

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Peripheral artery dissection occurs most commonly in relation to aortic dissection, but spontaneous peripheral artery dissection which arises without the involvement of aortic dissection has been very rarely reported.1 The causes of this disease include Marfan syndrome, pregnancy and fibromuscular dysplasia among others. Exercise that can cause trauma and apply a persistent and intense external force to the body has also been reported to cause spontaneous iliac artery dissection.23
The authors have treated spontaneous external iliac artery dissection in a male patient with no history of vascular diseases including aortic diseases or trauma with percutaneous stenting. The case is thus reported here.
CASE
A 50-year-old man visited the urology department of the authors' hospital with left back pain that started two weeks ago. The patient had smoked for 30 years. He had no unusual history of cardiovascular diseases and connective tissue diseases, with the exception of having undergone excision of a lipoma of the left lower scapula seven years ago. He had no unusual family history, either. At the time of the visit, the patient had acute pain and complained of left flank pain. His vital signs were as follows: blood pressure 110/70 mmHg, pulse 120 times/minute, respiratory rate 20 times/minute and body temperature 36.2 ℃. When auscultated on the chest, the patient had normal pulmonary and cardiac sounds while when palpitated on the abdomen, he complained of tenderness over the left upper abdomen and left costovertebral angle. No specific findings were observed in the bilateral lower extremities.
At the time of the visit, the patient's peripheral blood test results were as follows: leukocyte 11,070/mm3 (neutrophil 57.6%, lymphocyte 32.3%, eosinophil 1.05%), hemoglobin 13.2g/dL and platelet 241,000/mm3. The serum biochemical test results were as follows: albumin 3.9 g/dl, total bilirubin 0.19 mg/dL, direct bilirubin 0.06 mg/dl, AST 13 IU/L, ALT 11 IU/L, ALP 262 IU/L, prothrombin time 10.5 sec, PT INR 0.99 (normal range: 0.85–1.15), total cholesterol 177 mg/dl, HDL 32 mg/dl, LDL 97 mg/dl, TG 533 mg/dl, Troponin I 0.1 ng/ml (normal range: 0–0.3), CK-MB 0.83 ng/ml (normal range: 0–4.87), D-dimer 545.77 ng/ml (normal range: 0–500), blood urea nitrogen 19.2 mg/dl, creatinine 1.8 mg/dl, uric acid 4.2 mg/dl, LDL 264 and CRP 0.65 mg/dl. Other serum electrolyte and urine tests showed no specific findings and α-1-Antitrypsin and ANCA (anti-neutrophil cytoplasmic antibody) were not checked.
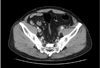
There was no evidence of urinary stone in a simple urinary tract x-ray. An abdominal computed tomography (CT) scan revealed a mass lesion over the upper left psoas muscle and left hydronephrosis. So a contrast-enhanced CT scan was also performed. As a result, features of dissection on the left external iliac artery origin accompanying a hematoma and left hydronephrosis due to the compression of the hematoma were found (Fig. 1); therefore, this case was transferred to the cardiopulmonary department, where an ABI (ankle brachial index) test and transthoracic echocardiography were additionally performed. The findings were normal.
The authors diagnosed the patient as spontaneous left external iliac artery dissection and decided to perform PTA (Percutaneous transluminal angioplasty). The left femoral artery was punctured and a 12 French catheter was inserted, followed by a 0.035-inch guidewire (Terum, Tokyo, Japan). With the performance of external iliac artery angiography, a graft stent (W. L GORE VIABAHN®, Flagstaff, AZ, USA) with a diameter of 11 mm and a length of 50 mm was placed on the dissected vessel site (Fig. 2A). To confirm a proper dissection sealing, imaging of the vessel using IVUS(Intravascular ultrasound) was conducted and it showed no abnormal findings (Fig. 2B). Afterwards, external iliac artery angiography was performed again to confirm that the vessel was well visualized to the distal part, with which the procedure was terminated (Fig. 3).
