

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Memory is a 2-pronged function, involving recall of the past and planning for the future.1 Prospective memory (PM), referred to as ‘remembering to remember,’ entails the formation of future action representations, temporary storage of such representations in memory, and their retrieval at future time points.2 PM is pivotal in meeting the challenges of daily living, and is key to autonomy and independence. PM tasks rely on self-initiated retrieval of intentions within specific time frames and involve externally prompted retrieval of information content.23 PM is further characterized as time- or event-based recollections. Time-based PM relates to actions to be taken at specified points in the future or after a specified period of time, whereas event-based PM pertains to actions triggered by specific events2; memory being crucial in both instances.3 Thus, successful execution of PM tasks requires not only timely detection of prospectively cued events/target times (prospective component), but also correct retrieval of delayed intention content (retrospective component).3 PM deficits are particularly pronounced in individuals with mild cognitive impairment and Alzheimer's disease (AD),45678910 and several areas of the brain have been identified as PM-related regions. Based on the cumulative evidence of neuroimaging studies to date, the frontal cortex, particularly rostral prefrontal cortex (approximating Brodmann area 10), is primarily implicated in PM.11121314
Cerebral small vessel disease is typically manifested as white matter hyperintensities and lacunes. Past studies have shown that the aggregate or extent of white matter hyperintensities (WMHs) predicts the rate of cognitive decline in mild cognitive impairment (MCI),1516 and in AD17 there is evidence that WMHs distributed in anterior regions of the brain bear an association with cognitive impairment and markers of AD pathology.18 Many studies have also demonstrated that WMHs negatively correlated with cognitive performance, including processing speed, immediate and delayed memory, executive functions, global cognitive functions1920212223 governing mobility,2425 urinary control,2627 and activities of daily living (ADL),28293031 in non-demented elderly adults and patients with AD. The link between WMHs and frontal dysfunction has been particularly well established. Consequently, we anticipated that WMHs may impact PM in patients with amnestic mild cognitive impairment (aMCI).
The purpose of this study was to assess PM differences in patients with aMCI, based on degree of WMHs, investigating whether PM changes are worsened by extensive WMHs. We also examined other factors, namely type of WMHs (periventricular vs. deep), acetylcholinesterase inhibitor (AChEI) use, and apolipoprotein E (APOE) genotype, for their effects on declining PM.
METHODS
Study participants
Between December 2011 and January 2014, we recruited consecutive patients with aMCI at 3 memory clinics of university-based hospitals. Although 74 patients were initially enrolled, only 69 patients (93.2%) completed this prospective study. Four of the 5 patients excluded from this analysis were lost to follow-up, and one patient withdrew consent. At baseline, all patients underwent standardized dementia assessments encompassing basic demographics, informant-based histories, collection of past medical histories, physical/neurologic examinations, comprehensive neuropsychological testing, laboratory diagnostics, and magnetic resonance imaging (MRI) of the brain. APOE genotyping was performed only as permitted by patients. The study protocol was approved by the Institutional Review Board (IRB) of each participating hospital (Konyang University, No. 11-15), and written informed consent was obtained from all patients and their caregivers, after a complete study description was given.
In general, we adhered to diagnostic criteria for aMCI defined by Petersen et al.32 and Winblad et al.33 as follows: 1) memory complaints; 2) cognitive impairment (at least −1.0 SD below age- and education-adjusted norms) involving memory and/or ≥1 domain (executive function, language, or visuospatial ability) on standard neuropsychological tests; 3) normal functional activities (informant's report of intact ADL); 4) clinical dementia rating (CDR) = 0.5; and 5) absence of dementia, as defined by Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria. Hemiparesis or clinically evident stroke was grounds for study exclusion, given related physical activity impediments. In addition, we excluded patients with histories of neurologic disorders (e.g., active epilepsy or Parkinson's disease), psychiatric illnesses (e.g., schizophrenia, mental retardation, major depression, or mania), psychotropic medication use, or significant alcohol and/or other substance abuses. Likewise, any candidates whose cognitive deficits were secondary in nature, as indicated by laboratory findings (i.e., complete blood count, blood chemistry, vitamin B12/folate, syphilis serology, or thyroid function tests) were also excluded. We also excluded patients with large territory infarctions/hemorrhage in MRI studies of the brain (screening for organic lesions that affect cognitive impairment), and patients displaying high MRI signal abnormalities related to various conditions (brain tumor, radiation injury, hippocampal sclerosis, or multiple sclerosis).
