

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The cutaneous innervation of the dorsum of the foot shows various branching patterns. Dorsum skin is supplied by the terminal branches of tibial nerve and common peroneal nerve. Branches of the superficial peroneal nerve (SPN) supplies major portion of the dorsum of the foot and toes except the areas supplied by the deep peroneal nerve (DPN) and sural nerve (SN).
SPN which is a branch of the common peroneal nerve in the lower third of the leg pierces the deep fascia and becomes cutaneous. It divides into medial and lateral dorsal cutaneous nerves, which in turn gives off dorsal digital nerves to supply the skin over the dorsum of the foot and the digits. SN supplies the lateral side of the fifth toe, saphenous nerve supplies the medial border of the foot up to the base of the great toe and the DPN supply the skin of the first interdigital cleft. Dorsal branches of the medial and lateral plantar nerves supply the nail beds [1].
SPN can be easily subjected to entrapment as it penetrates deep fascia of leg. It can also be affected in compartment syndrome of the lateral compartment of the leg. Clinicians working in emergency set up always come across patients who have injury to the dorsum of the foot that necessitate anesthesia for repair. As the major part of the dorsum of the foot is innervated by SPN, regional block of this nerve guarantees quick anesthesia of this area [2]. According to review by Asp et al. [3] on SPN it was concluded that SPN has highly variable anatomy from its origin at the level of the knee to its terminal branches to the dorsum of the foot. The key anatomical locations where the nerve is at risk includes many points in its course including over the first metatarso phalangeal joint which is supplied consistently by a medial dorsal cutaneous branch of the nerve [3]. The SPN is also at risk of injury in anterior ankle arthroscopy or fracture of ankle [4].
SPN and SN are used as donor nerve especially when multiple and very long nerve grafts are necessary. They have been harvested with good results [567]. Knowledge of such variations are essential for both orthopedic and trauma surgeons. Therefore, this study is conducted to know the different patterns of nerve distribution on the dorsum of the foot and also to compare it with earlier studies.
Go to : 
Materials and Methods
Forty formalin fixed lower limbs (30 males and 10 females) of adult cadavers without specification to the side it belongs were dissected in the Department of Anatomy, Kasturba Medical College, Manipal Academy of Higher Education, Manipal. The specimens are dissected as per the instructions given in Cunningham's manual of Anatomy [8]. The pattern of cutaneous innervation on the dorsum of the foot were carefully dissected, noted, classified into four groups and photographed. Group I is a classical pattern in which DPN supplying first interdigital cleft region, SN on lateral side of fifth toe, saphenous nerve along medial side of dorsum upto the base of big toe and SPN supplying remaining part of the dorsum. In group II, SPN supplies the entire dorsum except its medial and lateral sides. In group III, SN supplies lateral 2 1/2 toes, first interdigital cleft is supplied by DPN and remaining part is by SPN. In group IV, DPN communicates with the medial division of SPN and supplies first interdigital cleft, SN to the lateral side of the fifth toe and SPN to remaining part of the dorsum.
Go to :
Results
Results obtained in our study were classified into four groups as follows.
