

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
In selecting antimicrobials, not only the effectiveness but also the possible detrimental effects accompanying antimicrobial treatment should be considered. Timely administration of effective antimicrobials is crucial to clinical outcomes, especially in bloodstream infections (BSIs).12 However, the widespread use of broad-spectrum antimicrobials can lead to unintended consequences such as the emergence of resistance, superinfection by selected pathogenic organisms, and increased hospital costs.34
The spread of resistance and increase in healthcare-associated infections have led to challenges in establishing a treatment strategy for community-onset infections. In the case of gram-negative bacteria, the incidence of infections due to extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae has been increasing in the community,5678 which has made antimicrobial selection more difficult. Specifically, whether to use carbapenems is becoming a major issue.
The widespread use of carbapenems for treatment of community-onset infections should be avoided. There have been concerns about the emergence of carbapenem-resistant Enterobacteriaceae (CRE).910 Furthermore, we do not currently have a highly reliable treatment option for CRE infections.11 The broadness of the antimicrobial spectrum itself could also be a problem. Therefore, guidance is needed to help to determine the necessity of carbapenem use by predicting the presence of infection with ESBL-producing microorganisms.
We aimed to identify the predictors and build a prediction score for community-onset bloodstream infections (CO-BSIs) caused by Escherichia coli and Klebsiella species, which are potential ESBL-producing microorganisms and major pathogens in community-onset gram-negative bacterial infections. The validation process was also performed by applying the score to an independent group of subjects.
METHODS
Study setting
This study was conducted at a university-affiliated referral hospital in a metropolitan area. The number of hospital beds was 900 before April 2013, when it increased to 1,350 beds with the opening of a new building. In this institution, positive blood cultures results are reported to attending physicians and referred to infectious disease specialists through an automated process based on the hospital information system. This automated consultation started in August 2011 and the details of this process are described elsewhere.12
Study subjects
All cases of BSIs identified from January 2012 to December 2015 were reviewed. The BSI was included in the study if 1) the infection was community-onset, 2) the patient was aged ≥ 18 years, and 3) the confirmed pathogen was E. coli or Klebsiella species. If the presence of BSI was established (a blood culture of the BSI was ordered by a physician) within 48 hours of admission, it was considered a CO-BSI. If the BSI occurred in a patient transferred from another hospital, it was not considered a CO-BSI.
The BSI was excluded if it was 1) a polymicrobial or 2) a recurrent BSI occurring in the same patient during the study period. A polymicrobial BSI was defined as the isolation of two or more pathogenic species from the same blood culture set.
Species identification, antimicrobial susceptibility, and ESBL phenotype were tested and evaluated throughout the study period with a VITEK 2 system (bioMérieux, Lyon, France).
Data collection and definitions of variables
To select the candidate predictors of CO-BSIs caused by ESBL-producing E. coli and Klebsiella species (ESBL-BSIs), we referred to previous studies reporting risk factors associated with multi-drug resistance including ESBL.13141516 Prior hospitalization, residency in long-term care facilities, and operation were categorised according to the time sequence. For example, prior hospitalization was divided into three groups: within 90 days, 91 to 180 days, and 181 days to one year of admission. The antimicrobial prescription records within 90 days prior to admission were reviewed. A prescription of beta-lactam or fluoroquinolone for two or more consecutive days was included in the data as a prior course of beta-lactam or fluoroquinolone treatment. The timing and frequency of treatment were also investigated. If the prescription was for the same episode of infection, it was considered a part of a single course rather than an independent course of treatment.
The Charlson comorbidity index (CCI)1718 was calculated as a representative variable of the underlying conditions. The clinical characteristics and outcomes of the BSIs, such as the site of infection, presence of severe sepsis or septic shock, Pitt bacteremia score,19 administration of effective antimicrobials (active in vitro according to susceptibility test findings) within 48 hours from the time of blood cultures, length of stay, and all-cause 30-day mortality were also investigated.
Data management and analysis
Derivation and validation cohorts
The study subjects were divided into derivation and validation cohorts. The derivation cohort contained BSIs identified from 2012 to 2014; the validation cohort contained BSIs from 2015. The derivation cohort was used to identify the predictors and develop a prediction score for ESBL-BSIs, while the validation cohort was used to verify the performance of the prediction score.
