

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chordomas are rare, aggressive bone tumors that occur in the axial skeleton. The sacrococcygeal region is the most common site, accounting for 65% of all cases of chordomas, followed by the spheno-occipital/nasal (25%), cervical (10%), and thoracolumbar (5%) spines.1 This tumor is thought to originate from notochordal remnants.2 Histologically, chordomas are characterized by lobulated masses that are separated by thick fibrous septa. Tumors typically consist of physaliphorous cells that are arranged in cords or sheets within the abundant myxoid stroma. Histologically, there are three different subtypes of chordoma, namely, chondroid, dedifferentiated, and classical, with the chondroid type having better prognosis than the classical type.3
Because surgery of the skull base or sacral area is difficult due to the complex anatomy and adjacent critical structures, complete tumor resection is often impossible, and patients usually receive adjuvant therapy or radiotherapy like proton therapy.4 Thus, the benefit of adjuvant treatment according to the tumor location has been investigated.567 Meanwhile, few studies have conducted a detailed comparison of the histologic features of skull base and spinal/sacral chordomas. A previous study demonstrated that skull base chordoma (SBC) patients are significantly younger than non-SBC (NSBC) patients.8 Histologically, spinal chordoma shows increased proliferative capability,9 abundant intralesional fibrous septum and extracellular mucoid matrices, and a less frequent chondroid appearance.10 SBCs present with phagocytosis (hemosiderin deposits) more frequently than NSBCs.10
Yamaguchi et al.11 suggested a benign notochordal cell tumor (BNCT) as a precursor lesion of chordoma. BNCT is characterized by sheets of benign-looking, adipocyte-like large cells without intervening stroma. However, whether BNCT is a precursor or tumor component itself remains controversial,1213 and the histologic evaluation and clinical implication of these components in chordomas are yet to be clarified.
This study aimed to evaluate the clinicopathological features and prognosis of chordomas according to its location. The patients were divided into two groups according to the location of the chordoma, and the clinicopathological variables were compared between the two groups. The prevalence of BNCT-like component in each location was also analyzed.
METHODS
Patients and ethical concerns
Patients with chordomas admitted to Samsung Medical Center between March 1996 and February 2015 were retrospectively enrolled. Data on the patients' age at initial diagnosis, gender, tumor size, type of tumor resection (complete or incomplete), and postoperative adjuvant treatment were obtained from medical records. Magnetic resonance images of all the patients were reviewed to identify the tumor location. Chordomas were divided into two groups: SBCs and sacral/spinal chordomas (SCs). The SBCs included tumors of the clivus, sphenoid, spheno-occipital, sella/parasellar regions, petrosal part of the temporal bone, and intradural chordomas. Meanwhile, SCs included tumors of the spine and sacrococcygeal regions. For SBCs, tumor extension beyond the clivus or skull base was defined as an extracranial extension.
Histopathologic analysis
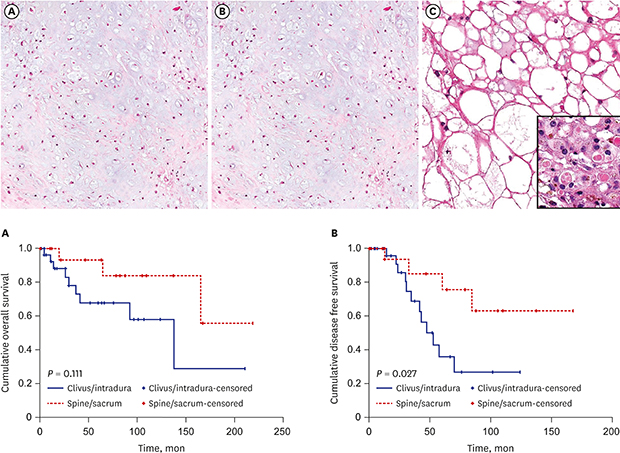
Histologic examination was performed using hematoxylin and eosin (H&E)-stained slides. All slides were retrospectively reviewed by two pathologists. The following histologic parameters were evaluated: tumor matrix (chondroid or myxoid [non-chondroid]), growth pattern (lobulating or diffuse), necrosis, presence and proportion of BNCT-like component, nuclear pleomorphism, and intracytoplasmic hyaline globules. Chondroid matrix was defined as bluish homogeneous matrix reminiscent of hyaline cartilaginous matrix, which was distinguished from eosinophilic, pinkish secretory materials or myxoid matrix (Fig. 1A). Lobulating growth pattern was assessed when obvious intralesional fibrous septa were identified under a low-power magnification (Fig. 1B). BNCT-like component was defined as sheets of large uni- or multivacuolated adipocyte-like cells with eccentrically located small nuclei and lacked the intervening tumor matrix (Fig. 1C). Nuclear pleomorphism was evaluated according to the following criteria: absent, small bland looking nuclei with inconspicuous nucleoli; present, enlarged nuclei having prominent nucleoli and membrane irregularity.
