

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Stereotactic radiosurgery using Gamma Knife is one of the standard treatment options for brain metastases and resulted in high tumor control rates and low morbidity.12 Although gamma knife radiosurgery (GKRS) for brain metastases is expected to show low morbidity associated with irradiation due to steep dose fall-off at the tumor margin, concerns relate to the adverse effects involving large-sized tumors.
Studies report attempts to split the irradiation to decrease the treatment-related complications.345 The benefit of fractionated GKRS is disputed because of the errors caused by movement of the head frame in patients. Traditional GKRS is based on a pin-based, rigid frame system that immobilized a patient and to accurately define the stereotactic coordinate. However, a new generation of GKRS with a frameless immobilization system has rendered fractionated GKRS an increasingly favorable treatment option. This is the first report of large metastatic brain tumors treated with frameless fractionated GKS (FF GKRS) using Gamma Knife ICON™ (Elekta AB, Stockholm, Sweden). Gamma Knife ICON™ tracks patient movement during treatment using a cone beam computed tomography (CBCT), a thermoplastic mask system, and an infrared-based high-definition motion management (HDMM) camera. Since the introduction of Gamma Knife ICON™, a few patients were treated with FF GKRS for large metastatic brain tumors using these useful tools.
We performed FF GKRS for large tumors with a tumor volume ≥ 10 cm3. To investigate the effectiveness and toxicity of FF GKRS, we report a preliminary outcome of short-term clinical and radiological follow-up.
METHODS
All 15 patients treated by FF GKRS using gamma knife ICON™ over 3 or 5 consecutive days underwent imaging follow-up via contrast-enhanced magnetic resonance imaging (MRI). Patient characteristics, radiologic tumor response, and clinical progress were reviewed by medical records.
Patient characteristics
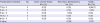
Between April 2016 and Mar 2018, 408 patients with 1,604 lesions underwent GKRS for brain metastases at the Gamma Knife Center of our institution. Of these, 15 patients with 17 lesions were treated with FF GKRS because of the large volume tumor more than 10 cm3 were included in this study. Table 1 lists the baseline patient demographics and clinical characteristics. The mean tumor volume was 19.53 ± 7.07 cm3. All patients were diagnosed with metastatic brain tumor.
Table 1
Characteristics of the 15 patients included in the study

Radiosurgical technique of FF GKRS using ICON™
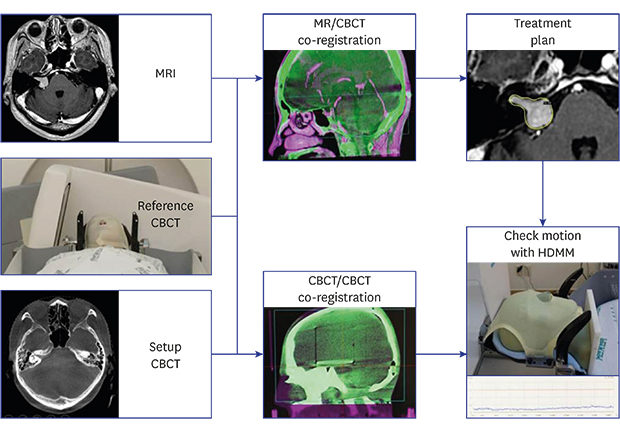
We performed thermoplastic mask-based FF GKRS for brain metastases. A brain MRI scan without Leksell frame was performed to obtain a thin-section image and a T1-weighed image with gadolinium enhancement to define the target volume. During the MRI, the patient's face was covered with a thermoplastic mask in a relaxed posture. The thermoplastic mask system consisted of customized cradles (Moldcare™; Alcare Co, Tokyo, Japan) and 3-point thermoplastic masks (Orfit® Industries, Wijnegem, Belgium). The nose portion of the mask was cut to place a single reflective optical marker on the nose of the patient's nose, which was visible in the radiation unit and served as a stable anatomic reference for motion tracking between fractions. Subsequently, we performed CBCT and co-registration with MRI scan for target localization and verification. Treatment was planned using the Leksell Gamma Plan Treatment Planning System (version 11.0.3; Elekta Instrument). Tumor margin was outlined using region and volume tool of GammaPlan software. The final target volume was defined with a tumor volume without additional margin. The prescription dose was 21 to 40 Gy in 50% isodose line and fractioned daily for 3 to 5 consecutive days via multiple isocenter plan (Table 2). The majority of fractionated GKRS for brain metastasis has been used 8 Gy × 3 fraction. However, the total dose was reduced or increased depending on the tumor location, size, and surrounding normal organ. A threshold of 5 Gy was applied to the optic apparatus per fraction perpendicular to the tumor. Intra- or inter-fractional repositioning error was limited to less than 1.5 mm through HDMM and CBCT.