Comparing case and control groups
The BSIs of the derivation cohort were classified according to whether the confirmed pathogen was ESBL producing microorganisms (case, ESBL-BSIs) or not (control, non-ESBL-BSIs). To compare the clinical characteristics of the two groups, chi-square or Fisher's exact tests were used for categorical variables. Continuous variables were presented as median values with interquartile range (IQR) and their differences were evaluated using Mann-Whitney median tests.
Identifying the predictors of ESBL-BSIs
To identify the predictors of ESBL-BSIs, a logistic regression analysis was performed. Variables with P < 0.10 in the univariate analysis were used to construct a multivariate regression model. For possible overlapping variables, such as an individual underlying disease and CCI, we constructed separate models. After stepwise backward elimination, variables with P < 0.05 were included in the final model.
Building a prediction score for ESBL-BSIs
The prediction score for ESBL-BSIs was built based on the final multivariate regression model and its regression coefficients.202122 The point for each variable was assigned according to the ratio between the coefficients. The overall risk was expressed as a sum of the points. The discriminative power of the score was evaluated by area under the receiver operating characteristics (ROC) curve (AUC) analysis. The calibration was assessed with the Hosmer-Lemeshow goodness-of-fit test.
Validation
The prediction score was validated by applying the score to the validation cohort. ROC curve analysis was performed, and the AUC was calculated.
Identifying the risk factors for mortality
A log-rank test was performed to compare mortality between ESBL-BSIs and non-ESBL-BSIs. Cox proportional hazards regression was performed to identify the risk factors for mortality. Both derivation and validation cohorts were included in this analysis. To reflect the influence of site of infection, respiratory tract and intraabdominal infection were classified as a high-risk source of infection.2324 Like in the logistic regression, variables with P < 0.10 in the univariate analysis were included in the multivariate model, and separate models were constructed for the possible overlapping variables in order to avoid multicollinearity.
RESULTS
Microbiology, demographics, and clinical characteristics
According to the enrolment criteria, we included 886 CO-BSIs caused by E. coli and Klebsiella species from 2012 to 2015. Of these, 594 BSIs were included in the derivation cohort (E. coli: n = 419, 70.5%; Klebsiella species: n = 175, 29.5%).
In the derivation cohort, 23.6% were ESBL-BSIs; of all cases, 27.2% of E. coli and 14.9% of Klebsiella species were ESBL-BSIs. The ciprofloxacin resistance rate was 30.8% (38.7% in E. coli, 21.0% in Klebsiella species). The rate was higher in ESBL-BSIs than that in non-ESBL-BSIs (76.4% vs. 16.7%, P < 0.001). There were no BSIs caused by carbapenem-resistant Enterobacteriaceae. The baseline patient demographics and clinical characteristics between ESBL-BSIs and non-ESBL-BSIs are compared in Table 1.
Table 1
Comparison of baseline demographics and clinical characteristics between CO-BSIs caused by ESBL-producing E. and Klebsiella species (ESBL-BSIs) and non-ESBL-BSIs

Values are presented as number of patients (%) or median (interquartile range).
CO-BSI = community-onset bloodstream infection, ESBL = extended-spectrum beta-lactamase, BSI = bloodstream infection, CCI = Charlson comorbidity index, IV = intravenous, SSTI = skin and soft tissue infection, BJI = bone and joint infection, ICU = intensive care unit.
aIdentification of ESBL-producing microorganisms from any clinical culture within 1 year.
![]()
Predictors of ESBL-BSIs and logistic regression analysis
The independent predictors of ESBL-BSIs in multivariate analysis were as follows (Table 2): identification of ESBL-producing microorganisms from any clinical culture within one year of admission (adjusted odds ratio [aOR], 7.75; 95% confidence interval [CI], 3.15–10.07; P < 0.001), beta-lactam or fluoroquinolone treatment within 30 days with 2 or more courses within 90 days (aOR, 6.82; 95% CI, 2.31–20.16; P < 0.001); with 1 course within 90 days (aOR, 2.89; 95% CI, 1.06–6.32; P = 0.037), hospitalization within one year (aOR, 2.48; 95% CI, 1.55–3.96; P < 0.001), and the presence of an indwelling urinary catheter at the time of admission (aOR, 2.34; 95% CI, 1.04–5.24; P = 0.039). To make a more parsimonious model, hospitalization within one year was included in the final model instead of the divided time periods. Supplementary Table 1 shows results of the regression analysis with the time periods.