Fig. 1
Characteristic histologic features of chordomas. (A) Chondroid matrix is frequently found in clival/intradural chordomas. (B) Fibrous septae with lobulating pattern is often observed in spinal/sacral chordomas. (C) BNCT-like area in clival chordoma. The cells resemble mature adipocytes and have eccentrically located small nuclei. Hyaline globules, one of the features of BNCT, are occasionally observed in BNCT-like areas of chordomas (inlet).
BNCT = benign notochordal cell tumor.

Immunohistochemical staining for Ki-67
To evaluate the proliferative activity of tumors, Ki-67 immunohistochemistry was performed for each tumor. Sections from formalin-fixed paraffin-embedded tissue were used for immunohistochemistry with antibodies against Ki-67 (clone MIB-1; 1:1,000; Abcam, Cambridge, UK). Briefly, 4-µm-thick paraffin sections were deparaffinized and rehydrated using xylene and alcohol solution. Immunohistochemistry was performed using the Ventana Discovery XT automated stainer (Ventana Medical System, Tucson, AZ, USA). Antigen retrieval was performed using cell conditioning 1 buffer (citrate buffer Ph 6.0, Ventana Medical System). Appropriate positive and negative controls for immunohistochemistry were included. The findings of immunohistochemical staining of all cases were assessed with eyeball interpretation method by two pathologists using light microscopes.
Statistical analysis
Results were expressed as mean ± standard deviation. Data were analyzed using SPSS for Windows (version 18.0; SPSS Inc., Chicago, IL, USA). Mann-Whitney U test and Kruskal-Wallis test were used to compare continuous variables, and Pearson's χ2 tests and Fisher's exact tests were used to compare categorical variables. Wilcoxon signed-rank tests were used to compare matched variables. Logistic regression analysis was used to assess the risk factors for death and recurrence. Disease-free survival (DFS) was calculated from the date of the first surgery to the date of the first regional or systemic relapse. Overall survival (OS) was estimated from the date of the first surgery to the date of the last follow-up or death from any cause. Cox proportional hazard model was used to assess the risk factors for overall survival and disease-free survival, and patients who were followed-up over 6 months were included for analysis. Kaplan-Meier survival curves and log-rank statistics were employed to evaluate time to survival. P < 0.05 was considered significant.
RESULTS
Comparison of clinicopathologic profile of patients between SBCs and SCs
In total, 52 patients were included in the analysis. Of them, 32 (61.5%) were men, and 20 (38.5%) were women. The mean age was 54.4 years (range, 18–82 years). The course of disease duration ranged from 1 to 276 months (average, 57.4 months). Regarding tumor location, 32 patients (61.5%) and 20 patients, (38.5%) had SBCs and SCs, respectively. The clinicopathologic features of the patients with SBCs and SCs are shown in Table 1. There was no dedifferentiated chordoma in the present cohort. Most of the SBCs affected the clivus (27 cases, 84.4%), from which extracranial extension was found in 17 patients. There were 3 cases of intradural chordoma. Extracranial extension of the tumor affected the sphenoid bone, pterygoid bone, and nasopharynx. Meanwhile, the most frequently affected region in SCs was the sacrococcygeal region (16 cases), followed by the cervical (3 cases) and thoracic spines (1 case). The mean age at diagnosis of the patients with SBCs was younger (53.5 years) than those with SCs (57.7 years). Meanwhile, the mean size of the tumors was significantly larger in SCs (65.4 mm) than that in SBCs (40.5 mm). Death and tumor recurrence were more common in SBCs than those in SCs (28.1% and 37.5% vs. 15% and 25%). Forty-four patients (84.6%) underwent surgical resection. The total resection rate was lower in SBCs (46.4%) than that in SCs (68.8%). Among patients who underwent surgical resection, complete resection without residual tumor was achieved in only approximately 50%. Adjuvant therapy including radiotherapy and proton therapy after biopsy or surgical resection was given in approximately 50% and 65% of patients with SBC and SC, respectively. The 5-year survival rate was lower for patients with SBCs than that for patients with SCs (78.1% vs. 95.0%), but not statistically significant. Other parameters including age, gender, patient death, and tumor recurrence were not significantly different between the two groups.
