

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Mucormycosis is an invasive, fungoid disease caused by rhizopus, mucor or other fungoids belonging to phycomycetes group. Although it mostly occurs in patients with diabetes through opportunistic infections, patients with impaired immune functions or normal people may be affected by the disease in rare cases. Its mortality rate is high due to its rapid and foudroyant progression. Mucormycosis can invade several organs, and can emerge in the form of a paranasal sinusitis in the area of otolaryngology as the patient inhales the mucor in the air. The mucor, attached to mucous membrane of paranasal sinus, primarily causes paranasal sinusitis and orbital inflammation. In addition, mucormycosis's high invasiveness with respect to blood vessels and tissues causes thrombosis in the arteries and veins, and leads to the easy invasion of surrounding nerves; and particularly, it can invade the optic nerve, internal carotid artery, cavernous sinus, ocular motor nerve, and others, which are anatomically adjacent to the sphenoid sinus, thus causing severe complications such as cavernous sinus syndrome and orbital apex syndrome. The authors have identified the rapidly-progressing loss of vision and successive occurrence of multiple cerebral artery occlusions in patients with cavernous sinus thrombosis caused by mucormycosis of the sphenoid sinus. While there have been reported overseas cases where mucormycosis caused cerebral artery occlusion or cerebral infarction,1 no cases have been reported in Korea. In that sense, this paper is intended to introduce such cases.
CASE
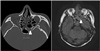
A 54-year-old man, suffering from severe headache that started 2 weeks previously, visited the department of neurology at another hospital, and then underwent brain magnetic resonance imaging (MRI) and computed tomography (CT). The imaging tests showed left sphenoid sinus lesion, but other abnormalities that suggested cerebral lesion were not found (Fig. 1).
It was concluded that the headache was a secondary headache caused by paranasal sinusitis, and endoscopic sinus surgery was scheduled to be performed under general anesthesia at the ENT department of the same hospital. The blood tests of the patient prior to the surgery revealed that his blood sugar was somewhat high, but additional tests were not conducted because the patient said that he had no medical history related to diabetes. According to operative findings, local fungal sinusitis was suspected, and the antifungal agent (Ambisone® 50mg, IV QD) was administered, in consideration of the potential for postoperative invasiveness progression. In addition, vancomycin (Hanomycin® 500mg, IV BID) was also used because methicillin-resistant staphylococcus was found in the rhinorrhea.
Three days after the surgery, symptoms occurred, including left ocular motor dysfunction, decreased visual acuity, and ophthalmoplegia in the lower orbital area. Although a steroid (Solumedrol® 125mg, IV QD) was administered to address the neurologic symptoms in the left eye, such as decreased visual acuity and ocular motor dysfunction, these symptoms continued to worsen. As a result, the patient was transferred to this hospital.
At that time, headache was the severest symptom among others. It was accompanied by a dull pain that persisted and tightened around the left ocular area and the left parietal area. The visual acuity showed finger counting, but ocular movement showed complete ophthalmoplegia, which was considered to be related to the oculomotor nerve, trochlear nerve, and abducens nerve. In addition, the patient complained of ophthalmoplegia in the left lower orbital area, which suggested that the maxillary branch of the trigeminal nerve was also invaded (Fig. 2A). The findings of the nasal endoscopy showed lesion and crusta, suspected as fungal hyphae, along the external wall of the left ethmoidal sinus; and a small amount of purulent discharge and granulation tissue were observed in the sphenoidal sinus. In the biopsy on the lesion site which the patient underwent at the outpatient department, the right-angled branched hyphae were observed. As a result, the patient was diagnosed with cavernous sinus syndrome caused by mucormycosis and mucormycosis (Fig. 3).
