprise the blood-brain barrier and neurovascular unit.40
Recently, a relationship between CMB and enlargement of the perivascular space in the centrum semiovale seen by MRI, was proposed. It was speculated that amyloid accumulation in CAA may cause enlargement of vascular space and microbleeds.414243 In Alzheimer's disease, CMB occurs mainly in the cortical-subcortical boundary and is caused by CAA associated with Alzheimer's disease. It is accompanied by blood-brain barrier dysfunction, as well as Aβ deposition in blood vessels. More than 87% of CMBs located strictly in the lobar regions and predominantly in the posterior cortex of the brain and not in the deep gray matter or brainstem, are likely caused by CAA.44 On the other hand, hypertensive microbleeds predominantly occur in deep gray matter or the brainstem.
DISEASES ASSOCIATED WITH CMBs
Dementia and cognitive decline
CMB has been shown to increase the risk of dementia and cognitive decline in patients with cognitive impairment, as well as in the normal community-dwelling population.61942 Although the number of CMB needed to affect cognitive function has not yet been determined, some studies have examined the relationship between number of CMB and cognitive function. In the Rotterdam study,643 the number of CMBs was associated with a greater cognitive decline, with more pronounced cognitive dysfunction at 4 or more CMBs, and decline of all cognitive functions, except memory at 5 or more CMBs.
CMB could damage function at the bleed location or cause various non-specific cognitive declines. Lobar microbleeds have been related to the Mini-Mental Status Examination score (general cognitive function), executive function, process speed, and memory impairment. Deep and infratentorial microbleeds have been associated with motor or psychomotor speed, and attention deficits.7 CMBs in the temporal lobe have been associated with memory and attention deficits, and frontal CMBs with dysfunction of memory, mental speed, set shifting, and attention.36
In general, CMBs are associated with a higher risk of dementia or cognitive decline in patients with cognitively normal, mild cognitive impairment, Alzheimer's disease or vascular dementia. Although there have not been many longitudinal studies analyzing the effect of CMBs on cognitive function over time, microbleeds in patients with ICH have been associated with a higher likelihood of cognitive decline.
CMB distribution is different among dementia types. CMBs in CAA, and in AD patients showed lobar distribution predominantly. CMBs in patients with Lewy-body dementia or fronto-temporal lobar degeneration, also occurred at lobar locations predominantly. However, CMBs in vascular dementia patients were distributed equally in the lobar, deep and infratentorial regions.45
Stroke
Microbleeds accompany strokes with lacunar infarction more often than cerebral infarction by atherothrombosis or cardioembolism. This suggests that microbleeds are associated with small vessel lipohyalinosis.46 CMB is used as a predictor of future stroke. In patients with lacunar infarction or transient ischemic attack, CMB is more likely to cause cerebral hemorrhage, as well as ischemic stroke.12224748 In particular, if there are more than 10 CMBs or multiple CMBs in the lobes, the risk of bleeding is higher.3149 Stroke mortality is significantly higher in patients with CMBs, than with other associated vascular risk factors.365051
Cerebral hemorrhage including CMB is classified as lobar hemorrhage. It is can be located in the cortex due to damage of cortical/leptomeningeal vessels by CAA; seen as deep hemorrhage caused by hypertension with damaging deep perforating artery; or mixed hemorrhage, a combination of lobar and deep hemorrhage.41 As lobar hemorrhage shows more severe white matter change in the occipital area, and has a higher frequency of ε4 than deep hemorrhage, this type of bleed is more likely to occur due to CAA.52 Deep or infratentorial microbleeds occur when there is a high systolic blood pressure, a high blood pressure fluctuation, a lacunar infarction, or severe white matter hyperintensities.353 Mixed hemorrhage has been associated with more lacunar infarction and lower risk of recurrence of hemorrhage, compared to only lobar hemorrhage or deep hemorrhage. Mixed hemorrhage was also associated more with older age, number of CMBs, and higher recur risk than deep hemorrhage, suggesting that location, mechanism, and prognosis are different between deep and mixed hemorrhage types.41
Genetic diseases
CMBs can appear in various diseases, such as cerebellar autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), autoimmune encephalitis, traumatic brain injury, cerebral degeneration after radiation therapy, and Moyamoya disease.212223 The incidence of CMB in CADASIL ranges from 30% to 70%, and increases with age, mainly in the thalamus.21 COL4A1 mutation carriers have a variety of brain lesions, such as white matter hyperintensities, perivascular enlargement, and microbleeds. More than half of the patients have CMBs that develop mainly in the deep white matter, gray matter, brainstem, and cerebellum.24 The sortilin-related receptor gene was reported to correlate with microbleeds in populations with hypertension, and involved the amyloid cascade process.54
MANAGEMENT AND PROGNOSIS
Although there is no proven therapy for CMB, management of hypertension may be helpful in microbleeds because blood pressure control can reduce not only hypertensive deep hemorrhage, but also CAA-induced lobar hemorrhage.10 Although different results have been seen, depending on study design and medications, the use of antiplatelet, antithrombotic, and thrombolytic agents for prolonged periods may cause CMBs.4446
Risk of CMB may influence the treatment of accompanying disease. There is insufficient evidence to limit the use of anticoagulants unconditionally for the treatment of atrial fibrillation in patients with CMBs. However, use of anticoagulants is not recommended in patients over 60 years of age with atrial fibrillation who require anticoagulant therapy, but may have: 1) a history of cerebral hemorrhage and superficial siderosis, 2) an intracranial hemorrhage in mid-life, 3) a family history of early-onset dementia and MRI findings suggest CAA, or 4) a multiple CMBs after taking 2 antiplatelet agents for acute cardiovascular disease.55 Caution should be exercised when selecting intravenous thrombolytic agents for management of acute cerebral infarction accompanied by CMBs. Studies have shown that the risk of cerebral hemorrhage is relatively greater after thrombolysis in the presence of CMB, and more symptomatic ICH occurs with higher numbers of microbleeds. However, there is not enough evidence yet to determine the appropriate use of thrombolytic agents in the cases of patients with CMBs. In relation to the treatment of Alzheimer's disease, some researchers have recommended that patients with more than 4 CMBs be excluded from treatment with Aβ immunotherapy.9 This is because an inflammatory reaction could be triggered by the immunotherapy agent used to target amyloid in the tissue and vessels.56
CONCLUSIONS
CMB increases the risk of cognitive decline or dementia, as well as increases the risk of stroke and stroke mortality. In addition, it plays a role as a biomarker of SVDs, such as arteriosclerosis and CAA, and the extent of CMBs can be used as an index to estimate the status of underlying disease. Therefore, systemic and quantitative evaluation should be used to assess prognosis. Further studies are needed on treatment guidelines that consider the risk of cerebral hemorrhage when there is CMB in stroke patients, and appropriate blood pressure therapy to prevent CMB occurrence.
 XML Download
XML Download