Table 2
Radiosurgical parameters of the patient group
Accuracy verification
Prior to each fraction, daily CBCT was performed to verify the actual skull position. The accuracy of imaging between CBCT and stereotactic CT was within 0.5 mm in the experiment using the anthropomorphic phantom performed in the Gamma Knife Center of our institution. Based on these results, we were confident that the accuracy was maintained during treatment over several consecutive days. The movement of the patients' head was controlled within 1.5 mm using a high definition motion management system.
Follow-up
Preoperative and follow-up data were extracted from the registered patient groups. The clinical status was determined via telephone if required. Imaging tests were routinely performed with detailed neurological examinations at 1, 3, 5, 7, 9, and 12 months after FF GKRS. In addition to the change in tumor volume in MRI, the clinical findings including improvement or deterioration of the existing symptoms and appearance of new symptoms were determined. Tumor volume increase was defined as a 120% increase in tumor volume relative to the time of FF GKRS. Toxicity was graded using the Radiation Therapy Oncology Group Central Nervous System (CNS) toxicity scoring system.
Statistical analysis
Differences between groups were assessed using the Mann-Whitney test or χ2 test for continuous and categorical variables, respectively. Kaplan-Meier survival plots were used to estimate the tumor control distributions and the log-rank test (level of significance, P < 0.05) was used to assess differences between the groups. All statistical analyses were performed using SPSS Statistics (version 19.0; IBM Inc., Armonk, NY, USA).
RESULTS
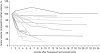
The mean duration of clinical follow-up was 12 months (range, 2–24), and the local tumor control rate was 100%. The tumor volume decreased in 13 lesions (76.5%) and remained stable in 4 lesions (23.5%). One patient with melanoma was classified as new lesion development because of the new occurrence of leptomeningeal seeding, despite the tumor volume remaining stable. Compared with the initial volume at the time of FF GKRS, tumor volume change at the last follow-up was 62.32% ± 29.80%. Fig. 1 shows the volumetric change after FF GKRS in each patient. Cumulative survival rate at 12 months was 93.3% ± 6.4%. One patient died during the follow-up period. This 40-year old men patient with a prior history of whole brain radiation therapy (WBRT) underwent FF GKRS for 3 metastatic lesions associated with non-small cell lung cancer (NSCLC). Despite the radiological decrease in tumor volume, the patient died because of progression of primary cancer at 4 months after FF GKRS.
Fig. 1
Tumor volume changes in each patient after frameless fractionated GKRS.
GKRS = gamma knife radiosurgery.
Nine patients manifested neurological symptoms at the time of FF GKRS (Table 3). Pre-existing symptoms included headache in four patients, motor weakness in two patients, and diplopia, dysarthria, visual disturbance, dizziness, seizure, and paresthesia in one patient, respectively. Four patients manifested more than one symptom, and another 6 patients exhibited no presenting symptom before FF GKRS. Of nine patients, four experienced symptom improvement after FF GKRS, and five remained stable. One patient with motor weakness before treatment remained stationary after FF GKRS. One patient with visual disturbance due to parieto-occipital lesion, one with diplopia, and other patients with headache and paresthesia were not improved after FF GKRS. Four of the patients experienced symptoms afresh. Tolerable headache controlled by medication was reported in one patient. Another one patient exhibited motor weakness, which disappeared in one of them. One patient with melanoma complained of progressive dizziness, and leptomeningeal seeding was found afterward. Subjective memory disturbance was noted in one patient who underwent FF GKS for metastatic tumor in frontal lobe from breast carcinoma. The median Karnofsky Performance Status score at the final clinical follow-up was 100. No patient showed radiation necrosis in the follow-up. Fig. 2 represents illustrative cases of four patients with favorable response to FF GKRS.
