

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although the cancer-related death rate has significantly dropped since 1991, and led to more than 1.7 million deaths by the year 2012, it is still the leading cause of death [1]. Gastric cancer (GC) represents the men's third and the women's forth leading cancer diagnosed and the third leading cause of death among both men and women in China [2]. With great progress in the diagnoses and treatments, the prognosis of GC has greatly improved, while the 5-year survival rate is still very poor in individuals with advanced GC [3]. Conventional biomarkers, such as carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9, have been inefficient because of their low sensitivity and specificity that can hardly predict overall survival accurately [4]. Therefore, novel biomarkers are needed for early diagnoses and determining accurate prognoses.
Fibrinogen and platelets play complex and varied roles in tumor formation and progression. Previous studies have reported that platelets and fibrinogen facilitate each other in protecting tumor cells from natural killer cells [5]. Satoshi Takagi reported that platelets can promote tumor growth and metastasis via direct interaction between aggrus/podoplanin and clec-2 [6]. Moreover, in our previous study, we found that serum fibrinogen levels were positively correlated with advanced tumor stage and poor survival in patients with gastric cancer undergoing gastrectomy [7]. Lian et al. [8] reported that mean platelet volume (MPV) predicted chemotherapy responses and prognoses in patients with unresectable gastric cancer. For these reasons, we conducted this study to investigate the combination of functions of fibrinogen, platelets, and MPV for predicting survival of patients with GC.
MATERIALS AND METHODS
Patient selection
For the study, 1,946 consecutive histologically proven GC patients, aged from 19 to 88 (mean age: 62 years), that underwent gastrectomy between January 2007 and December 2011, and 299 patients with benign gastric tumor (BGT) between January 2000 and June 2018 at the Harbin Medical University Cancer Hospital (Heilongjiang, China) were recruited. All of these patients signed the informed consents for the use of their data for future study when admitted to our hospital and this research obtained the approval and support of the Medical Ethics Committee(approval number SHGC-1029) of Harbin Medical University Cancer Hospital.
The inclusion criteria of GC patients were as follows: all of these patients 1) underwent total or subtotal gastrectomy; 2) never received chemotherapy, radiotherapy, or other anticancer treatments; 3) survived for more than two months and none died in perioperative period; 4) never received transfusions or other blood products before blood examination; 5) died from GC or related diseases. BGT included gastric polyps, gastric leiomyoma, gastric neurofibroma, and others. Blood examinations were conducted immediately or the second day after being admitted to our hospital to assess platelet count (109/L), fibrinogen (g/L), MPV (fL), CEA (ng/mL), and CA 19-9 (U/mL). The pathological staging was based on the 7th edition of the TNM-classification (for the “Tumor-Nodes-Metastases” system) by the Union for International Cancer Control/American Joint Committee on Cancer (UICC/AJCC).
For our convenience, we used the following terms: fibrinogen*MPV (FM), platelet count*fibrinogen*MPV (PFM), fibrinogen count/MPV ratio (FMR), platelet count*fibrinogen (PF), (platelet count*fibrinogen)/MPV ratio (PFMR), platelet count*MPV (PM), platelet count/MPV ratio (PMR).
Patient follow-up
These GC patients were followed-up every 3 months for the first 2 years and every 6 months in the following several years until death or June 2016. The follow-up time varied from 3 months to 9 years with an average duration of 37 months, and the overall survival time was evaluated from surgery to death.
Statistical analysis
The Student's t-test was used to compare the levels of fibrinogen, platelets, MPV, and FMR among different stages. The optimal cut-off levels for fibrinogen, platelet, MPV, FMR, and PMR were determined by receiver operating curve (ROC) analysis [9]. Chi-square test was used to compare and assess the association of platelets with fibrinogen and clinicopathological characteristics. Survival curves were calculated by Kaplan-Meier survival analysis along with log-rank test. Multivariate analysis was evaluated by Cox proportional hazardous model, and all of the significant factors in the univariate analysis were used in multivariate analysis. P<0.05 was considered statistically significant. All of the statistical analyses were performed using SPSS version 17.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
The relationship between clinicopathological characteristics, prognosis, and biomarkers
After comparison of fibrinogen, platelet, and MPV levels at different stages, we found that the differences were significant for fibrinogen in BGT vs. GC, I vs. II, I vs. III, I vs. IV, II vs. III, and II vs. IV; platelet in BGT vs. GC, I vs. II, I vs. III, I vs. IV, and II vs. III; and MPV in BGT vs. GC, I vs. II, and I vs. IV (Fig. 1). No other significant differences were observed between any other stages. In general, the levels of fibrinogen, platelets, and MPV were increased along with stages developed.
