

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Early-onset Alzheimer's disease (EOAD) have difficulty in making accurate clinical diagnosis, its patients are more likely to show atypical symptoms such as visual, language, and behavioral abnormalities compared to older Alzheimer's disease (AD) patients with typical memory impairment.1 Recently, several fluorine-18-labeled positron emission tomography (18F PET) tracers have been developed and used to enable pathological diagnosis of AD.1
A 51-year-old female patient visited our dementia clinic with a gradual cognitive decline. The patient could not operate properly due to difficulties in using mobile phone and TV remote control, and could confuse one for the other. She often forgot where she put her clothes or things in general and could not remember her children's birthday. Also, she had already left the company she was working for. Her consciousness was clear and there was no abnormality in cranial nerve examination. Her motor, sensory, and deep tendon reflexes were all normal in limbs.
The patient was a college graduate. She scored 18 points in her Korean version of Mini Mental Status Examination and 2 points in Clinical Dementia Rating. There was no evidence of depression at the short version of the Geriatric Depression Scale. However, severe functional impairment was found during the Korean-Boston Naming Test, language memory, and frontal/executive functions. On the blood test, thyroid function tests, syphilis, vitamin B 12 and folate levels were normal and the apolipoprotein E genotype was 3/3. Magnetic resonance imaging revealed a slight atrophy of the medial temporal lobe.
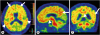
The patient was judged to be a candidate for amyloid PET examination of the amyloid imaging taskforce (AIT).2 The 18F flutemetamol PET was performed and amyloid deposits were observed in various regions of the brain cortex (Fig. 1).
The patient was prescribed donepezil after diagnosis by EOAD.
Clinically, it is difficult to accurately diagnose EOAD because they have atypical clinical characteristics such as vision or speech difficulties, behavioral changes, and difficulty in using the tool.1 In addition, in studies comparing EOAD and late-onset AD, apraxia and visuospatial dysfunction have been reported to be early symptoms of EOAD.3 The exact diagnosis of EOAD is very important considering the different treatment methods and prognosis according to the cause of dementia.
For the 51-year-old female patient, she had difficulties in using the mobile phone and the remote control as well as distinguishing them. Therefore, this could be the early symptom of EOAD as mentioned above. However, due to her age and her progressiveness, the patient and her family could not accept it and wanted more accurate tests. Therefore, amyloid PET test was performed to make a pathological diagnosis. Amyloid PET examination revealed amyloid pathology, confirming EOAD, and patient and her family were cooperating and actively involved in the treatment of AD.
Recently, several 18F PET tracers, including 18F flutemetamol, have been used to allow non-invasive identification of amyloid pathology.1 As a result, these pathological biomarkers are increasingly being used clinically and are included in research criteria for AD. However, the level of amyloid beta is increased not only in AD but also in the elderly. The price is high and there are limitations such as the limited number of institutions that can perform such tests. Therefore, when choosing patients for amyloid PET examinations, it may be advisable to follow the guidance from the AIT.2 In this study, it was concluded that the condition of dementia patients with early age of onset with atypical clinical course was satisfactory.
Although the costs and equipment problems of Amyloid PET testing have not yet been resolved, choosing a candidate carefully according to the guidelines will be a great help for the diagnosis, treatment, and prognosis of AD.
 XML Download
XML Download