

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Giant pulmonary bulla (GPB), first described by Burke in 1937, is a rare clinical and radiological manifestation which usually occurs in the upper lobes of the lung.123 GPB commonly increases in size over time and develops into respiratory symptoms commonly caused by a pneumothorax or by the compression of the adjacent lung.24 According to these characteristics of GPB, it is clinically accepted that patients with GPB will greatly benefit from a surgical intervention: bullectomy.56 However, few case reports have been reported to show the complete resolution of GPB after the inflammatory process, such as an infected bulla or peribullous pneumonia, without any additional interventional procedure or surgery.7 Herein, we present a rare case of a complete resolution of GPB after the inflammatory process without the administration of any further interventional procedure or surgical resection.
CASE
A 51-year-old man was referred to our hospital due to pleuritic chest pain in right side of his chest. The subsequent chest X-ray identified a cystic lung lesion. Four years prior to his visit, he was treated for a lower urinary tract infection in our hospital. At that time, his chest X-ray showed a GPB measuring 10.0×9.4 cm on the right upper lobe (RUL). (Fig. 1A) Three days prior to his admission, the patient developed the following symptoms: coughing, purulent sputum, and intermittent chills with myalgia. He was a smoker with a history of 15-pack-year. However, he had quit smoking for 1 month.
During the examination, he exhibited an ill-mannered temperament, his body temperature was 37.9 ℃, blood pressure was 135/70 mmHg, pulse was 88 beats/min, respiration rate was 22/min, and his oxygen saturation was 94% to 96% while breathing ambient air. In the laboratory test, the total WBC count was normal but the C-reactive protein (CRP) was mildly elevated (82.5 mg/L).
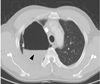
A chest radiograph showed the air-fluid level was newly developed in the GPB of RUL. (Fig. 1B) A computed tomography (CT) scan of the chest revealed that the GPB was occupying the near total space of RUL and heterogenic density of air-fluid level, suggesting an infected GPB. (Fig. 2)
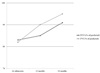
The patient was admitted and treated with a 2-week course of intravenous piperacillin/tazobactam and levofloxacin. All microbiological tests including sputum culture, blood culture, pneumococcal urinary antigen test, and atypical pneumonia antigen PCR test came back with a negative result. His pleuritic chest pain and chills with myalgia had improved within 3 days. He was discharged after 1 week of antibiotic therapy and received a 2-week prescription for oral antibiotics. After 3 weeks of antibiotic therapy, we followed up with a chest X-ray. (Fig. 1C, D) One year after the treatment of the infected GPB, a subsequent chest X-ray showed that the GPB had disappeared completely and left a small fibrotic scar on the RUL. During the 3-year follow-up study, the patient did not exhibit any respiratory discomfort or symptoms. Furthermore, his lung function has also improved with the resolution of GBP. (Fig. 3)
DISCUSSION
A pulmonary bulla is defined as the well-demarcated air-space in the lung parenchyme, and measures over 1 cm in diameter in the distended state with less than 1 mm of wall thickness.8 The term of GPB is used when the bulla occupies at least 30 percent of one hemithorax.4
Although some factors of the progressive air-trapping based on a check-valve mechanism have been proposed in congenital pulmonary and vascular malformations, GPB is known as a long-term side effect of cigarette smoking in the majority of cases.45 The natural clinical course of GPB is not predictable, although spontaneous regression of GPB can occur on rare occasions. It is usually marked by a gradual increase in size and the development of respiratory symptoms resulting from pulmonary impairment or compression of the adjacent lung.24910 Moreover, it can also be complicated by pneumonia or pneumothorax. For these reasons, a surgical resection or bullectomy is traditionally recommended when possible.511 In our case, the patient refused to undergo a surgical procedure because of the rapid improvement of his pleuritic pain after receiving medical therapy. This was also in consideration to the gradual enlargement and infected condition of his GPB, which may have suggested a need for surgical resection.
However, there is no current definitive guideline for the treatment of GPB, despite the widely accepted use of surgical resection. Percutaneous intra-cavitary drainage is also administered as an alternative therapeutic method on patients with severely impaired lung function or other comorbidities.1112 Remarkably, the GPB of RUL was completely resolved in the absence of any surgical intervention in this patient. He was only treated with medical therapy for the infected GPB. Surgical resection was considered once the patient became more stabilized. However, the proposal was dismissed as the patient's clinical symptoms showed rapid improvement.
Although the actual mechanism of this natural GPB resolution is still not clear, two hypotheses can be postulated.713 First, cases associated with infection may result from the obliteration of the bronchus supplying the GPB by mucus formation and/or airway edema, and, as a result of this airway obstruction due to the inflammation, it accelerates reabsorption of trapped air resulting in the shrinkage of GPB. The second explanation is that the retraction of GPB can compress the adjacent bronchus supplying the GPB itself. It also can result in reducing air-flow to the GPB with comparable recoil pressure over a long period. In our case, it can be explained by the first hypothesis as the patient had infected bullae and his GPB gradually regressed.
This spontaneous regression of the volume of GPB without lung volume reduction surgery is also called “inflammatory autobullectomy.”1415 Several previously reported cases, including a case that was reported in South Korea, showed that this mechanism of inflammatory autobullectomy was based on the association of lower respiratory tract infection.71416 Furthermore, rapid improvement of lung function after inflammatory autobullectomy is also observed to be as good as surgical bullectomy.17 Similar observations were also made in our case study as the patient showed improvement in lung function in subsequent pulmonary function tests. (Fig. 3)
In conclusion, this rare case of the inflammatory autobullectomy should be observed as a remarkable yet exciting medical phenomenon as the patient was fully recovered without additional lung volume reduction surgery. However, a cautious clinician must also always be aware that surgical intervention is the primary therapy method with the patients with GPB because this phenomenon is not common.

 XML Download
XML Download