Table 2
Results of univariate and multivariate logistic regression analyses for the predictors of CO-BSIs caused by ESBL-producing E. coli and Klebsiella species

CO-BSI = community-onset bloodstream infection, ESBL= extended-spectrum beta-lactamase, BSI = bloodstream infection, CCI = Charlson comorbidity index, IV = intravenous.
aIdentification of ESBL-producing microorganisms from any clinical culture within 1 year.
![]()
Building a prediction score for ESBL-BSIs
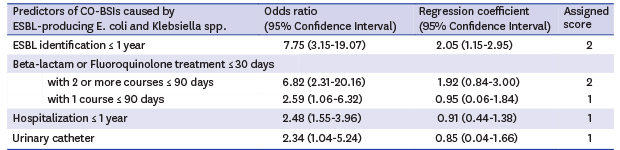
The prediction score was built using the regression coefficients of the final multivariate regression model (Table 3). Each regression coefficient was divided by the lowest coefficient in the final model, which was the coefficient of the presence of an indwelling urinary catheter. Two points were assigned for ESBL identification within one year and beta-lactam or fluoroquinolone treatment within 30 days with 2 or more courses within 90 days. One point was assigned for beta-lactam or fluoroquinolone treatment within 30 days with 1 course within 90 days, hospitalization within one year, and the presence of an indwelling urinary catheter, respectively. A total of 190 BSIs had a score of 1 (190/594, 32.0%), 32 (5.4%) had a score of 2, 34 (5.7%) had a score of 3, 17 (2.9%) had a score of 4 or more.
Table 3
Regression coefficients from multivariate logistic regression and clinical prediction score for CO-BSIs caused by ESBL-producing E. coli and Klebsiella species
CO-BSI = community-onset bloodstream infection, ESBL = extended-spectrum beta-lactamase.
aIdentification of ESBL-producing microorganisms from any clinical culture within 1 year.
![]()
The AUC of the score was 0.72 (95% CI, 0.68–0.77) (Fig. 1). The P value for the Hosmer-Lemeshow test was 0.60. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for each cutoff are shown in Table 4; The PPV was 66.3% at a cutoff of 2, 76.5% at 3, and 100% at 4 or more; The NPV was 83.4% at a cutoff of 2, 81.4% at 3, and 78.7% at 4.
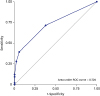 | Fig. 1ROC curve of the clinical prediction score for community-onset bloodstream infections caused by extended-spectrum beta-lactamase-producing E. coli and Klebsiella species.ROC = receiver operating characteristics.
|
Table 4
Receiver operating characteristics cutoff values of the clinical prediction score for CO-BSIs caused by ESBL-producing E. coli and Klebsiella species

CO-BSI = community-onset bloodstream infection, ESBL = extended-spectrum beta-lactamase, CI = confidence interval, PPV = positive predictive value, NPV = negative predictive value.
![]()
Predictors of ESBL-BSIs in E. coli subgroup
When the subjects were confined to BSIs caused by E. coli which was the dominant species in the study, the independent predictors of ESBL-BSIs were as follows: identification of ESBL-producing microorganisms within one year (aOR, 7.71; 95% CI, 2.60–22.95; P < 0.001), beta-lactam or fluoroquinolone treatment within 30 days with 2 or more courses within 90 days (aOR, 5.91; 95% CI, 1.50–23.36; P < 0.001); hospitalization within one year (aOR, 2.30; 95% CI, 1.38–3.84; P < 0.001). The AUC was calculated as 0.703. The detailed results are shown in Supplementary Table 2.
Validation
The validation cohort included 292 BSIs (E. coli: n = 200, 68.5%; Klebsiella species: n = 92, 31.5%). The proportion of ESBL-BSIs was 24.3% (28.0% in E. coli, 16.3% in Klebsiella species). The rate of ciprofloxacin resistance was 29.1% (35.5% in E. coli, 15.2% in Klebsiella species). The rate was higher in ESBL-BSIs than that in non-ESBL-BSIs (73.2% vs. 14.9%; P < 0.001). There were no BSIs caused by carbapenem-resistant Enterobacteriaceae.
The same variables as the derivation cohort were investigated (Supplementary Table 3). In the validation cohort, patients with a history of residency in long-term care facilities were more common (6.9% vs. 3.7%; P = 0.038), and the incidence of urinary tract infection was higher (45.6% vs. 35.9%; P = 0.005). Otherwise, there were no significant differences in demographics and clinical characteristics between the two cohorts including the length of stay and all-cause 30-day mortality rate.
