

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Numerous studies have reported that the incidence of epilepsy is increasing in the elderly.1234 With advancements in the field of medicine, there is an increase in the survival rate of the elderly who are vulnerable to stroke, head injury, and degenerative brain diseases that can be associated with epilepsy. Epilepsy occurs in the elderly mostly owing to cryptogenic causes. However, one-third of epilepsy incidences can be attributed to symptomatic causes such as stroke, dementia, brain tumor, and head injury.5 Among these causes, various studies have been conducted on the contribution of Alzheimer's disease (AD) to the increasing incidence of epilepsy.6789 Incidence of epilepsy ranges from 1.5% to 64% depending on stages of AD.6 According to a clinical study, the incidence of epilepsy in the AD group is increased 6–10 times compared to that in the control group with the same age range.7 The incidence of epilepsy in patient group aged ≥65 years with neurodegenerative diseases is approximately 10%.9 However, few epidemiological studies on epilepsy have been reported in Asia. In addition, conflicting study results have been reported. Regarding risk factors for the incidence of epilepsy during the progression of AD, United States studies have reported various risk factors, including stages of AD, earlier age at diagnosis of AD, use of antipsychotic drugs, diabetes, and hypertension.10111213 Various studies have reported that stages of AD and earlier age at diagnosis of AD are two crucial risk factors.14 The current study aimed to investigate the correlation between AD and epilepsy by utilizing demographic characteristics (sex and age) and clinical characteristics (such as diabetes and presence or absence of cardiovascular disease) based on the National Health Insurance Service-National Elderly (NHIS-elderly) cohort database.
METHODS
Subjects
The NHIS-elderly cohort database was used as the source of research data comprising eligibility and socio-economic information, hospital-use history, health-checkup results, and medical institution information for 550,000 people, which was 10% of approximately 5.5 million people who were eligible for health insurance and medical aid by the end of December 2002. This study was conducted by using the NHIS-elderly cohort data obtained between 2004 and 2013, referring to all claims data except for non-benefit medical care conducted in South Korea during this period. This study was conducted after obtaining approval from the Institutional Review Board of the National Health Insurance Service Ilsan Hospital.
Diagnosis for the elderly in the cohort data was based on the International Classification of Disease, 10th revision (ICD-10). Research subjects were selected by including cases with Korean Classification Diseases codes G30 and F00 related to AD as claim codes in principal and minor diagnoses, excluding cases with F01 as claim code known to be related to vascular dementia. To select only patients who were initially diagnosed during this study period, patients with AD admitted between 2002 and 2003 were excluded and 4,516 patients who were admitted owing to AD between 2004 and 2006 were defined as new patients. Considering factors such as sex and age for comparative analysis, the control group was selected by 1:5 through propensity score matching method among patients with similar characteristics to the patient group. A total of 19,713 individuals without AD between 2004 and 2006 were assigned into the control group.
This study was conducted to determine the incidence of epilepsy in patients with AD. The criteria for the incidence of epilepsy were defined as patients with diagnosis codes such as G40, G41, R56, and F80 as per the ICD-10 guideline or those who were taking related drugs. Survival time was defined as the time from the first episode of AD to the incidence of epilepsy or the end of the study which was December 31, 2013.
Statistics
Data were analyzed using SAS 9.4 system, version 9.4 (SAS Inc., Cary, NC, USA). The χ2 test was used to identify descriptive statistics and frequency of various factors as well as differences between patient group and control group. To determine the difference of clinical factors according to the presence or absence of AD, a cross-tabulation analysis was performed. Kaplan-Meier survival analysis was performed for the time elapsed from the incidence of AD to the diagnosis of epilepsy. The hazard ratio (HR) was calculated using the Cox proportional hazards model. The 95% confidence interval (CI) and statistical significance of 0.05 were used for validation.
RESULTS
The number of study subjects was 4,516. Subjects had been followed up for a maximum of 10 years until December 31, 2013. During this period, 631 (13.97%) incidences of epilepsy occurred in the AD group and 1,193 (6.05%) people in the control group were diagnosed as having epilepsy, with the AD group showing higher incidence of epilepsy (Fig. 1). The number of patients with diabetes, hypertension, chronic kidney disease (CKD), hyperlipidemia, and tumors was significantly higher in the AD group than that in the control group (Table 1).