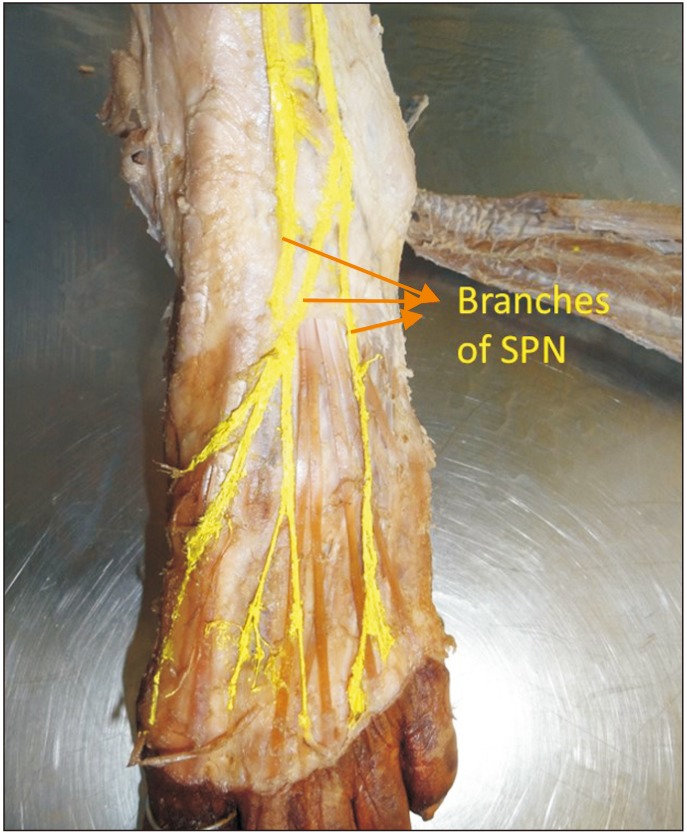
Group I (Fig. 1): DPN supplying the skin over first interdigital cleft; SN, lateral side of the fifth toe; SPN, remaining part of the dorsum in 18 limbs (45% of specimens).

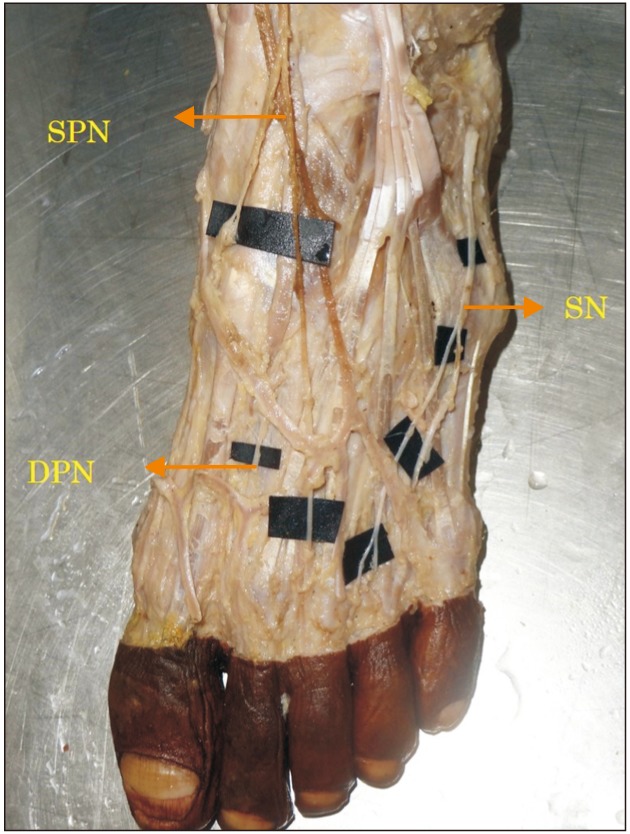
Group II (Fig. 2): SN, lateral side of fifth toe; SPN, remaining part of the dorsum in 12 limbs (30% of specimens).
Group III (Fig. 3): SN, lateral 2 1/2 toes; DPN, first interdigital cleft; SPN, remaining part of the dorsum in 6 limbs (15% of specimens).
