

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
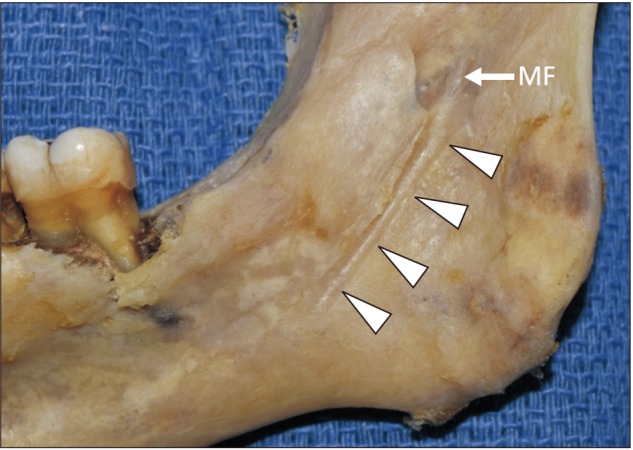
The nerve to the mylohyoid (NM), which is also known as “nervus mylohyoideus,” originates from a branch of the mandibular division (V3) of the trigeminal nerve [1]. It branches from the inferior alveolar nerve (IAN) before the IAN enters the mandibular foramen [23]. The NM, then, courses in the mylohyoid groove (Figs. 1, 2) or canal situated on the medial aspect of the mandibular ramus [1234]. The nerve then gives off motor branches, which penetrate the inferior aspect of the mylohyoid muscle and the anterior belly of the digastric muscle [12345]. The NM contained sensory fibers per one histological study [6] and might provide sensory branches to the mandibular teeth [34789101112]. One study suggested that the NM supplies sensation to the premolar, canine, and incisor teeth with a frequency of approximately 60% [13]. The NM might also provide cutaneous branches (with a mean number of 2.3 [14]) to the skin of the chin [15], which was first described by Valentin in 1843 [16]. Fujii et al. (2015) [17] evaluated the magnetic resonance imaging (MRI) retrospectively and concluded that the NM was difficult to detect on MRI due to its small diameter. Heasman and Beynon [18] performed a histological observation of the NM and showed a mean fiber count of 1,251. Interestingly, the number of nerves in the edentulous mandible was significantly less than those in non-edentulous subjects [18].
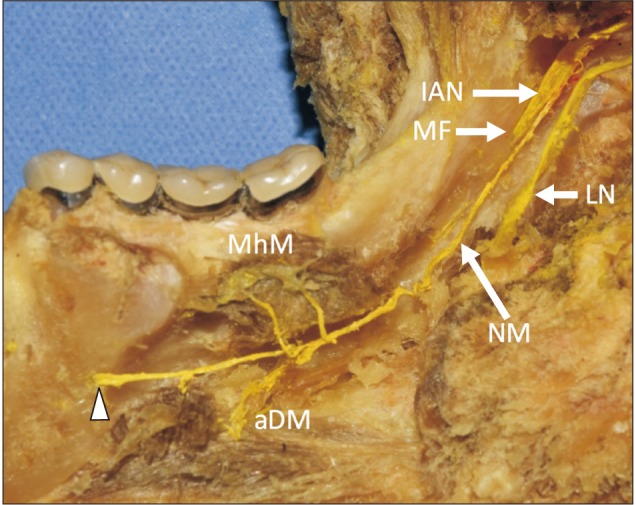 | Fig. 2The nerve to the mylohyoid derived from the inferior alveolar nerve (IAN), provides the motor branches to the mylohyoid and anterior belly of digastric muscles and enters the lingual foramen (arrowhead). aDM, anterior belly of digastric muscle; LN, lingual nerve; MF, mandibular foramen; MhM, mylohyoid muscle; NM, nerve to mylohyoid.