After the stent implantation, the patient showed an alleviation of the left lower abdomen pain and left flank pain. A week later, an abdominal CT scan revealed the disappearance of the left iliac artery dissection; however, there was no improvement in the hydronephrosis due to the hematoma around the dissected site and the ureteral compression on the left distal part. Serum creatinine level did not improve, either, so the treatment was commissioned to the urology department where a double J catheter insertion was performed; after this, the patient was discharged.
The abdominal CT scan performed a month later confirmed the disappearance of the hematoma and hydronephrosis near the left external iliac artery and a decrease in serum creatinine level (1.34 mg/dl). So the D-J catheter was removed, following which the patient has been monitored in the outpatient clinic.
DISCUSSION
Spontaneous external iliac artery dissection is a very rare disease and it is known to be caused by trauma, connective tissue diseases, fibrous dysplasia, lack of alpha 1-trypsin, vascular ulcer due to atherosclerosis, persistent and strong external force and so on. According to some reports published in the past, pain in the groin area, radicular pain in the back or thigh and lower extremity claudication are the main symptoms.234 Therefore, it can be predicted that its diagnosis will take a long time in many cases. This patient also complained of a sudden onset of left flank pain, and the examinations to detect urologic problems such as urinary stones preceded the diagnosis. Ultrasonography or contrast-enhanced CT may be performed for the diagnosis of the diseases, but vascular angiographic imaging is necessary for the identification of the degree of dissection and the location of intimal flaps.
In this case experienced by the authors, the patient was a healthy 50-year-old man who had no risk factors for atherosclerosis other than smoking and had no suspected connective tissue diseases or vascular diseases. He had engaged in extended physical exercise such as golf about a month before visiting the authors' hospital, but it was difficult to define this as a clear predisposing factor. Kevin D. et al. presumed, in their case report, that long-term smoking can cause vascular endothelial cell damage, atherosclerosis and aneurysm expansion in the blood vessels that have been relatively largely damaged by intense exercise such as running and swimming, leading to spontaneous iliac artery dissection.5 However, this case showed no evidence of atherosclerosis or aneurysm expansion as in the patient of the case reported by Kevin D. et al. in the abdominal and lower limb arterial angiography.
Percutaneous intervention, drug treatment and surgical treatment are all possible for lower extremity vascular dissection including external iliac artery dissection.4567 However, in cases where patients have severe symptoms or a high risk of rupture, there is a need for an immediate treatment. According to Whchulis A. R. et al., early surgical treatment is recommended because of a high probability of rupture within months of iliac artery dissection.8 In addition, Honjo O. et al. reported that 8 of 10 patients with iliac artery dissection underwent artificial blood vessel or autologous vein transplantation, which resulted in a successful treatment without a need for subsequent reoperation.9
Endovascular Tx. has the merit of being relatively easy and noninvasive compared to surgical Tx. but there has been no case of long-term monitoring so far. Kwak, Han et al. reported that percutaneous stenting was performed in two cases of spontaneous iliac artery dissection and there was no recurrence or stent stenosis during a 2 year and 10 month monitoring period.10
Since the first successful coronary artery intervention in 1977, percutaneous intervention for peripheral arteries as well as for coronary arteries have seen remarkable progresses. The American Heart Association presented recommendations for the treatment of leg arterial intervention in 2005,11 and the revised version was published in 2011. In Europe and North America as well, the Transatlantic Intersociety Consensus Working Group was formed in 2001, centered on the departments of interventional radiology, vascular surgery and cardiology. This group has continuously published and revised treatment guidelines until recently.12 However, these guidelines mostly include content related to the stenosis and occlusion of lower limb arteries associated with arteriosclerosis or diabetes. The authors successfully performed stent implantation using percutaneous intervention in the patient with spontaneous iliac artery dissection, and confirmed that there were no specific problems such as recurrence or restenosis, although the monitoring was only carried out for a relatively short period of seven months. Based on this, the authors believe that objective and systematic guidelines for the dissection and rupture of peripheral arteries including iliac arteries as reported in this case are necessary.


 XML Download
XML Download