

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Brain imaging is an essential tool utilized in the diagnostic process of patients with dementia symptoms.12 Although the brain magnetic resonance imaging (MRI) is a principal test to determine dementia in a patient, in some circumstances, it has been replaced with the use of computed tomography (CT) scans, for limiting the financial difficulties of patients and caregivers or for large-scale community dementia examinations.3 Most cases of Alzheimer's disease or vascular dementia, which is a major part of the disease caused by dementia, can be diagnosed with the use of a CT scan alone, but some dementia patients are not sufficiently reviewed for diagnosis based on the results of only a CT examination alone.
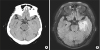
In this study, a 76-year-old female presented with a 3-week history of cognitive decline and significant gait disturbance. These symptoms had deteriorated abruptly and worsened over time. The patient was on medications for managing the conditions of hypertension and diabetes, and was devastated by the death of his spouse a month ago. In the neuropsychological test, the patient had difficulty in performing the cognitive function testing because not only the patient's memory function had decreased but the patient's language ability had also significantly decreased. The Korean version of the Mini-Mental Status Examination (K-MMSE) score was 5/30, and the result of the Korean version of the consortium to establish a Registry for Alzheimer's Disease Assessment Packet (CERAD-K) showed that there was a significant decline in the entire cognitive area considering her education level and age. On neurologic examination, the weakness of both lower extremities was not definite, and that the deep tendon reflex and cranial function test were normal, but, could not maintain a standing position. At first, the possibility of a vascular dementia or space occupying brain lesion was high, and a rapid test was recommended considering the sudden occurrence of the disease and the medical history of hypertension and diabetes with the patient. The patient conducted a diagnosis program for the dementia care center due to financial conditions, and underwent a routine blood test and CT examinations. In the brain CT scan, a mild atrophy and several small vessel lesions were seen, but there was no distinct lesions to describe the symptoms (Fig. 1A). However, in addition to the examination program, the patient was admitted to the hospital to conduct further tests in consideration of a review of the continuous progress of their symptoms.
On the brain MRI examination, a note of multifocal infiltrative enhancing lesions were observed involving the right high frontal cortex, bilateral frontoparietal white matter, left medial temporal and occipital lobe, thalamus, corpus callosal splenium, and bilateral cerebellar dentate nucleus areas (Fig. 1B). These findings were indicative of a central nervous system lymphoma, and we also checked the chest area for an evaluation of the possibility of a cancer metastasis, but we could not conduct further evaluation for brain lesions, because of disclaimers of the patient family due to economic conditions. In this case, it was initially difficult to diagnose accurately with a CT, and for that reason a MRI was needed, which allowed access to view and analyze the cause disease. Considering the limitations of CT examinations, even in a community examination that uses CT, we must include additional MRI if the clinical presentations of patients were not seen to have followed a common progression of Alzheimer's or vascular dementia, especially on a review and through the close attention to the detailed patient history.
 XML Download
XML Download