Table 3
Clinical course of neurological symptoms after FF GKRS
Fig. 2
Illustrative cases of four patients with favorable response to FF GKRS. (A) This 65-year-old female patient with history of NSCLC felt dizziness and underwent FF GKRS for large metastatic lesion on Lt frontal convex. The initial tumor volume was 27.084 cm3, but slowly decreased until 17 months after FF GKRS using 9 Gy for 3 consecutive days. (B) This 37-year old female patient was diagnosed as NSCLC and treated by Alectinib. Her neurologic symptoms were headache and vomiting, and she underwent FF GKRS for the large metastatic tumor of 22.701 cm3 located nearby the posterior horn of left lateral ventricle. The radiosurgery parameter was 3 Gy with 3 fraction for 3 consecutive days. After 5 months after FF GKRS, the tumor nearly disappeared. (C) This figure shows a case of 59-year-old male with NSCLC treated by wedge resection. Brain metastasis with 22.124 cm3 was incidentally found, and the tumor showed dramatic decrease until 3 months after FF GKRS using 8 Gy with 5 fraction. (D) The patient of this figure was 64-year-old female newly diagnosed with NSCLC and brain metastasis. After FF GKRS using 8 Gy with 5 fraction, the metastatic lesion of 31.413 cm3 showed gradual decrease.
FF GKRS = frameless fractionated gamma knife radiosurgery, NSCLC = non-small cell lung cancer.

When defining tumor control failure as local control failure, clinical death, or new lesion development, two patients with four lesions were classified into tumor control failure group. There was no statistically significant relationship between fractionation schedule and tumor control failure (Table 4).
Table 4
Clinical outcome according to fractionation schedule
When comparing the CBCT and preoperative CT images, the inter-fractional movement was less than 0.5 mm. Daily difference in intra-fractional movement was 0.1 mm with a maximum error of 0.5 mm in HDMM system. The accuracy of HDMM system was 0.1 mm with a maximum error of 0.5 mm.6 We also performed an experiment using an anthropomorphic phantom and validated the accuracy of co-registration with a difference of less than 0.5 mm between the CBCT and stereotactic CT image.
DISCUSSION
When treating large-volume tumors, fractionation yielded the four R's of radiobiology: repair of normal tissue, reoxygenation of tumor hypoxia, redistribution into radiosensitive cell cycle stages, and repopulation. In tumors with large volume and adjacent to the eloquent area, complete surgical resection without postoperative complications is almost impossible.78 Radiosurgery is indicated in such cases. The current therapeutic dose for brain metastases may be excessive and not appropriate due to adjacent normal tissue, such as the optic apparatus or brain stem. Traditional single-session radiosurgery resulted in adverse radiation effects without rapid volume reduction.9
Despite the poor radiobiological bases of fractionated radiosurgery, a few studies using LINAC-based instrument showed that fractionated radiosurgery was safe and effective in brain metastases.101112 Aoyama et al.11 treated 87 patients with 35 Gy in 4 fractions, and concluded that fractionated radiosurgery is as effective as single-session radiosurgery with minimal toxicity. Kim et al.10 compared single-session and fractionated radiosurgery for brain metastases in 98 patients. In their study, fractionated radiosurgery showed minimal toxicity and superior tumor control when compared with single-session radiosurgery, especially for large-volume tumors. However, few studies reported fractionated GKRS for brain metastases. A few studies investigated fractionated GKRS for brain metastases using several fractionated schemes.31314 They performed separate radiosurgeries at 1 to 4-weeks intervals, and showed symptomatic improvement of 74% without complications,13 and a local control rate of 89.8% with a volume reduction rate of 39.8%.15
Our group previously reported that fractionated GKRS resulted in satisfactory tumor control and low morbidity in case of large brain metastases > 10 cm3.16 In the published study, we analyzed the efficacy and toxicity of hypofractionated GKRS to treat metastatic brain tumors for which surgical resection were not considered as the primary treatment option. The previous study included 36 patients with 40 cases, and the mean gross tumor volume was 18.3 cm3. The median dose was 8 Gy at 50% isodose line with 3 fractions, which was similar to this study. The cumulative survival rate at 1 and 2 year was 66.7% and 33.1%, respectively. The local tumor control rate was 90% and grade 3 or higher toxicity was 2.7%. In the previous study, we proposed the indications for fractionated GKRS as follows: 1) large tumors with a volume greater than 10 cm3, 2) tumors adjacent to eloquent areas such as the optic apparatus or brain stem, and 3) previously irradiated tumors.