Table 1
Clinicopathologic characteristics based on anatomical location and tumor extent

Regarding histopathological features, the lobulating pattern was more significantly common in SCs (85.7%) than that in SBCs (34.4%). Chondroid matrix was observed more frequently in SBCs (75%) than in SCs (43.8%). Meanwhile, nuclear atypia and necrosis tended to be more frequently found in SCs, but the frequency is not significantly different. BNCT-like features were observed in 37.5% (12/32) of SBCs and 25.0% (5/20) of SCs. Hyaline globules were found in 18.8% (6/32) of SBCs and 25.0% (5/20) of SCs. For the mean Ki-67 labeling index (LI), no significant difference was found between SBCs (mean, 2.6%) and SCs (mean, 3.2%). The Ki-67 LI of tumors and BNCT-like areas showed no significant difference according to the tumor location. However, a comparison of the Ki-67 LI of tumors and BNCT-like areas in each patient showed that large cells of BNCT-like areas tended to show a lower Ki-67 LI than those of typical chordoma areas (0.83% ± 1.82% vs. 2.28% ± 3.70%; P = 0.063).
Risk factors for mortality and recurrence in SBCs and SCs
In univariate logistic analysis, residual tumor was the only risk factor for patients' death in SBCs (Table 2). History of adjuvant treatment and presence of BNCT-like component were independent negative risk factors for recurrence in SBCs (Table 3). No significant variables associated with death or recurrence was observed in SCs.
Table 2
Risk factors for patients' death on univariate analysis
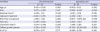
Table 3
Risk factors for recurrence based on location

In SBCs, older age and residual tumors were risk factors for shorter OS, and older age was the only independent risk factor for shorter OS (Table 4). No significant risk factor was found in SCs. There was no significant risk factor for shorter DFS in both SBCs and SCs. Only chondroid matrix seemed to be the risk factor for shorter DFS in SCs, but it was not significant (Table 5).
Table 4
Risk factors for shorter overall survival as assessed on Cox proportional hazard analysis
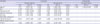
Table 5
Risk factors for shorter disease-free survival on Cox proportional hazard analysis
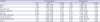
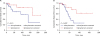
In the overall analysis regardless of tumor location, older age was the only independent risk factor for shorter OS, and chondroid matrix was the only independent risk factor for shorter DFS. The OS was not significantly different between patients with SBCs and SCs. However, the patients with SBCs showed significantly shorter DFS than those with SCs (Fig. 2).
Fig. 2
Overall survival and disease-free survival based on tumor location. Overall survival (A) tends to be lower in patients with clival/intradural chordomas than in those with spinal/sacral chordomas, although the difference is not statistically significant. However, disease-free survival (B) of patients with clival/intradural chordomas is significantly lower than that of those with spinal/sacral chordomas.
When all patients were analyzed together, risk factors for short OS was age, which was significant in univariate and multivariate analysis (Table 6). For risk factors of short DFS, chondroid matrix was an only significant factor by univariate and multivariate analysis in all patients (Table 7). Clinvus/intradural location of tumor was a significant risk factor of short DFS by univariate analysis but not significant by multivariate analysis (Table 7).
