

 PDF
PDF Citation
Citation Print
Print



Although the evidence linking humidifier disinfectant-associated lung injury (HDLI) and exposure to humidifier disinfectants (HDs) containing 5-chloro-2-methyl-4-isothiazolin-3-one (CMIT)/2-methyl-4-isothiazolin-3-one (MIT) alone is lacking in animal studies, this disorder has been clinically confirmed in several human cases in which HD products containing a mixture of CMIT/MIT had been used in the home.1 We here describe the pathologic findings of an HDLI case with CMIT/MIT.
A previously healthy 26-month-old girl was transferred to our hospital with a 3-week history of progressive respiratory symptoms including cough, sputum, and dyspnea. She was continually exposed to 5-chloro-2-methyl-4-isothiazolin-3-one (CMIT)/2-methyl-4-isothiazolin-3-one (MIT) alone for 12 months in total (between 11 and 25 months of age), with an interlude during the summer months. The distance between her and the humidifier was less than 50 cm and the humidifier output was directed towards her nose and mouth. The airborne density was estimated to be 1.65 μg/m3.2
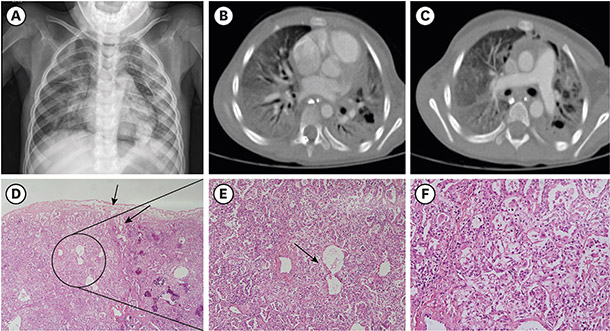
Three weeks before her admission to another hospital, she developed coughing and mild fever and was treated with cold medicine. She developed dyspnea and tachypnea about 2 weeks after these initial symptoms which became progressively worse. She showed desaturation (SaO2 80% at room air) and respiratory difficulties at the time of her prior admission. Chest radiography revealed consolidation in both lung fields and pneumomediastinum (Fig. 1A). Her respiratory function deteriorated and she developed acute respiratory distress syndrome (ARDS) two days after admission. She was then intubated and mechanically ventilated. Nevertheless, her oxygen saturation was not maintained and the clinical symptoms and radiologic findings worsened. She was transferred to our hospital on hospitalization day 3 (June 7, 2006).
She had a resulting SaO2 of 77% with a PaO2 of 47 mmHg (PaO2/FiO2 = 47) and a PaCO2 of 59 mmHg on arterial blood gas. Respiratory virus, sputum and blood cultures were all negative. Serologic testing for Epstein-Barr virus and cytomegalovirus were also negative. Her chest computed tomography revealed diffuse ground glass opacity with pulmonary interstitial emphysema, multifocal consolidations in both lung fields and pneumomediastinum (Fig. 1B and C).
On the third day of hospitalization at our clinic, lung biopsy and histological examination of the superior segment of the left lower lung revealed sparing of the subpleural and paraseptal parenchyma, peribronchiolor alveolar damage with centrilobular distribution, and interstitial fibroblast proliferation (Fig. 1D-F). The patient's condition deteriorated with repeated air leakage and lung fibrosis and she died on hospitalization day 95, despite intravenous steroid treatment, high-dose immunoglobulin treatment, antibiotics, and mechanical ventilation.
All of the reported histopathologic findings for HDLI are for cases exposed to polyhexamethylene guanidine (PHMG)/oligo (2-[2-ethoxy] ethoxyethyl) quanidinium chloride (PGH) alone or mixed with CMIT/MIT. Histopathological specimens of HDLI show a bronchiolocentric, temporally homogenous acute lung injury pattern, with sparing of the subpleural and peripheral alveolar areas.34 Most cases of HDLI exhibit bronchiolar destruction consistent with the inhalation of toxic material. These bronchiolar lesions are characterized by epithelial sloughing and replacement with flattened regenerating cells, mild to severe subepithelial fibroblastic proliferation resulting in bronchiolar obliteration, and varying degrees of peribronchiolar fibrosis.
CMIT/MIT use is far lower than PHMG/PGH use among registered HDLI patients.2 CMIT/MIT was known to be less toxic than PHMG/PGH. The incidence of HDLI can be related to the toxicity of the disinfectant in different HD products. However, this case report demonstrating HDLI pathology proved that CMIT/MIT can also cause pathologically similar lung injury due to PHMG/PGH.
However, this is the first case that the clinical course, imaging, and pathologic findings of HDLI exposed to CMIT/MIT alone are similar to those of PHMG/PGH.
The authors obtained approval from the Institutional Review Board (IRB) of Asan Medical Center (2018-1406), and informed consent was waived by the IRB.

 XML Download
XML Download