|
Go to : 
Anatomic Variations of the NM and the Mylohyoid Groove
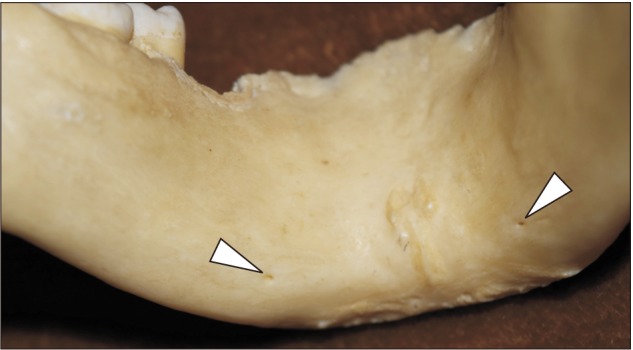
In 43%–50% of the population, the terminal branches of the NM penetrate the lingual aspect of the mandible via the lingual foramina or lateral lingual foramina (Figs. 3, 4), which is located in the midline of the mandible or just below the premolar region, to innervate the mandibular incisors or premolars and related gingivae [11920]. Moreover, the branching point of the NM from the IAN is described to be 13.4 to 14.7 mm proximal to the mandibular foramen [121]. Kumar et al. [22] observed a NM branching directly from the mandibular nerve trunk in 10% of specimens (5/50). In these five cases, all of the NMs ran posteromedial to the IAN [22]. Although most unusual connections between the NM and the lingual nerve (LN) have been reported as case reports [32324], Sato et al. [25] investigated this anomaly and revealed that in 1.45% of cases (6/413), one or two large branches of the NM connected with the LN in the submandibular or submental triangles. This incidence was significantly different from that reported by Kameda (1952) [26] who identified communicating branch of the LN and NM in the submental triangle in 46.3% of the cases (74/160). According to Potu et al. [3], an unusual communicating branch between the LN and NM was identified after the LN passed proximal to the lower third molar tooth. The NM often gives off several branches to the muscles and can also give a branch to the submandibular gland [27].

Other documented variations of this nerve include it originating from the glossopharyngeal nerve or the LN and communicating with a dental branch of the IAN [23]. The NM may also travel within the mandibular canal instead of underneath the mylohyoid groove and is often doubled through accessory foramina in the mandible [23].
The morphology of the mylohyoid groove is variable [28]. Endoscopy has used to visualize the mandibular foramen and related structures and demonstrated that the mylohyoid groove could be doubled, narrowed, or occasionally covered by a bony bridge [29]. The frequency of mylohyoid bridging has been reported as 10.99% (21/191) [30], 10.0% (4/40) [31], and 6.0% (3/50) [32]. Fabian concluded that the formation of the medial wall of the mandibular foramen and/or attachment of the sphenomandibular ligament onto the lingula leads to variations in location of the mylohyoid groove [33]. Iwanaga et al. [34] reported a case of mylohyoid canal that was found on computed tomography with multiple accessory foramina of the mandible. The data from Stein et al. [5] suggest that a mandible has an average number of 36 foramina.
Go to :
Association of Failed IAN Blockade to the Variations of the NM
The IAN block is the most commonly used anesthetic technique for mandibular surgeries including dental treatments [19]. However, it carries a significant failure rate that ranges from 38% to 90% [519]. Even experienced endodontists occasionally have difficulty with total IAN block due to the anatomical complexity and variability [13819]. The presence of accessory sensory branches of the NM to the mandibular incisors might contribute to a failed IAN block [13819].
In the presence of such fibers that travel through the lingual foramen with a higher-than-anticipated branching point of the NM from the IAN within the infratemporal fossa, the NM may avoid immersion by the anesthetic agent during the procedure [158]. Additionally, Stein et al. [5] reported that the sphenomandibular ligament may form a physical barrier, further contributing to a failed anesthesia. Therefore, patients may initially display the signs of successful anesthesia, such as diminished skin sensation in the V3 distribution, but complain of pain upon initiation of the procedure i.e. when the incisors and gingivae are stimulated [18]. Furthermore, Potu et al. [3] claimed that a connection between the NM and the LN may also contribute to a failed mandibular nerve block. Stein et al. [5] further explain that the mandibular teeth receive sensory innervation from a plexus of nerve fibers.