Table 6
Risk factors for shorter overall survival for all patients on Cox proportional hazard analysis
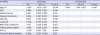
Table 7
Risk factors for shorter disease-free survival for all patients on Cox proportional hazard analysis

DISCUSSION
The present study investigated the clinicopathological features between SBCs and SCs and found that extracranial extension is frequent in SBCs affecting the clivus. SBCs were significantly smaller in size than SCs. Because the skull base is narrower than the sacrum and surrounded by cranial nerves, blood vessels, and bones, the clinical manifestations may develop earlier in patients with SBCs than in those with SCs, even in patients with smaller SBC lesions. Regarding histopathological parameters, the lobulating growth pattern typical of classical chordoma was less frequent in SBCs, while the diffuse growth pattern and chondroid matrix were more common in SBCs than in SCs. These different histopathological findings of SBCs were also observed in a previous study by Naka et al.14 In another study by Naka et al.,9 they demonstrated that the lobulation of chordoma is associated with nuclear pleomorphism and higher proliferative index, but also more favorable prognosis. The authors hypothesized that as the tumor progressed, the lobulation pattern would be replaced by diffuse growth pattern that would be related with poorer prognosis.9 In the present study, diffuse growth pattern was correlated with higher Ki-67 LI in clival/intradural chordomas, which also might reflect the tumor aggressiveness. Although no direct correlation was found between growth patterns itself and death or recurrence, it could partly be the cause of shorter DFS in SBCs.
As chondroid matrix was an independent risk factor for shorter DFS, it seems to be related with shorter DFS of SBCs. Although the surgical approach and total tumor resection are difficult in SBCs, residual tumors were not an independent risk factor of recurrence in multivariate analysis. Furthermore, in case of small biopsy specimen, chondrosarcoma would be the important differential diagnosis of SBC as chondroid matrix is frequently found in both tumors. Positive for cytokeratin immunohistochemical staining and the midline location favor the diagnosis of chordoma over chondrosarcoma in those cases. Chondroid chordoma was originally described as a variant of chordoma that contained cartilaginous areas indistinguishable from hyaline type chondrosarcoma, and they have better prognosis than non-chondroid chordomas.3 However, the immunohistochemical and ultrastructural features of chondroid chordomas are similar to those of classical chordomas.15
In the present study, the frequency of BNCT-like component was not different between SBCs and SCs. Unlike previous studies that focused on BNCT,11161718 our study is different in that we preferentially included chordoma cases at the beginning of the study, whereas BNCT is a benign aggregation of cells that originated from embryonic notochords; it is thought to be a potential precursor of chordoma.13 Some studies showed that the radiologic, histologic, and immunohistological features of BNCT vary1920; however, whether BNCT is a real precursor of chordoma remain controversial.21
In the present study, we evaluated BNCT-like component that mimicked the histology of true BNCT, that is, a lower Ki-67 LI than that of typical chordoma. However, although the Ki-67 LI of BNCT-like area was lower than that of typical chordoma area, but the difference was not significant. Thus, we assumed that this BNCT-like component is also a tumor component although histologically it resembled true BNCT, including even having cytoplasmic hyaline globules that have been reported to be found in true BNCT. Interestingly, three cases of intradural chordomas were included in our study. Intradural chordomas are rare and have been reported to have better prognosis than conventional chordomas.2223 In the study by Wang et al.,24 three of the six intratumoral chordomas showed large-sized cells with abundant cytoplasm and little extracellular mucus-like matrix, which is similar to the histology of BNCT. Moreover, in the current study, all three patients with intradural chordoma were alive and did not experience recurrence, and two of them had BNCT-like component along with hyaline globules. Furthermore, intradural chordoma is more likely to achieve gross total resection, which also could contribute the favorable prognosis of intradural chordoma in this study.
SC patients showed longer OS and DFS than those with SBC, but the OS was not statistically significant. These results are in contrast to previous findings that sacral chordomas have worse prognosis. This discordance might be due to the difference in treatment modalities between the two studies. In the present study, over 50% of sacral chordoma patients received complete surgical resection, whereas only 33% (4/12) of patients received gross total resection in the previous study.8 However, both previous and current studies analyzed only a small number of patients treated with variable modalities, and thus the results lack statistical power. Further studies with larger number of patients are needed.
In conclusion, our results highlight the histopathologic differences of chordomas based on anatomical location, which have not been thoroughly investigated previously. Regarding tumor location, clival/intradural chordomas are characterized by chondroid matrix and diffuse growth pattern, whereas spinal/sacral chordomas showed lobulating pattern. Pathologists should be aware that BNCT-like component may present in up to one-third of chordomas and should thus be diagnosed carefully.
 XML Download
XML Download