

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The sternum is comprised of three distinctive portions: manubrium, body (gladiolus), and xiphoid process [1]. The first portion, the manubrium, articulates with both the clavicle and first rib and is therefore fixed in position [2]. The second portion, the body, serves as the articulation point for ribs two though seven [2]. Lastly, the xiphoid process, contributes minimally to the articulation of the seventh rib [2]. The principle function of the sternum during respiration, is to serve as the link between the left and right portions of the thorax [2]. Even though the xiphoid process contributes minimally to the chest wall anatomy and physiology, it has importance in the epigastrium as it serves as an attachment site for regional muscles and soft tissues, i.e., the aponeurosis of the internal and external abdominal oblique muscles, rectus abdominis muscle anteriorly, and the diaphragm posteriorly [3]. Herein, we report an elongated xiphoid process that protrudes dorsally in the shape of a “hook.” Few have reported a dorsally hooked xiphoid process [4]. The hook-shaped xiphoid process has possible clinical consequences associated with it, e.g., mimicking an epigastric mass [5]. This has the potential to lead to unnecessary medical procedures that could be avoided by understanding anatomical variations of the xiphoid process. This case is presented to clinicians, cardiothoracic surgeons, radiologists, and anatomists in order to further our knowledge of anatomical variations that are present with the xiphoid process in order to decrease potential clinical/surgical complications.
Go to : 
Case Report
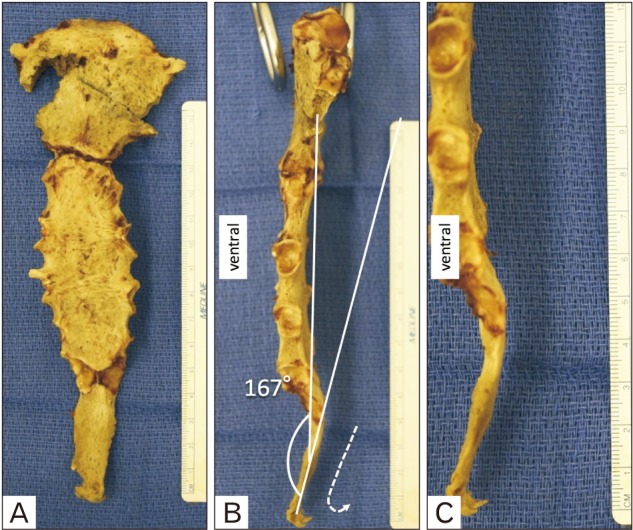
During routine dissection of a fresh-frozen cadaveric specimen, a 44-year-old at death Caucasian male was found to have an elongated and hook-shaped xiphoid process that protruded dorsally (Fig. 1). Measurements were taken using a digital microcaliper (Mitutoyo, Kanagaw, Japan). The measured length, width, and thickness of the xiphoid process were 54.2 mm, 17.1 mm, and 4.6 mm, respectively. Sternal body and manubrium lengths were 83.5 mm and 60.0 mm, respectively. The angle from the sternal body to xiphoid process was 167°. The attachments of the muscles to the sternum, including the xiphoid process, were normal. During extraction of the sternum from the rib cage, the manubrium was slightly fractured but no other anatomical variations were identified.
Go to :
Discussion
Various anatomical variations of the xiphoid process have been reported and include a bifid, trifid, pointed, flat, wide, deflected or curved shape [678]. Akin et al. [9] documented variations of the xiphoid process in 500 patients using multidetector computed tomography. Ventral deviation of the xiphoid process was present in 327 out of the 500 patients and accounted for the majority of xiphoid variations at 65.4% [9]. However, only three out of the 500 patients (0.6%) presented with a hook-shaped xiphoid process that protruded dorsally. Mean length, width, and thickness were 50 mm, 22 mm, and 7.3 mm, respectively [9]. Xie et al. [5] reported that the mean length, width, and thickness was 60.31, 23.42, and 8.25 mm in 943 sternums (41 cadavers and 902 patients), respectively.
Ateşoğlu et al. [10] reported that mean length, width, and thickness were 39 mm, 22 mm, and 6.6 mm in 97 adult males. Our findings illustrate a similar or above average length of the xiphoid process but a width and thickness that is less than the mean found in these studies. Empirically, it is thought that the mean length of the xiphoid process is approximately 2–3 cm. However, recent studies using computed tomography have revealed the mean length to be 4–6 cm, which is much longer. These differences might result from the difficulties in the visualization of the cartilaginous part of the xiphoid process or its differentiation from neighboring soft tissues [10].
Xie et al. [5] found that the dorsal, hook-shaped protrusion of the xiphoid process variation was present in 19 out of 943 (2.0%) cases and was found only in type II (pointed shape) processes. Mashriqi et al. [11] described a bifid xiphoid process that was orientated in the anterior direction which could also possess the risk of appearing as an epigastric mass during imaging. Even though various unusual variations of the xiphoid process can resemble an epigastric mass, directionality (anterior vs dorsally curved) of the variant could pose a red flag in terms of fractures involving the xiphoid process. Due to the liver's proximity dorsal to the xiphoid process, the hook-shaped xiphoid process is already angled closer to the liver than when normally observed. A fracture of the xiphoid process could potentially puncture the liver or the heart during, for example, cardiopulmonary resucitation. Therefore, our case report illustrates the rare anatomical finding of a hook-shaped xiphoid process that is orientated dorsally and the potential complications that may arise with such anatomy.
Overall, this unusual finding of a xiphoid process serves to provide a better understanding of current anatomical variations that exist pertaining to the xiphoid process [1121314]. Further, it provides a means of proper diagnosis during imaging and surgical interventions.
Go to :
 XML Download
XML Download