

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Checking axillary lymph node metastasis in breast cancer patients is critically in order to assess the patient's prognosis and come up with a treatment plan.1234 Recently, axillary lymph node metastasis is determined by sentinel lymph node biopsy.567 However, sentinel lymph node biopsy is accompanied by long-term and short-term complications like lymphedema, which occurs in 7% of all patients who undergo surgery for breast cancer.8 Therefore, to reduce the frequency of complications, many studies have sought to determine axillary lymph node metastasis through non-invasive methods using various kinds of diagnostic imaging.91011
Magnetic resonance imaging (MRI) is a non-ionizing imaging technique, and is a type of diagnostic imaging using hydrogen nuclear fusion reaction in the body within the magnetic field.12 This imaging is very useful for checking malignant lesions, and can be used to obtain additional information.12 Recently, some studies are examining diagnostic methods using nanoparticles.131415161718 Superparamagnetic iron oxide is an inorganic nanoparticle with the central part consisting of iron oxide, which is a metal molecule.19 This particle shows a dark signal on T2 MRI of normal lymph nodes, but a white signal in metastatic lymph nodes.2021 Therefore, superparamagnetic iron oxide MRI can be used to distinguish normal lymph nodes and metastatic lymph nodes.
Accordingly, the researchers in this paper conducted a meta-analysis to determine the diagnostic value of superparamagnetic iron oxide MRI in determining axillary lymph node metastasis in breast cancer patients.
MATERIALS AND METHODS
Article search method
To evaluate the diagnostic value of superparamagnetic iron oxide MRI in determining axillary lymph node metastasis in breast cancer patients, the researchers searched studies that had been registered on PubMed, Cochrane Library, ScienceDirect, SpringerLink, and Ovid databases up until December 2013, and searched for articles including the keywords and titles “magnetic resonance imaging AND axilla” and “superparamagnetic iron oxide AND axilla.”
Standard for article selection
Three researchers (J.G.P., D.W.R. and Y.S.K) reviewed all searched articles and decided whether they were suitable for analysis. The articles included in this study must be 1) original articles, 2) articles that determined metastasis based on biopsy, 3) articles published in English, or 4) articles that report or can calculate true positive, false positive, false negative and true negative values. Among the searched articles, ones that are not original articles (reviews, poster presentations, case reports, etc.) and ones published in languages other than English were excluded.
Qualitative evaluation of articles
All researchers planned and reviewed this study together. In the case where there were different opinions over the selection of articles, discussions were held until agreement was reached. For qualitative evaluation of the analyzed articles, the “QUADAS tool (quality assessment of diagnostic accuracy studies tool)” was used.
Analysis goal
The goal of this study is to evaluate the diagnostic value of superparamagnetic iron oxide MRI. To this end, true positive, false positive, false negative and true negative values included in the selected articles were used to analyze the sensitivity and specificity of superparamagnetic iron oxide MRI.
Statistical analysis
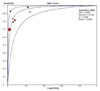
The heterogeneity of articles included in the study was evaluated through Cochran's Q test and I2-statistics. It was considered that there was heterogeneity if P-value is lower than 0.1 in Cochran's Q test.22 Moreover, the level of heterogeneity was determined by dividing the range of I2-statistics into three ranges (< 25%: low, 25–75%: moderate, > 75%: high) of heterogeneity.23 A random model effect was used when heterogeneity was confirmed. The results of analysis were quantified using the SROC (summary receiver operating characteristics) curve, and AUC (area under curve) was identified to evaluate the diagnostic value of superparamagnetic iron oxide MRI. Furthermore, a subgroup analysis was conducted to verify the cause of heterogeneity among studies.
All studies were statistically analyzed using Meta-Disc 1.4 (Clinical BioStatistics Unit, Hospital Universitario Ramón y Cajal, Madrid, Spain) and STATA 12.0 (STATA Co., College Station, Texas, United States), and it was considered statistically significant when the P-value was lower than 0.05.
RESULTS
Article search results
Figure 1 shows the flow chart for the article selection in this meta-analysis. A total of 346 articles were searched, 7 of which were ultimately selected and analyzed in this study. Redundant articles were determined by checking the author names, titles and contents.
Characteristics of analyzed articles and qualitative evaluation
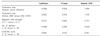
Table 1 shows the quality and characteristics of articles included in this study. All included articles were published between 2002 and 2011. Moreover, all articles had a QUADAS score of 8 or higher, indicating that they were generally acceptable studies.
