

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Cases of esophageal injury, deep neck infection, and mediastinitis caused by accidental ingestion of a fish bone have frequently been reported in the previous papers. However, intestinal perforation or development of an intra-abdominal abscess caused by ingestion of fish bone is rare. Abscess formation can occur secondary to a penetrating injury to a segment of the small or large intestine due to a sharp, ingested foreign body.
Herein, we describe a case of a 78-year-old man who developed an intra-abdominal abscess caused by fish bone. An abdominal computed tomography (CT) scan demonstrated a 5 cm cystic, contrast-enhancing lesion with adjacent fatty infiltration of the periumbilical mesentery. The diagnosis of a periumbilical mesenteric abscess caused by a foreign body, ultimately identified to be a fish bone, was confirmed following colonoscopy. On further history taking, the patient did not recall swallowing a fish bone.
CASE
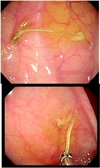
A 78-year-old man visited the emergency department with a complaint of abdominal pain of 10 days duration. His vital signs were as follows: blood pressure, 160/80 mmHg; pulse rate, 75 beats/min; and body temperature, 36.7 ℃. On physical examination, he exhibited moderate tenderness to palpation over the periumbilical area, but there was no evidence of rebound tenderness or guarding. Bowel sounds were normal and present in all 4 quadrants. There was no palpable mass. The initial laboratory findings were as follows: white blood cell count, 7,690 mm3 (neutrophils 59.7%); hemoglobin, 13.8 g/dL; platelets, 230,000/mm3; BUN, 12.7 mg/dL; creatinine, 0.71 mg/dL; and C-reactive protein, 86.1 mg/dL. Abdominal x-ray revealed no abnormal findings. The abdominal CT scan revealed a 5 cm cystic lesion with a contrast-enhancing wall associated with adjacent fatty infiltration of the periumbilical mesentery (Fig. 1). Ultrasonographyguided aspiration of the cyst demonstrated pus from which Klebsiella pneumoniae was isolated. Colonoscopic examination was performed, and it revealed that the cause of the intra-abdominal abscess was a 2 cm, sharp fish bone located in the terminal ileum. The foreign body was removed by forceps (Fig. 2, 3).
When asked about his diet, the patient had not recently experienced a foreign body sensation during meal times. After administration of ampicillin and sulbactam for 11 days, followed by oral amoxicillin and clavulanate potassium for 30 days, his symptoms improved and the abscess was not seen on the follow up CT 7 weeks after his presentation (Fig. 4).
DISCUSSION
Our case demonstrates the diagnostic and therapeutic utility of colonoscopy in the evaluation and management of an intra-abdominal abscess. Intra-abdominal abscesses can develop secondary to hollow viscus perforation and may occasionally mimic the presentation of colon cancer.12 In addition, intra-abdominal abscesses can develop secondary to localized peritonitis, which is usually due to direct microbial inoculation following trauma or recent surgery. Abscesses most commonly develop secondary to appendicitis (59%), diverticulitis (26%), surgical procedures (11%), and due to undetermined causes (4%).3 In this particular case, the cause of the intra-abdominal abscess was unveiled as a fish bone located in the terminal ileum, and ultimately, it was removed by colonoscopy.
Most ingested foreign bodies pass through the gastrointestinal tract within one week.4 Fish bone ingestion is common, but intestinal perforation due to fish bone ingestion is rare. The risk of perforation is related to the length and shape of the foreign body ingested. While intestinal perforation due to fish bone ingestion is rare, the perforation rate reaches up to 15%–35% when the ingested foreign object is sharp.56 Esophageal perforation caused by a foreign body is even rarer. High mortality associated with this condition results from the lack of clinical suspicion and late initiation of treatment. Fish bones are the most commonly ingested foreign objects that cause bowel perforation.7 Most perforations occur at areas of anatomical narrowing and angulation segments of the gastrointestinal tract, and, for these reasons, the most common sites of perforation are the ileocecal and rectosigmoid regions.8 Foreign body may cause intestinal perforation and it may lead to the development of a liver abscess, enteric fistula, intestinal obstruction, as well as peritonitis. In most cases, the ingested foreign bodies are confined to the extraluminal space, without any penetration of adjacent organs (Table 1).
Fish bone ingestion can cause pancreatitis, appendicitis, and liver abscess as well as intra-abdominal abscess.91011 The most common clinical features of intra-abdominal perforations caused by foreign body ingestion are abdominal pain, fever, and localized peritonitis.12 Plain radiography, ultrasound, CT, upper gastrointestinal series, upper endoscopy, colonoscopy, and laparotomy can be used to detect/identify foreign bodies in the gastrointestinal tract.13 Fish bones are usually invisible on a plain film. A CT scan of the abdomen is helpful to detect fish bones.14 However, fish bone in the hollow viscus is not detected by a CT scan and a definitive preoperative history of ingestion of a foreign body is usually uncertain as in our case. Therefore, accurate determination of the cause of an intra-abdominal abscess before operation can be difficult. Therefore, in patients who cannot recall swallowing a foreign body, and who are found to have an abscess of unknown origin on imaging, colonoscopy may be indicated to evaluate this possibility. If a foreign body is embedded within the abscess, an open laparotomy and removal of the foreign body is the recommended treatment of choice.15 Especialy in case of elderly people, the masticatory function may be deteriorated due to tooth problem. Hence, they are likely to be at a greater risk of ingesting a foreign body unconsciously during meal times.
In our case, conservative management was chosen, and the abscess resolved after colonoscopic retrieval followed by treatment with systemic antibiotics.
When a patient presents with an intra-abdominal abscess of unknown cause, the possibility of foreign body ingestion must be considered even though the patient denies having swallowed any foreign body.




 XML Download
XML Download