The preformed prediction score was applied to the validation cohort. The calculated AUC was 0.70 (95% CI, 0.63–0.77). The sensitivity, specificity, PPV, and NPV for each cutoff were similar to those of the derivation cohort (Supplementary Table 4).
Clinical outcomes of CO-BSIs caused by E. coli and Klebsiella species
Among the 886 BSIs from 2012 to 2015, the median length of stay was significantly longer in ESBL-BSIs than that in non-ESBL-BSIs (15 days [IQR, 10–24] vs. 10 days [IQR, 7–16]; P < 0.001). The log-rank test revealed that there was no significant difference in all-cause 30-day mortality rates between the two groups (8.5% vs. 5.6%; P = 0.131).
Cox proportional hazards regression analysis showed that a high-risk source (adjusted hazard ratio [aHR], 3.79; 95% CI, 2.22–6.47; P < 0.001), Pitt bacteremia score ≥ 3 (aHR, 3.49; 95% CI, 2.07–5.89; P < 0.001), and CCI ≥ 3 (aHR, 2.08; 95% CI, 1.23–3.54; P = 0.007) were independent risk factors of mortality (Supplementary Table 5). ESBL-BSIs (unadjusted HR, 1.52; 95% CI, 0.87–2.67; P = 0.141) and the administration of effective antimicrobials within 48 hours (unadjusted HR, 0.72; 95% CI, 0.38–1.36; P = 0.306) had no significant effect on mortality.
DISCUSSION
This study identified the predictors of CO-BSIs caused by ESBL-producing E. coli and Klebsiella species and suggested a simple prediction score. It also showed the possibility of the extension of the results through validation. The significant advantage of this score is that it consists of easily obtainable clinical parameters, including 1) identification of ESBL-producing microorganisms within one year, 2) beta-lactam or fluoroquinolone treatment within 30 days, 3) hospitalization within one year, 4) presence of an indwelling urinary catheter at the time of admission. The ease of calculation is another advantage of this score.
The previous identification of ESBL-producing microorganisms within one year was the most important predictor of ESBL-BSIs in our study. Several studies have also reported the importance of prior culture positivity.162526 To investigate the previous identification history, we reviewed the medical records and test results for the previous year. However, we could not reflect the time difference between the onset of BSI and the prior identification because there were not enough subjects for this classification. Considering that the fecal carriage of ESBL-producing microorganisms persisted in over one-third of patients after one year of follow-up,2728 more extended time of investigation may be needed regarding this issue.
Prior antimicrobial treatment within 30 days was also a predictor of ESBL-BSIs. Several studies have shown that previous exposure to beta-lactam or fluoroquinolone is associated with infections due to ESBL-producing microorganisms.131415 In our study, both the timing and frequency of antimicrobial treatment were considered when building the multivariate model. The risk of ESBL-BSIs was higher in patients receiving antimicrobial treatment more recently and more frequently, which means overall antimicrobial pressure is important. This increased risk may also have been due to the intensity of medical use rather than the use of antimicrobials. Nevertheless, our finding implies that various factors, such as timing, frequency, dose and/or type of antimicrobials should be considered to evaluate the association between antimicrobial exposure and the risk of infections due to multidrug-resistant microorganisms.
The other predictors of ESBL-BISs included prior hospitalization within one year and the presence of an indwelling urinary catheter. To evaluate the effect of prior hospitalization, the study subjects were classified according to the time difference between the onset of BSI and the prior hospitalization. Unlike our expectation, the difference between the time periods was not significant. Several variables with a period of 30 or 90 days could have influenced these findings, but no significant statistical interaction between the variables was detected. Previous studies have shown that the presence of prosthesis is associated with infections due to ESBL-producing microorganisms.1314 The presence of an indwelling urinary catheter was an independent predictor in our study; however, the fact that the prevalence of urinary tract infection was high should be considered.
In this population, the risk factors for 30-day mortality were 1) high-risk source, high CCI (≥ 3), and 3) high Pitt bacteremia score (≥ 3). ESBL association and the administration of effective antimicrobials had no significant impact on the 30-day mortality. In previous studies, the impact of ESBL association varied especially when adjusted by confounding variables, and it had been suggested that the appropriateness of initial antimicrobials might be the key mediator.29 The association between the initial administration of antimicrobials and mortality was more evident in the subjects with severe sepsis, septic shock, or high-risk source of bacteremia.243031 The lack of association between initial administration of antimicrobials and mortality in the present study is presumably due to the high proportion of low-risk infections such as urinary tract and hepatobiliary infections and the low proportion of bacteremia with severe sepsis or septic shock. Furthermore, the mortality rate was not significantly high in the study subjects. All of the aforementioned features are common in community-onset infections, even though a considerable number of healthcare-associated infections were included in the study. Additionally, the high proportion of elderly patients with comorbidities might have influenced the overall results.