Diagnostic accuracy and SROC curve
In this meta-analysis, superparamagnetic iron oxide MRI had a sensitivity of 0.83 (95% confidence interval: 0.75 – 0.89) and specificity of 0.97 (95% confidence interval: 0.94–0.98) (Fig. 2).
Figure 3 shows the SROC curve of superparamagnetic iron oxide MRI, and AUC turned out to be 0.9563.
Heterogeneity of articles and subgroup analysis
Table 2 presents the heterogeneity of studies on superparamagnetic iron oxide MRI. Both sensitivity (P = 0.0062, I2 index = 66.7%) and specificity (P = 0.0987, I2 index = 43.8%) showed moderate heterogeneity.
Furthermore, Table 3 shows the results of subgroup analysis. This study proved that the surgical method (sentinel lymphadenectomy) had the highest diagnostic accuracy for axillary lymphnode metastasis (sensitivity = 1.00 (95% confidence interval: 0.16–1.00), specificity = 1.00 (95% confidence interval: 0.63–1.00). The authors attempted to conduct a subgroup analysis according to stage and patient age as well, but failed due to the lack of data.
Meta-regression analysis
To determine the cause of heterogeneity, the authors conducted a meta-regression analysis on the year of publication (before 2009 vs. after 2010), area of publication (East vs. West), magnetic field strength (1.5 tesla vs. 1.0 tesla), number of research subjects (less than 10 persons vs. 10 persons or more), and QUADAS score (lower than 10 points vs. 10 points or higher) (Table 4). In this meta-analysis, QUADAS score (P = 0.010, relative diagnostic odds ratio (DOR) = 0.351) turned out to be the factor related to heterogeneity.
DISCUSSION
This study analyzed the diagnostic value of superparamagnetic iron oxide MRI in determining axillary lymph node metastasis of breast cancer patients by analyzing sensitivity and specificity. The authors searched previous studies that conducted a histological diagnosis after superparamagnetic iron oxide MRI and analyzed the accuracy of the aforementioned diagnostic imaging, and ultimately analyzed 7 articles conducted on a total of 118 patients.
This meta-analysis searched and analyzed clinical studies published up until December 2013 and thus it does not include data published after that. The QUADAS tool was used for qualitative evaluation of the articles included in this meta-analysis.
Studies included in this meta-analysis had heterogeneity in both sensitivity and specificity. Thus, a meta-regression analysis was conducted to analyze the cause of such heterogeneity, and it was discovered that the QUADAS was the biggest cause of heterogeneity.
Moreover, a subgroup analysis was conducted on studies included in this meta-analysis to analyze the factors related to the accuracy of diagnosing axillary lymph node metastasis, and it was found that sentinel lymph node biopsy was the factor that had the highest accuracy in diagnosing axillary lymph node metastasis. However, only in 1 of the 7 articles was sentinel lymph node biopsy performed, which indicates that more research is needed.
In this study, sensitivity and specificity of superparamagnetic iron oxide MRI in determining axillary lymph node metastasis were 0.83 (95% confidence interval: 0.75 – 0.89) and 0.97 (95% confidence interval: 0.94 – 0.98) respectively, revealing a high diagnostic value, which can be identified through the AUC value using the SROC curve (AUC = 0.9563).
This study has a few limitations. First, even though the database was generally used in meta-analysis such as EMBASE, this study failed to check the database for which the organization has no search rights. However, the authors made the most of the database for which the organization has search rights, such as PubMed, Cochrane Library, ScienceDirect, SpringerLink, and Ovid databases. Moreover, they checked each of the references for the articles included in this meta-analysis to minimize loss of data. Second, most studies included in this meta-analysis included both “patient to patient” data and “lesion to lesion” data, but some studies only presented either “patient to patient” or “lesion to lesion” data. This study gave priority to “patient to patient” data in analysis. Therefore, studies with no “patient to patient” data were analyzed by applying “lesion to lesion” data, which may have affected the study results. However, in studies that presented both “patient to patient” data and “lesion to lesion” data, each of the data sets did not show much a numerical gap in sensitivity and specificity, and thus may not have had a crucial effect on the study results. However, more research is needed for more accurate analysis.
In conclusion, superparamagnetic iron oxide MRI may be an effective diagnostic imaging technique for stage setting and prognostic prediction by determining axillary lymph node metastasis before surgery in breast cancer patients. Furthermore, it will help determine whether to perform invasive diagnosis such as sentinel lymphadenectomy or axillary lymph node dissection, which will be useful in preventing complications.





 XML Download
XML Download