The blood test revealed that the WBC and CRP levels had increased to 10,000 /ul and 6.25 mg/dl respectively, and the urine test showed an increase in glucose to 3 +. According to additional tests, blood sugar and glycated hemoglobin after eight hour fasting were increased to 252 mg/dl and 10% respectively, indicating that uncontrolled diabetes had not been recognized for a long time. Thus, joint treatment was immediately carried out with the department of endocrinology, and the sugar was controlled by focusing on insulin therapy rather than oral agents due to the risk of nephrotoxicity and hepatotoxicity.
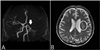
To re-evaluate the patient's condition, imaging testing was performed. The paranasal sinus CT scan showed soft tissue density along with the site of previous surgery and heterogenous contrast enhancement around the orbital apex; the T1 and T2 imaging in the brain MRI revealed that in the pterygopalatine fossa and orbital apex, the lesion site was observed with low signal intensity, and the occlusion of the left internal carotid artery was confirmed (Fig. 4).
The antibiotic test was performed again by continuously administering vancomycin (Vancocin® 1g, IV BID) and aseptically collecting rhinorrhea according to the findings of fungus identification of the previous hospital. As a result, methicillin-resistant staphylococcus was also identified. Although the antifungal agent (Fungizone® 50mg, IV QD) and the high-dose steroid (Methysol® 125mg, IV BID) continued to be also administered, symptoms such as ophthalmoplegia, loss of vision, and headache were not improved. In particular, the patient showed a complete loss of vision as the decreased visual acuity continued to progress. On the fifth day of hospital visits, thus, he underwent the revision surgery to remove the residual lesion in the ethmoidal sinus and sphenoid sinus and decompress orbital and optic nerves. First, the granulation tissue and sphacelus were removed from the inner wall of the left orbit and the left sphenoid sinus. The optic nerve decompression was performed by removing and grinding the bone fragments of the superolateral sphenoid sinus and the external wall of ethmoidal sinus to the maximum along with the moving path of left optic nerve. The absorbable material (Surgicel®) was applied to prevent bleeding, and another packing was not carried out (Fig. 5).
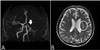
The brain MRI and the MR angiography, taken to monitor the patient's status on the first day of surgery, showed the occlusion of the left middle cerebral artery and left anterior cerebral artery as well as the occlusion of the internal carotid artery, already confirmed; and the cerebral infarction in left middle cerebral artery. Although dysarthria or quadriplegia caused by cerebral artery infarction was not found, the patient was transferred to the department of neurology to treat him and monitor his status (Fig. 6). The antithrombotic and antilipid agents (Plavix® 75mg, Lipitor® 80mg) were additionally administered along with antibiotics and antifungal agent, after he was transferred to the department of neurology.
According to the findings of the postoperative nasal endoscopy, mucor and hyphae were not observed; abnormalities were also not found in the site of orbital decompression; and the headache disappeared, but the left ocular motor dysfunction, the loss of vision, and the hypoesthesia in the left isthmus still persisted. Six months after the revision surgery, the loss of vision still persisted, but the ocular motor dysfunction and ptosis were partially recovered (Fig. 2B).