However, pin-based fractionated GKRS was a difficult method for patients with brain metastases. We interviewed patients who were exposed to FF GKRS using mask-based immobilization and found that it was certainly more comfortable for patients receiving GKRS for brain metastases. Another disadvantage of the pin-based, rigid head frame system is the lack of reproducibility once it was removed. To overcome this problem, an advanced instrument, Gamma Knife ICON™, was developed to facilitate fractionated radiosurgery as well as frameless fixation. This instrument enabled on-board verification of patient position and correction using a quality CBCT system. In addition, the intra-fraction patient position was monitored using an optical tracking system and the treatment delivery was controlled for positional excursion from the planned treatment position. Using these tools, fractionated and frame-based Gamma Knife ICON™ ensured treatment efficacy.6 This study showed that the HDMM system was accurate with an error of almost 0.01 mm and a maximum of 0.05 mm. Other studies also showed that mask-based immobilization using Gamma Knife ICON™ reduced the mean width of the inter- and intra-fraction movement to within 1 mm.17
After introduction of FF GKRS using Gamma Knife ICON™, our group has performed FF GKRS based on this assumption. We investigated the feasibility of FF GKRS using mask-based immobilization. Our results showed that FF GKRS reduced radiation-induced complications and facilitated patients with brain metastases adjacent to the eloquent area, large volume tumors, and those previously exposed to radiation. Our results were similar to those of previously published data using hypofractionated GKRS using frame, showing a local control rate of 94.1% and a volume reduction rate of 27.7% for large brain metastases. In contrast to other investigators suggesting fractionation intervals between GKRS sessions to reduce radiation toxicity, we performed dose-fractionated GKRS on a daily basis. Notably, daily fractionated GKRS showed no radiation-induced complications for brain metastases despite high irradiation doses.
Clinical studies with Gamma Knife ICON™ have rarely been reported. This study demonstrates that FF GKS using Gamma Knife ICON™ is safe and effective for the treatment of large metastatic brain tumors. Our results showed local tumor control rates of 89.8%, similar to other published data with a local control rate of 70% to 90%.18192021 Longer follow-up is required for consolidation of the results, whereas FF GKRS using Gamma Knife ICON™ is a sufficiently reliable modality for large metastatic brain tumors based on the current study.
GKRS is also indicated as a salvage treatment for patients with recurrent tumors in spite of previous radiosurgery or WBRT. This present study included 8 patients who underwent radiosurgery or WBRT prior to FF GKRS. The indications for repeated GKRS in recurrent brain metastases remain unclear in terms of morbidity due to irradiation. However, our results show that repeated GKRS is effective for recurrent large metastatic brain tumors. There results have been corroborated in other studies, which showed no radiation-induced complication in 16 patients treated with an average of 2.6 cycles of radiosurgery.22
The complication rate of GKRS for brain tumors was reported at 1%–2% in previous studies.923 However, GKRS is associated with irreversible toxicity due to radiation. Therefore, fractionated GKRS promotes tolerance by adjacent normal tissues and intracranial tumor control in multisession radiosurgery.52425 We previously reported the efficacy and toxicity for the treatment of large metastatic brain tumors using fractionated GKRS with pin-based immobilization resulting in effective tumor control and low toxicity rates.26 We have shown that fractionated GKRS is a possible indication for tumors adjacent to the eloquent area or tumors irradiated previously. In our experience, no acute complication due to radiation was detected after daily consecutive FF GKRS in cases diagnosed with brain metastases.
This study reports the preliminary experience at a single institution using Gamma Knife ICON™, an advanced gamma knife system for FF GKRS. However, the relatively short follow-up duration and lack of prospective assessment of patients' progress is a limitation. Inconsistent radiological evaluation is another limitation. The effect of histology and radiosensitivity to radiosurgery may also confound the effect of FF GKRS due to the varying histology of patients included in this study. Further, eight patients were treated with concurrent chemotherapy regimen, including ceritinib, gefitinib, and erlotinib, and it is unclear whether tumor response was due to FF GKRS in these patients. The optimal dose and fractionation regimen for brain metastases has yet to be determined.
In this study, we demonstrated that daily application of FF GKRS by Gamma Knife ICON™ to patients with large metastatic brain tumors is an alternative to surgical resection or single-session radiosurgery, especially for patients with large-volume tumors. Daily FF GKRS by Gamma Knife ICON™ showed satisfactory tumor control rate and low morbidity compared to those of fractionated GKRS using frame, despite the short follow-up period. Further prospective studies with longer follow-up of large cohorts of patients diagnosed with brain metastases are required to elucidate the therapeutic effect of FF GKRS.
 XML Download
XML Download