Fig. 1
Comparison of fibrinogen, platelet, MPV, and FMR between different stages. Data represents averages and standard deviation of plasma fibrinogen, platelet, MPV, and FMR levels in peripheral blood.
MPV = mean platelet volume; FMR = fibrinogen to mean platelet volume ratio.
*P<0.001; †P<0.05.

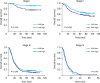
The ROC curves and cut-off points for fibrinogen, platelet, MPV, FM, PFM, FMR, PF, PFMR, PM, and PMR of GC patients are shown in Fig. 2 and Table 1. As the cut-off point for MPV was not significant, we took the upper limit of normal level 11.0 to divide MPV. Next, in univariate survival analyses, patients with low fibrinogen and platelet levels had better prognoses, but no significant differences in MPV levels were observed (Fig. 3). So, we investigated the relationships between fibrinogen and platelets and clinicopathological features (Table 2). The patients were divided into 2 groups based on the mean age (62 years), the mean value of maximum diameter of the tumor (6.16 cm), and the mean value of MLNR (31.5%). Fibrinogen level was significantly associated with age, tumor depth (T), lymph node metastasis (N), distant metastasis (M), AJCC stage (TNM), radicality, tumor size, metastasis lymph node rate (MLNR), CA19-9, and CEA (Pall<0.05). Platelet level was significantly associated with sex, age, T, N, TNM, radicality, tumor size, MLNR, CA 19-9, and CEA (Pall<0.05), and was not significant for distant metastasis (P=0.715).
Fig. 2
Optimal cut-off points for these indexes were on with ROC curves.
ROC = receiver operating curve; PFM = platelet*fibrinogen*mean platelet volume; PF = platelet*fibrinogen; PM = platelet*mean platelet volume; PMR = platelet to mean platelet volume ratio; FM = fibrinogen*mean platelet volume; FMR = fibrinogen to mean platelet volume ratio; PFMR = (platelet*fibrinogen) to mean platelet volume ratio; MPV = mean platelet volume.

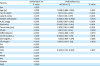
Table 1
The optimal cut-off point for overall survival
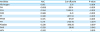
FM = fibrinogen*mean platelet volume; PFM = platelet*fibrinogen*mean platelet volume; FMR = fibrinogen to mean platelet volume ratio; PF = platelet*fibrinogen; PFMR = (platelet*fibrinogen) to mean platelet volume ratio; PM = platelet*mean platelet volume; PMR = platelet to mean platelet volume ratio; MPV = mean platelet volume; AUC = area under curve.
Fig. 3
Kaplan-Meier curves for overall survival based on levels of fibrinogen, platelet, and MPV.
MPV = mean platelet volume.
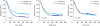
Table 2
Relationship between clinicopathological features and fibrinogen and platelets
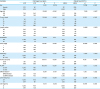
The relationship between indexes, clinicopathological characteristics, and clinical prognosis
In the univariate survival analyses, we found that patients with low FM, PFM, FMR, PF, PFMR, PM, and PMR exhibited better prognoses and longer overall survival times (Pall<0.05) (Fig. 4, Table 3). Additionally, age, T, N, M, TNM stage, radicality, tumor size, MLNR differentiation, CA 19-9, and CEA were all associated with overall survival times. When we included age, T, N, M, TNM stage, radicality, tumor size, MLNR, differentiation, CA19-9, CEA, fibrinogen and FMR into multivariate analysis, the results showed that T, N, M, TNM stage, radicality, tumor size, MLNR, fibrinogen, and FMR were all independent risk factors affecting patient survival (Pall<0.05).
Fig. 4
Kaplan-Meier curves for overall survival based on FM, PFM, FMR, PF, PFMR, PM, and PMR.
FM = fibrinogen*mean platelet volume; PFM = platelet*fibrinogen*mean platelet volume; FMR = fibrinogen to mean platelet volume ratio; PF = platelet*fibrinogen; PFMR = (platelet*fibrinogen) to mean platelet volume ratio; PM = platelet*mean platelet volume; PMR = platelet to mean platelet volume ratio.
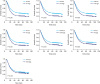
Table 3
Univariate and multivariate analysis of factors for overall survival
HR = hazard ratio; CI = confidence interval; AJCC = The American Joint Committee on Cancer; MLNR = metastasis lymph node rate; CA = carbohydrate antigen; CEA = carcinoembryonic antigen; FM = fibrinogen*mean platelet volume; PFM = platelet*fibrinogen*mean platelet volume, FMR = fibrinogen to mean platelet volume ratio; PF = platelet*fibrinogen; PFMR = (platelet*fibrinogen) to mean platelet volume ratio; PM = platelet*mean platelet volume; PMR = platelet to mean platelet volume ratio.