DISCUSSION
Mucormycosis is a rare disease that occurs through opportunistic infections in patients with impaired immune function who mainly have diabetes, hematologic malignancies, or suffer from chronic alcoholism; in particular, about 70% of mucormycosis patients are reported to have uncontrolled diabetes.23 Mucormycosis divides into five major types: pulmonary type, dermal type, cerebral type, gastrointestinal type, and systemic disseminated type. And cerebral mucormycosis can be divided again into the rhino-orbito-cerebral type with a bad prognosis and the rhino-paranasal sinus type showing satisfactory progress.4 In particular, the rhino-orbito-cerebral type exhibits rapid deterioration and high mortality. It occurs as a result of tissue invasion of the mucor aspirated through the nasal cavity.5 If it becomes morbid in the form of sphenoid sinus lesion, it may cause complications in the anatomically adjacent cavernous sinus. Cavernous sinus syndrome collectively refers to neurological symptoms or thrombosis in lesions around cavernous sinus. Its most common cause is tumors (30%) and infection, deformity and trauma can also be the cause of the disease.6 It may cause neurological abnormalities by affecting the ocular branches of maxillary nerve and maxillary branches, and invades blood vessels and lymph nodes and, particularly, pierces the walls of the arteries and causes thrombosis, leading to cerebral infarction. In addition, the intracranial invasion may cause encephalitis, cerebral hemorrhage and, in severe cases, death.7
The initial symptom of cavernous sinus syndrome may be headache. Other symptoms include pains in the posterior ocular segment due to the invasion to ocular branches of trigeminal nerves,; systemic symptoms occur such as fever or nausea, vomiting, ocular motor dysfunction, exophthalmos, and loss of vision.8
Mucormycosis of the sphenoid sinus, as in this present case, is not easy to access through the endoscopic examination because of the location of lesions, which can delay its diagnosis. In addition, invasion to cavernous sinus may lead to fatal complications. In that sense, rapid diagnosis is a very important factor in the progress of treatment and the prognosis. Although imaging examinations such as computed tomography (CT) and magnetic resonance images (MRI) can provide findings regarding the status of paranasal sinus and orbital apex, cavernous sinus, internal carotid artery or cerebral artery, its definite diagnosis is made through a biopsy.
To be specific, the definite diagnosis is made by identifying the non-septated, right-angled branched hyphae of irregular shape using the Grocott's Methenamine Silver-Periodic Acid Schiff or Hematoxylin & Eosin staining of the lesion tissues.9
Prior to the treatment for mucormycosis, if the patient is suffering from lowered immune function, it is essential to control underlying diseases.10 Drug therapy and surgical treatment may be considered for treatment. Drug therapy is carried out centering on antifungal agents, especially Amphotericin B. High doses (1.0 to 1.5 mg/kg/day) are recommended to prevent complications and their progress, and nephrotoxicity must be taken into consideration.1112 Surgical treatment is based on aggressive and extensive resection of necrotic tissues, and all lesions should be removed until bleeding tissues are identified.
As the disease worsens over a few days or even a few hours, predicting its progress is difficult and complications can be fatal. Therefore, even total maxillectomy or eye enucleation should be actively considered if the need arises according to the lesion's location or the surgeon's judgment.13 In this case, the revision surgery was performed for orbital decompression as a complete loss of vision was confirmed during the monitoring period when the mucormycosis treatment was carried out accompanied by diabetes examination and control through joint treatment with the department of endocrinology. Other treatments can include hyperbaric oxygen therapy and the administration of a blood coagulation inhibitor. However, despite the advancement of therapy methods, the mortality rate of rhino-orbito-cerebral mucormycosis is still as high as 20 to 50 %.1014
In this case, cavernous sinus syndrome occurred after the endoscopic sinus surgery for mucormycosis of the sphenoid sinus. It rapidly worsened within a few days after the first operation. Currently, the patient still continues to show ocular motor dysfunction, loss of vision and ophthalmoplegia in the lower orbital area. However, it is believed that a relatively early diagnosis and a wide range of surgical interventions helped prevent a fatal outcome and ensure partial recovery of ocular movement. In general, the use of steroids in treatment for invasive mucormycosis is contraindicated because it can accelerate the progression of mucormycosis; however, in this case, steroids were unavoidably administered to decompress optic nerves as the patient experienced rapid loss of vision.
The postoperative cerebral artery infarction is thought to have been caused by thrombosis due to mucormycosis invasion to the left internal carotid artery during the endoscopic sinus surgery or by the fungus itself that acted as an embolus in the middle cerebral artery. Therefore, antithrombotic and antilipid agents are being administered to the patient who is under observation.
Several cases of orbital apex syndrome or cavernous sinus syndrome caused by cerebral mucormycosis have been reported. However, since no cerebral artery infarction caused by thrombosis accompanying the disease has been reported in Korea, this case is being introduced with a review of the literature.



 XML Download
XML Download