Although AUC analysis showed decent values of AUC in the derivation and validation cohorts, the practical values of its results are limited considering the specificity and sensitivity. Particularly, low specificity was problematic at cutoff 1 (61.9%), while low sensitivity was problematic at cutoffs 2 (39.3%) and 3 (27.9%). Thus, a stratified approach might be needed to promote the appropriate use of antimicrobials using the prediction rules. One of the main purposes of the Cox regression analysis was to establish the basis for the stratified approach in the study population. For example, cutoffs more than 1 may be considered in the presence of high Pitt bacteremia scores, high CCIs, and a high-risk source. In the absence of these risk factors, cutoffs more than 2 might be appropriate. The cutoffs of the prediction score can be set differently depending on the circumstances including the clinical setting of the infection, overall resistance profile in the area, antimicrobial prescription behavior in the hospital, and desired goals.
These results should be applied to other populations cautiously. Firstly, the study subjects were confined to those with E. coli and Klebsiella species infections, although the potential subjects of this study were those affected by community-onset bloodstream infections caused by Enterobacteriaceae. We excluded Enterobacteriaceae other than E. coli and Klebsiella species from the analyses because of the concerns over increasing the heterogeneity and the ambiguity in defining ESBL production or 3rd generation cephalosporin resistance. The number of cases with infections caused by species other than E. coli and Klebsiella species was relatively small, and it was not possible to formulate clear criteria on which species could be included or excluded. When the study subjects were confined to only those with E. coli infections, the impact of the presence of indwelling urinary catheter and recent use of antimicrobials reduced relatively. Since the primary aim of the present study was to make prediction rules which can be used clinically, we concluded that the multivariate model represented the characteristics of the study subjects better when it included both E. coli and Klebsiella species. Thus, E. coli and Klebsiella species, the two dominant pathogens in community-onset gram-negative bacterial infections, were selected as the study subjects.
Secondly, the study was performed at a single institution. The institution is located in a city adjacent to the capital city of the country, and we presumed that it has the dual characteristics of a referral center as well as a community-based hospital. Moreover, there are several long-term care facilities in the same area. Given the universal aging and the increase in healthcare-associated infections, we considered the patients of the institution to be good candidates to evaluate the risks of community-onset infections associated with multidrug-resistant pathogens. Nevertheless, the results are limited and should be interpreted cautiously because the overall study setting cannot represent the general circumstances. The limitation of this study as a single center one may also weaken the strength of the validation, although it was performed on an independent group of subjects. In the validation cohort, residency in long-term care facilities and urinary tract infections were more frequent. It might have been possible that the number of local patients increased first during the expansion of the institution. Conversely, these differences between the two cohorts and the results of validation may imply that the results of the study can be applied to subjects in different conditions.
Finally, as this study was performed retrospectively, the clinical setting at the time point of empirical treatment was not sufficiently reflected. A prospective approach might be needed, especially for the process of validation. Before performing a study, the inclusion criteria for the subjects and the variables to be evaluated should be thoroughly reviewed. Although several studies have been conducted to identify the risks due to the infections by multidrug-resistant pathogens, the details of materials and methods are quite different among the studies. In the current study, some information, including whether the patient was a resident of a long-term care facility, was recorded in preformed text format which had been developed for clinical purposes. We expect that the details of our study design and concepts will provide new perspectives for future studies.
The boundary between community-acquired and healthcare-associated infections has become unclear with the increase in the elderly population and the use of medical care. Antimicrobial resistance circulates bidirectionally between the community and medical facilities, and the selection of appropriate antimicrobials is increasingly more difficult. The results of the present study suggest a simple and easy-to-use scoring system to predict CO-BSIs caused by ESBL-producing E. coli and Klebsiella species. It may be difficult to make a generalized guideline or prediction score reflecting various local factors, but we expect our experience will help build a strategic approach to promote appropriate use of antimicrobials for the treatment of community-onset infections.
 XML Download
XML Download