Finally, we examined the value of these indicators for different stages (Table 4). Fibrinogen, FM, PFM, and PF were all significant at stage III and PMR was significant at stage IV. Only FMR was significant at stages I, II, and III. Kaplan-Meier survival curves are shown in Fig. 5. The comparisons between BGT and GC and their stages were shown in Fig. 1 and the comparisons were significant in BGT vs. GC, I vs. II, I vs. III, I vs. IV, II vs. III, and II vs. IV.
Table 4
Univariate analysis of factors for overall survival at different stages

FM = fibrinogen*mean platelet volume; PFM = platelet*fibrinogen*mean platelet volume; PF = platelet*fibrinogen; PFMR = (platelet*fibrinogen) to mean platelet volume ratio; PM = platelet*mean platelet volume; PMR = platelet to mean platelet volume ratio; FMR = fibrinogen to mean platelet volume ratio.
DISCUSSION
In this study, we found that plasma levels of fibrinogen and platelets were significantly different at various stages and played important influence on prognosis, and this corroborated with previous reports [610]. Fibrinogen and platelets had crucial effect on the tumorigenesis, tumor progression, and prognosis. In our previous study, we had found that platelet level was closely associated with tumor-induced systemic inflammatory response (SIR) and prognosis of patients with advanced GC [11]. As a main indicator of platelet activation status, MPV has also been reported to be associated with prognosis of malignant diseases [1213]. Therefore, it is essential to combine fibrinogen, platelet, and MPV together to reveal their combined prognostic significance. This investigation was the first successful attempt to appraise the prognosis of patients with GC based on so many indicators obtained by evaluation of fibrinogen, platelet, and MPV levels.
As a major acute reactive phase protein produced by liver, fibrinogen levels increase in the event of malignances or SIR [14], and its level would decrease after surgery and increase again at the time of recurrence [10]. The hyperfibrinogenemia was also reported to affect prognosis in many other malignancies, such as non-small-cell lung cancer [15], esophageal cancer [16], and breast cancer [17]. Fibrinogen promoted lymph node metastasis by interacting with IL-6 and platelets [18]. Mikami et al. [19] reported that platelets can promote the proliferation of gastric cancer cells, which, in turn, can be inhibited by antiplatelet antibodies, meanwhile mir-4670-5p might be involved in this process. Goel et al.'s [20] experiments also showed that the degree of aspirin-inhibited colon cancer cells was dependent on the mismatch repair (MMR) status. Tumor cells could release high-mobility group box1 protein, and when they escape from the primary tumor, could hang together with fibrinogen and platelets and cluster around to dodge the innate immune systems, especially NK cells, and then, the tumor cells could reside in the vasculature of distant organ [212223]. The level of MPV, an intimation of platelet size, reflected the activity of the platelets, and the increase in MPV was reported in myocardial infarction and cancers [2425]. But in our study, we found that the MPV was significantly higher in BGT than that in GC and it increased further along with cancer progression. The exact mechanisms of how fibrinogen and platelets promote tumor progression were still controversial.
In the univariate analysis, fibrinogen, platelet, FM, PFM, FMR, PF, PFMR, PM, and PMR were all significant prognostic factors. When incorporated into Cox multivariate analysis, fibrinogen, PFMR, FM, PMR, and FMR all showed prognostic abilities. This may indicate that fibrinogen, platelet, and MPV can be used in combination as indicators of prognosis. But when we divided these patients according to the AJCC TNM stage, FMR showed prognostic ability only in stages I, II, and III; PMR showed prognostic ability only in stage IV; and fibrinogen, FM, PFM, and PF showed prognostic ability only in stage III. This indicated that FMR may be a superior biomarker for predicting survival of patients with GC. In addition, although fibrinogen and platelet facilitated infiltration and migration of tumor cells, we speculated that whether distant metastasis would develop didn't depend on the level of fibrinogen and platelet. These indicators may be more suitable to predict survival in non-metastasis GC patients.
The current study has some unavoidable constraints. First, it is a single-center and retrospective research with some uncertain bias. Secondly, the effect of chemotherapy on survival and the relationships between chemotherapy and these biomarkers were not evaluated in this research. However, within these limitations, our findings still showed the prognostic significance of these biomarkers. Although the principle may still be controversial, with their merits of convenience and attractive price without any additional injuries, these biomarkers should be included in prognostic risk stratification models and clinical applications.
In conclusion, elevated levels of fibrinogen and platelets are associated with advanced stages and poor prognosis, and fibrinogen, platelet, and MPV can be combined together for predicting survival of patients with GC. Meanwhile, fibrinogen and FMR can be considered as independent risk factors for overall survival in non-metastatic GC. This will help clinicians to formulate therapeutic strategies and provide better cure to the patients.
 XML Download
XML Download