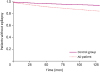 | Fig. 1Comparison of epilepsy occurrence risk between non-AD and AD patients.AD: Alzheimer's disease.
|
Table 1
Demographic and clinical characteristics of control subjects and AD patients
![]()
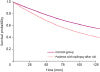
Total risk of incidence of epilepsy was 2.773 (95% CI, 2.515–3.057) times higher in the AD group than that in the control group. Analysis of factors affecting the incidence of epilepsy showed that sex (female) was a factor that lowered the risk of incidence of epilepsy, with a HR of 0.859 (95% CI, 0.782–0.944). Regarding comorbidity that might increase the risk of incidence of epilepsy, the presence of hypertension showed the highest risk (HR, 1.929; 95% CI, 1.742–2.137), followed by hyperlipidemia (HR, 1.855; 95% CI, 1.688–2.040), diabetes (HR, 1.693; 95% CI, 1.544–1.857), and CKD (HR, 1.438; 95% CI, 1.059–1.953). The risk of incidence of epilepsy was 25.5 (95% CI, 19.376–33.560) times higher in patients with tumors than that in those without tumors. However, because the number of patients with tumors was insufficient, the confidence interval was very wide, requiring caution in analysis (Table 2). The risk of death was 1.527 (95% CI, 1.375–1.695) times higher in the AD group than that in the control group (Fig. 2).
Table 2
Risk of occurrence of epilepsy in control subjects and AD patients

![]()
DISCUSSION
This study investigated the risk of incidence of epilepsy in patients with AD by using NHIS-elderly cohort data. Some previous studies have reported that the incidence of epilepsy in patients with AD is rare while some have reported that the incidence is common1516. Recent studies have reported that AD can increase the risk of epilepsy by 6–10 times and that approximately 10% of Alzheimer's patients over 65 years of age have seizures.6 A study conducted in Taiwan in 2015 revealed that 4.7% of patients with AD developed epilepsy and that AD increased the risk of incidence by 1.85 (95% CI, 1.20–2.83).14
The present study showed that the incidence of epilepsy occurred in 631 (13.97%) of 4,516 patients with AD. In addition, the risk of incidence of epilepsy was 2.773 (95% CI, 2.515–3.057) times higher in the AD group than that in the control group considering sex, age, and household income. This value is higher than that reported by a study in Taiwan, suggesting that difference in operational definitions of epilepsy between respective studies could affect results. Rather than diagnosing epilepsy more specifically through electroencephalographic test results, this study defined patients with epilepsy as those with predetermined diagnosis codes. In addition, fluctuations in study results could be largely due to the use of various diagnostic criteria in different countries.
This study revealed that the risk of epilepsy was increased in patients with AD if they were males or had comorbidities such as hypertension, hyperlipidemia, diabetes, and CKD. Some recent studies have reported that stages of AD and earlier age at diagnosis of AD are two crucial risk factors, although various opinions have been reported on other factors such as antipsychotic use, hypertension, diabetes, and cognitive function level.10111213 Despite slight differences in incidence of epilepsy in each study, the incidence of epilepsy has been reported to be slightly higher in males than that in females. This might be because incidences of head injury or stroke are higher in males.1718 Since hypertension, hyperlipidemia, and diabetes are all risk factors for stroke, patients with these comorbid factors might show higher probability of stroke, resulting in higher incidence of epilepsy.
Patients with epilepsy after diagnosis of dementia were found to have higher mortality rate than control group with long-term follow-up observation. Death rate of patients with epilepsy is mostly related to comorbidities (26% for those with tumors, 25% for those with pneumonia, 24% for those with cardiovascular diseases, 12% of seizure-related deaths, 6% of sudden unexplained death in epilepsy, and 3% of accidental death).5 Aspiration pneumonia is more likely to occur with comorbid dementia than those without. The cardiovascular risk factors including hypertension, hyperlipidemia, diabetes and CKD appear to affect the incidence of epilepsy and increase the risk of death.
The purpose of this study was to investigate the incidence of epilepsy among patients with AD in the elderly. This study is significant in that it is the first such study conducted in South Korea with a follow-up period of at least 8 years and a large patient cohort. Although we strived to include as many clinical factors as possible for the correction of data, this study had some limitations. First, this study did not include more sufficient factors such as electroencephalogram findings and environmental factors. Furthermore, because clinical aspects of epilepsy are frequently deviated in patients with dementia, patients or their guardians could not accurately perceive these symptoms. Thus, complementary research methods are required to resolve this issue. In addition, medicines such as depression drugs, acetylcholinesterase inhibitors, and psychiatric drugs that could affect seizures in epilepsy were not considered.
In conclusion, this study showed that patients with AD had a high risk of incidence of epilepsy. In addition to sex (male), comorbidities such as hypertension, hyperlipidemia, diabetes, and CKD also contributed to the increase in the probability of epilepsy incidence. Furthermore, the risk of death was high in patients with AD. This study provides useful insights because data are created based on demographic characteristics (sex and age) and clinical characteristics (such as diabetes and presence or absence of cardiovascular disease) in South Korea by using the NHIS-elderly cohort database. Further studies on mechanisms of epilepsy and AD are required.
 XML Download
XML Download