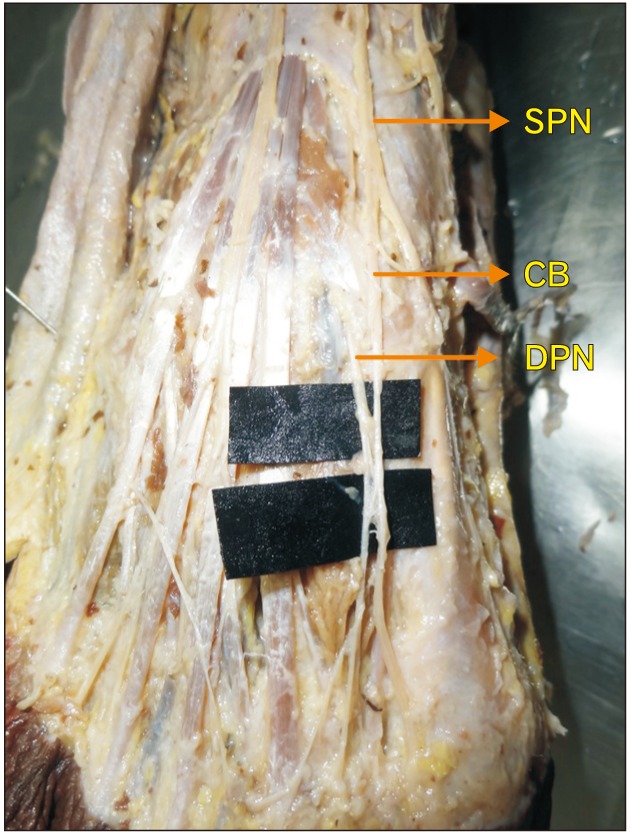
Group IV (Fig. 4): DPN communicates with the medial division of SPN and supplies first interdigital cleft. SN, lateral side of the fifth toe; SPN, remaining part of the dorsum in 4 limbs (10% of the specimens).
Go to :
Discussion
In a study, 35.38% specimens the lateral side of the fifth toe was supplied by SN and rest was by SPN [9]. In our study, 30% of cases had this pattern. In the same study, 24.61% specimens lateral 2 1/2 digits were supplied by SN. In our study, 15% were supplied in this way. The innervation patterns found in other groups were not found in our study.
The most common distribution of the SN in the foot was to the lateral side of the fifth toe seen in 60% of specimens, in contrast we got 90%. In 26.7% cases, the SN supplied lateral 2 1/2 digits [10], whereas in our study it is seen in 15% of the cases.
In a study conducted by Drizenko et al. [11], the communicating branches between SN and SPN were seen in more than 50% of cases. In our study, communication between SPN and DPN were seen only in 10% of cases.
Prakash et al. [12], found in 33.33% cases an additional branch of SPN called as accessory DPN which was seen supplying the ankle and dorsum of the foot. Wahee et al. [13] found a variation pattern in 53.3% of cases which is similar to our group I, i.e., first interdigital cleft by DPN, lateral border of fifth digit by SN and remaining by SPN [13].
Four distinct patterns of innervation was observed by Gupta et al. [14]. In 55% of cases, our group I type of innervation was seen (i.e., SN on lateral border of fifth digit, DPN in the first interdigital cleft, rest of the dorsum by SPN). In 35% cases, the pattern is similar to our group III (i.e., SN, lateral 2 1/2 toes; DPN, first interosseous space; SPN, remaining part of the dorsum). In the same study, the communicating branches were found between SPN and DPN in 25% cases, between SPN and SN in 15% of cases. A study conducted on communicating branches between SPN and SN of the foot 58% of the cases found to have communicating branches [11]. The rich sensory innervation of foot is manifest through the communicating branches linking the neural trunks. In our study the communicating branch was found between SPN and DPN in 10% of cases. There was no communicating branch found between SPN and SN. The knowledge of communicating branches and their variations will help to decrease iatrogenic injury to the nerve.
Numerous variations do exist in the cutaneous innervation of the dorsum of the foot. Knowledge of such variations are useful for physicians while assessing sensory deficits and pain on the dorsum of the foot. The cutaneous nerves are at risk of iatrogenic injuries during surgeries involving ankle, open reduction and internal fixation of fracture, arthroscopy, local anesthetic block, nerve grafting, and surgical decompression of neurovascular bundle [15]. Therefore, a detailed knowledge of the cutaneous innervation pattern is helpful in diminishing the damage to these nerves during operative procedures.
Go to :
 XML Download
XML Download