The location of the mandibular foramen is a crucial landmark in IAN blockade [7]. However, many anatomical variations of the foramen also exist and, thus, may also contribute to a failed nerve block [7]. The insertion of a needle into the pterygomandibular space may not only lead to a transient or permanent paresthesia by severing sensory fibers of the NM, but it may also cause cardiovascular and visual complications due to IAN's close proximity to other neurovascular structures [7]. Moreover, an infective abscess within the pterygomandibular space may also form postoperatively [7].
To avoid such complications, Altug et al. [7] suggested a simpler and easier alternative to an IAN block i.e., a NM block, which is given supra-periosteally, to produce an equally effective anesthesia as that of an IAN block that requires insertion of a needle into an anatomically complex space [5]. Stein et al. [5] attributed the effectiveness of a NM block to the diffusion of the anesthetic agent into the thin mandibular cortical bone and that this method is effective as a supplement to an IAN block. However, Clark et al. [19] reported that a NM block, with or without a concomitant IAN block, does not provide or enhance anesthesia to the mandibular incisors and adjacent gingivae. Tubbs et al. [23] recommended a “high mandibular nerve block”.
Go to :
Blockade of the NM
According to Altug et al. [7], to prevent any IAN injury during mandibular implants, NM and buccal nerve blocks can be considered as an alternative method for an IAN block. However, the NM innervation to the lingual cortical bone might only be supplemental and the blockade of the NM itself might not anesthetize the lower molar teeth [7].
Go to :
Injury to the NM during Maxillofacial Surgery
Potu et al. [3] described a case of a NM that was connected to the LN at a point close to the molar tooth, an anatomic variation that predisposes one to a nerve injury upon tooth extraction [23]. Injury to such a network of nerve fibers may result in a sensory loss of the anterior two-thirds of the tongue [323].
A transient or permanent sensory deficit around the skin of the chin, without affecting the sensation of the lower lip [235], has been reported following removal of the submandibular gland, during which the gland is physically separated from the NM [2233536], a bilateral sagittal split osteotomy (BSSO) [4], and post-genioplasty [35].
Guyot et al. [35] reported a case of 20-year-old male who received a genioplasty after which he complained of transient bilateral hypoesthesia over the inferior surface of the chin and around the mental prominence even though the mental nerves were not damaged during the procedure and attributed the unusual presentation to a damage to cutaneous branches of the NM [27].
Go to :
Relationship of Mandibular Fracture to the Mylohyoid Groove
Mensink et al. (2014) [31] performed a standardized BSSO on 40 cadaveric hemi-mandibles to investigate the relationship of a lingual fracture line and the mylohyoid groove. Thirty percent of the lingual fracture lines (12/40) ran through the mylohyoid groove, showing their significant relationship [31]. After leaving the inferior border, 37.5% of the lingual fracture lines (15/40) ran parallel and inferior to the mylohyoid groove toward the horizontal bur cut [31]. While 7.5% (3/40) ran parallel and superior to the mylohyoid groove, 17.5% (7/40) crossed the mylohyoid groove and ran toward the horizontal bur cut [31]. The hypothesis that the mylohyoid groove would function as the pathway of least resistance for the lingual fracture was only partially confirmed [31].
Go to :
Other Clinical Considerations
Tubbs et al. [36] performed a feasibility study of using the NM as a donor for a facial nerve reanimation procedure. Their study found that the NM could easily be transposed to the facial nerve stem with limited morbidity.
Go to :
Conclusion
As can be seen, variations of the NM can result in unusual clinical and thus has clinical relevance. According to He et al. [20], the variations are crucial to note for an implant over an edentulous mandible, tori removal, harvesting a graft, and screw placement post-trauma in addition to the clinical implications described in this review. Therefore, in order to minimize complications and improve the prognosis of invasive mandibular procedures, surgeons must always be knowledgeable of variations of the NM. Finally, it is also crucial to warn patients, prior to a surgery, of the possible clinical manifestations as described in this review [37].
Go to :
 XML Download
XML Download