

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Adequate knowledge regarding the anatomical variations in the origin and course of the testicular artery is very important as any compression of the testicular artery may lead to loss of gametogenesis and hormone production as it the main artery supplying the testis. The male gonadal arteries, i.e., the testicular arteries are one of the paired vessels arising from the anterolateral aspect of the abdominal aorta at the level of the second lumbar vertebra, usually inferior to the level of the origin of the renal artery. In its usual course, it passes downwards and laterally towards the deep inguinal ring. It is accompanied by the corresponding testicular vein on its lateral side and supplies the testis.
Anatomical variations regarding the number, origin and course of the testicular arteries have been described by many authors. Variation of the gonadal arteries is reported to be more common in females than in males and its prevalence in high on the right side than on the left side [1]. Unusual course of testicular artery is important in many surgical procedures. Surgeons should have a thorough knowledge about the morphologic variations of these arteries and ensure that they are not neglected as any injury to this artery can lead to compromising oxygenation of the gonads which might cause testicular atrophy. We report in here a clinically important variation of the left testicular artery and associated abnormality of the left renal vein.
Go to : 
Case Report
The case presented below was noted incidentally, in a 60-year-old male cadaver during routine dissection. The left testicular artery had a high origin from the anterior aspect of the abdominal aorta, just behind the upper part of the left renal vein. Its origin was at the same level as the origin of left renal artery. In its further course, the left testicular artery passed through a hiatus present in the left renal vein (Fig. 1). The left testicular artery passed medially near the median plane because of its course through the renal hiatus. The hiatus was formed by the incomplete fusion of the two embryonic left renal veins. The left testicular vein drained into the left renal vein proximal to the hiatus. After passing through the hiatus, the testicular artery coursed downwards lateral to the testicular vein. The rest of the course of the testicular artery was normal. No anomalies were found in the right gonadal vessels. The left testis also appeared to be normal. A schematic diagram depicting this case is shown in Fig. 2.
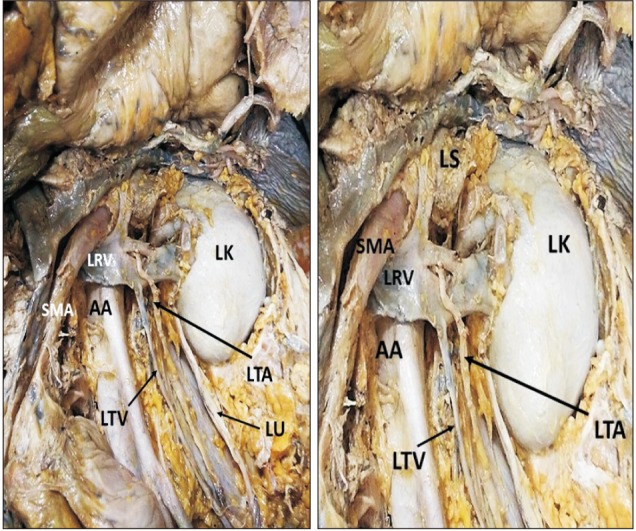 | Fig. 1Dissection of the abdomen showing the left testicular artery (LTA) passing through a vascular hiatus in left renal vein (LRV). AA, abdominal aorta; LK, left kidney; LS, left suprarenal gland; LTV, left testicular vein; LU, left ureter; SMA, superior mesenteric artery.
|
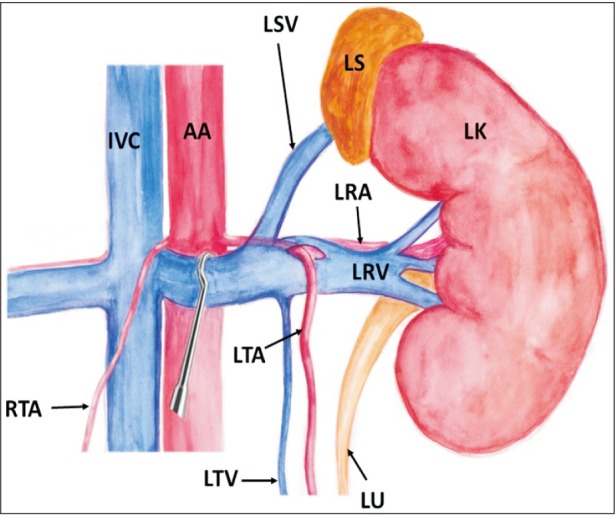 | Fig. 2Schematic diagram showing the course of left testicular artery (LTA) through a hiatus in left renal vein (LRV). AA, abdominal aorta; IVC, inferior vena cava; LK, left kidney; LRA, left renal artery; LS, left suprarenal gland; LSV, left supra renal vein; LTV, left testicular vein; LU, left ureter; RTA, right testicular artery.
|
Go to :
Discussion
Variations in the origin and anatomical relationship of the testicular arteries to the renal vessels are frequently reported in literature. However, reports on the unusual course of testicular artery is scanty. With the advent of newer surgical and diagnostic techniques, understanding of any atypical anatomical presentations have gained enormous importance. High origin of left testicular artery and its arching over the left renal vein [2], bifid testicular artery [3], and testicular artery arising from a common trunk or be doubled, tripled or quadrupled [4], left testicular artery originating from the inferior renal artery [5] are few reported variations. It has been observed that testicular artery variations are commonly associated with the variations of the renal vessels [6]. This fact is attributed to their complex embryological origin.
Bifurcation of left renal vein [7], and right testicular artery passing through a bifid right renal vein has also been reported [8]. But, the anomalous course of left testicular artery passing through a vascular hiatus in the renal vein is very rare. Such abnormal course could lead to the entrapment of the testicular artery and compression of left renal vein. Knowledge regarding this variation and its relation with renal vein could avoid complications in operative surgery.
Anatomical variations of testicular artery is attributed to their embryological origin which is very complex. Nine lateral mesonephric arteries are divided into the cranial, middle and caudal group. From those branches generally, caudal one develops as a definite gonadal artery and others atrophy [9]. A persistent cranial lateral mesonephric artery might have resulted in the high origin of the testicular artery as seen in the present study. It is assumed that a highly complex embryological development of the left renal vein compared to its right counterpart results in greater clinically significant variations of the left renal vein. In early human embryo, two renal veins are present on each side of the body, one dorsal and the other ventral, whereas at 45 mm stage of embryo, only a single renal vein is found [10]. Thus the presence of a hiatus in the left renal vein, as in our case, may be due to the incomplete fusion of the two embryonic renal veins. The course of the testicular artery through the hiatus in the renal vein may be explained by considering that in the course of development, the testicular artery reaches the testis after passing between the two persistent embryonic renal veins.
Vascular variations are clinically silent and remain unnoticed until discovered during venography, surgery or autopsy. This variation is immensely important because of its implications in renal transplantation, renal surgery, vascular surgery, uroradiology, and gonadal surgeries. Anomalous course of testicular artery through the renal vein restricts the availability of vein for mobilization procedures and must be well preserved to avoid the possible complications resulting from damage to it [11]. The testicular artery may get compressed in the hiatus, which may lead to degeneration of the testis. Presence of vascular hiatus in the left renal vein might lead to nutcracker syndrome and reduced blood flow in the renal vein. This condition also leads to retrograde blood flow from the left renal vein into the left testicular vein and may hence be manifested as varicocele in men [12]. This variation is thus important, not only from a surgery standpoint, but also from a physiological prospective. Hence, unusual course of the testicular artery is worth reporting in efforts to educate clinicians involved in abdominal and urogenital surgical procedures.
Go to :
 XML Download
XML Download