All subjects with aMCI met the Peterson MCI criteria (Petersen et al., 2000)32 as follows: 1) assistant-corroborated subjective memory impairment; 2) memory lower than expected for age and education of subject (within −1.0 SD below norms), confirmed by Korean Mini-Mental State Examination (K-MMSE) and Shiraz Verbal Learning Test (SVLT), especially 20-min delayed recall scores; and 3) no or very minimal impact of memory deficits on subject activities and CDR scores=0.5.34
Clinical and prospective memory assessments
Cognitive functions were assessed by neuropsychologists using the K-MMSE35 and the Seoul Neuropsychological Screening Battery (SNSB).36 The SNSB addresses five specific cognitive domains: attention, visuospatial abilities, language, verbal/visual memory, and frontal executive functions. The 15-item Geriatric Depression Scale (GDS-15),37 Korean Instrumental Activities of Daily Living (K-IADL)38 or Seoul Instrumental Activities of Daily Living (S-IADL),39 CDR, and CDR Sum of Boxes (CDR-SB) were measured at baseline.
We used the Korean version of the Prospective and Retrospective Memory Questionnaire (PRMQ) (Supplementary Table 1) to assess PM.4041424344 PRMQ is a questionnaire that allows patients to gauge and self-report levels of PM and retrospective memory (RM) operant in their daily lives. It consists of 16 questions (eight each on PM and RM) pertaining to memory type, period, and types of clues. Each item is set to a 5-point scale.
MRI acquisition and WMHs assessment
All patients underwent MRI scans under standard conditions. Imaging performed at each center involved a 3.0T MRI system, referencing anterior-posterior commissure. MRIs were set to ideal parameters. Axial T2, T1, and fluid-attenuated inversion recovery (FLAIR) images were generated at 5-mm thickness without gaps. A neurologist and a radiologist (both on staff at the participating centers) rated degrees of WMHs on FLAIR sequences. In the event of rating disagreements, central committee members ultimately reached consensus determinations. WMH-rating scales were developed by the central committee for the Clinical Research Center for Dementia of South Korea (CREDOS) study, by modifying Fazekas et al.45 and Scheltens et al.46 scales. The broadest diameters of WMHs around lateral ventricles (capping or banding of periventricular areas) and depths of WMHs (especially at centrum semiovale) were evaluated. PVWMHs were rated as P1 (<5 mm), P2 (≥5 mm, <10 mm), or P3 (≥10 mm); and DWMHs were rated as D1 (<10 mm), D2 (≥10 mm and <25 mm), or D3 (≥25 mm). Periventricular and deep ratings were combined to produce overall ischemic ratings (mild, moderate, or severe). Combined D1+P1 (D1P1) and D1+P2 (D1P2) ratings were considered mild. Most other combinations (D2P1, D3P1, D2P2, D3P2, D1P3, and D2P3) were deemed moderate, with D3P3 rated as severe. Inter-rater reliabilities for ratings of PVWMHs (κ=0.595), DWMHs (κ=0.787), and WMHs (κ=0.785) were high, as were intra-rater reliabilities for WMHs ratings (PVWMHs + DWMHs: κ=0.694-0.979). We grouped patients by degree of WMHs as mild, moderate, or severe. A number of studies have already used the same protocol.30474849
Statistical analysis
In patients with aMCI stratified by degree of WMHs, we used a paired t-test to compare PRMQ total scores and sub-scores tabulated at baseline and 3 months later. We similarly compared such scores according to type of WMHs, AChEI use, and APOE genotype. Categorical variables were analyzed using χ2 test or Fisher's exact test, invoking analysis of variance for general characteristics and analysis of covariance for results of neuropsychological testing. The latter was based on ratings of WMHs and status of APOE ε4, once adjusted for age, gender, education, K-MMSE, and CDR-SB, and after investigating multiplicative interaction terms. All computations relied on standard software (SPSS for Windows v20.0; SPSS Inc. [IBM], Chicago, IL, USA), setting statistical significance at p<0.05.
RESULTS
Although 74 participants were registered, only 69 (93.2%) completed the study. One withdrew consent, and four were lost to follow-up. A summary of patient demographics and PRMQ profiles at baseline is shown in Table 1. Patients with WMHs of moderate (vs. mild) degree tended to be older and have higher incidences of hypertension. Otherwise, between-group demographic differences were not significant, and there was no statistical difference in baseline PRMQ profiles. Mean changes in total PRMQ scores at 3 months also differed (mild, 0.2±7.1; moderate, −2.8±7.2), those patients with moderate (vs. mild) degrees of WMHs showing greater decline in PRMQ scores (p=0.032). The same was true of PRMQ PM sub-scores. Patients with moderate (vs. mild) degrees of WMHs demonstrated faster PM decline. However, RM scores of the two groups were not significantly different (Table 2). When further stratified by type of WMHs (DWMHs vs. PVWMHs), PM scores in patients with moderate (vs. mild) degrees of DWMHs showed greater decline. There were no differences in PM among groups stratified by degree of PVWMHs (mild, moderate, or severe) (Table 3), and changes of PRMQ scores in patient groups with mild or moderate degrees of WMHs did not differ significantly in terms of AChEI use or APOE Ɛ4 carrier status (Supplementary Tables 2 and 3).
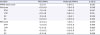
Table 1
Baseline clinical characteristics of patient subsets (mild vs. moderate WMHs)

Continuous variables expressed as mean±standard deviation, categorical variables as number (%).
WMHs: white matter hyperintensities, APOE: apolipoprotein E, K-MMSE: Korean Mini-Mental State Examination, CDR-SB: clinical dementia rating sum of boxes, GDS-SF: 15-item Geriatric Depression Scale, PRMQ: Prospective and Retrospective Memory Questionnaire, PM: prospective memory, STM: short-term memory, LTM: long-term memory, SC: self-cued, EC: environmentally-cued, RM: retrospective memory.
![]()
Table 2
Changes in PRMQ scores of patient subsets at 3 months (vs. baseline)
All values expressed as mean±standard deviation of each score-based slope, reflecting differences between baseline and follow-up data.
PRMQ: Prospective and Retrospective Memory Questionnaire, WMHs: white matter hyperintensities, PRMQ: Prospective and Retrospective Memory Questionnaire, PM: prospective memory, STM: short-term memory, LTM: long-term memory, SC: self-cued, EC: environmentally-cued, RM: retrospective memory.
![]()
Table 3
Changes in PRMQ scores at 3 months (vs. baseline) by type and degree of WMHs

All values expressed as mean±standard deviation of each score-based slope, reflecting differences between baseline and follow-up data.
PRMQ: Prospective and Retrospective Memory Questionnaire, WMHs: white matter hyperintensities, DWMHs: deep white matter hyperintensities, PVWMHs: periventricular white matter hyperintensities, PM: prospective memory, STM: short-term memory, LTM: long-term memory, SC: self-cued, EC: environmentally-cued, RM: retrospective memory.
![]()
DISCUSSION
The aim of this study was to document changes in PRMQ-assessed PM displayed by patients with aMCI 3 months after baseline testing. Our results subsequently indicated significant declines in total and PM scores generated by PRMQ at 3 months in patients with moderate (vs. mild) degrees of WMHs. Similarly, we confirmed that WMHs (especially DWMHs) positively correlated with PM decline, exerting significant negative impact.
As in the present study, previous investigations of WMHs in this setting have regularly demonstrated their negative effects on cognition.505152 WMHs serve to disrupt neuronal connectivity, impairing cognitive function, and PM loss is sustained in the same manner. However, perhaps due to inherent heterogeneity, specific ramifications of PVWMHs and DWMHs have yet to be clarified. The impact of WMHs is known to vary in accord with size, location, and extent of lesions. Some researchers have linked heightened loads of PVWMHs with reduced cognitive function in normal aging adults and in patients with MCI or AD47535455; and longitudinal studies of patients with cognitive dysfunction have suggested a predilection for periventricular WM lesions.52 These findings seem plausible, given that periventricular fiber connections convey long-association, interhemispheric, and long-projection fibers, whereas DWMHs convey relatively short-association fibers involved in specific brain regions.56
Unlike the above studies, other efforts have shown a correlation between DWMHs and cognitive functions,57585960 thus supporting our contention that DWMHs (rather than PVWMHs) are preferentially involved in declining PM. It may be that PVWMHs have diffuse consequences, whereas effects of DWMHs are largely confined to frontal-subcortical circuits. In addition, PM requires higher-level function and is rooted not only in frontal lobe, but also in the temporal lobe, which is chiefly responsible for memory. In contrast to RM, PM has greater bearing on various frontal lobe functions. Thus, by disrupting frontal-subcortical circuits, WMHs (especially extensive DWMHs) promote frontal dysfunction and more rapid progression of PM. As we have shown, the extent of DWMHs seems to correspond with the rapidity of PM decline. Yet, rather than hastily assign more importance to DWMHs or PVWMHs, it is reasonable to conclude that the burden of WMHs is clearly and consistently implicated in loss of PM (rather than RM) experienced by patients with aMCI. Contrary to our expectations, the present analysis yielded no group-wise differences with AChEI use. However, the 3-month time interval stipulated may not have ensured full drug efficacy, and not everyone was prescribed an AChEI, so this comparison may be premature.
The present study has several acknowledged limitations. First, this was a small, hospital-driven study, not a population-based investigation, creating a potential for bias in patient selection and limiting any generalization of our results. Also, we did not collect detailed information on lacunes, again possibly skewing our results. Furthermore, we did not include patients with severe degrees of DWMHs, and the follow-up period was relatively brief. The overall credibility of our findings could be bolstered by addressing such deficiencies.
In summary, WMHs affect PM, and WMHs are involved in greater PM decline, especially if DWMHs are extensive. Therefore, it is important to pay greater attention to the change of PM in aMCI patients with WMHs.
 XML Download
XML Download