

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The process of aging is an important factor that contributes to changes in the body throughout life and the rate of impact of aging differs widely between individuals [1]. During life, all the various body systems change with aging including the nervous, respiratory, cardiovascular, and musculoskeletal systems. Changes were found in both organ structures and functions [2]. The cardiovascular system is of particular interest in age-related research as cardiovascular disorders have been a leading cause of the high prevalence of mortality in major populations [34]. The heart valves are complex structures which project from the heart wall and maintain the unidirectional blood flow throughout the heart despite having different structural characteristics [5]. In general, the human heart valve opens and closes about forty million times per year. Therefore, during an average lifetime they close and open over three billion times [6]. Morphological changes of the heart valves are affected by age and these changes in the valvular anatomy and physiology result in the alteration of organ function, affecting longevity. There are several previous studies about age changes of the heart valves in human such as gross morphology by dissection in donor cadavers and autopsy [78910], histological assessment of microstructural changes in the valve [10111213], and echocardiography [1415]. For the histology, collagen, elastin, and glycosaminoglycans there were changes which were seen with age. The echocardiography can be used for examination the valve circumference, orifice area, and diameter in patients. In this review, we aim to describe the age-related changes of the anatomy of the heart valve in humans. Data is being presented pertinent to the detailed anatomy of all types of heart valve, morphological changes with age, heart valve diseases, and treatment for valve dysfunction in human.
Go to : 
Anatomy of the Heart Valves
The major valves within the heart are the tricuspid, pulmonary, mitral, and aortic valves [1617]. The orifices of the heart valves are defined by the fibrous skeleton which is composed of many densely packed collagenous fibres. Each cardiac valve has specific anatomical morphology and histological features. Cardiac valves are divided into atrioventricular and semilunar valves. The atrioventricular valves are the tricuspid and mitral valves that separate the atria from the ventricles. The pulmonary and aortic valves are semilunar valves which separate the ventricles from the large arteries. The atrioventricular valves function to enable blood to flow into the ventricles without reverse flow to the atria during the cardiac cycle. The semilunar valves function to prevent blood flow back into the ventricles from the major arteries [16181920].
Go to :
Tricuspid Valve
Tricuspid valve is located between the right atrium and the right ventricle and it is comprised of three leaflets, the anterior, posterior, and septal leaflets, and also the chordae tendinae, the annulus, and the papillary muscles [161821]. In the tricuspid valve, it is more difficult to define the separate leaflets [1618]. The leaflets are asymmetrical shape, attaching to the chordae tendinae at the ventricle and anchored at the annulus [22]. The anterior leaflet extends from the annulus downwards to the inferolateral wall of the ventricle. The posterior leaflet is the smallest leaflet and it is attached to the posteroinferior wall of the right ventricle. Finally, the septal leaflet is attached to the interventricular septum. There is a thin, translucent area which is located at the inferior region of the valve. This area is attached to the chordate tendinae and by them to the papillary muscles [2324]. The dimensions of each leaflet are different. Generally, the anterior leaflet is the largest one and the shape is quadrangular. The septal and posterior leaflets are semicircular shaped but their shape may vary [25]. However, the posterior leaflet has many clefts or indentations at the free edge, presenting as scallops and there are many variations in the number of scallops [24]. The papillary muscles of the tricuspid valve usually have three main muscles, anterior, septal and posterior papillary muscles [26]. The anterior papillary muscle attaches to the anterior wall of the right ventricle and the chordae tendinae insert to the posterior and anterior leaflets. The posterior muscle attaches to the posterior wall of the right ventricle and the chordae tendinae insert to the septal and posterior leaflets. The septal papillary muscle attaches to the interventricular septum and the chordae tendinae insert to the septal and anterior leaflets [2326]. The function of papillary muscles is early contraction to tighten the chordae tendinae before contraction of the right ventricle and to pull the leaflets when the cardiac muscle in the ventricular wall begins contraction [27].
Go to :
Mitral Valve
The mitral valve separates the left atrium and the left ventricle and the important structures of this valve are the leaflets, annulus, chordae tendinae and papillary muscles. There are usually two leaflets making up the mitral valve, termed the anterior and posterior leaflets. The anterior leaflet has a triangular or semicircular shape and the leaflet base is attached to the annulus. Another side of leaflet is attached to the chordae tendinae and the apex of the leaflet is known as the free edge [2829]. The anterior leaflet is larger than the posterior leaflet. However, interestingly, the posterior leaflet is attached to about two-thirds of circumference of valve [28]. The posterior leaflet is rectangular in shaped and is often divided into three scallops which are defined as the medial, lateral, and middle scallops. Generally, the valve leaflets are thin, soft and translucent. The papillary muscles consist of the anterolateral and posteromedial papillary muscles [30]. The annulus of the mitral valve is similar to the tricuspid valve in that it is formed by the proximal part of the leaflets [31]. The mitral valve is a structure which has been related to various diseases so the studies about its general morphology and geometry are of great importance for clinical applications.
Go to :
Pulmonary Valve
The location of the pulmonary valve is between the pulmonary artery and right ventricle. This valve connects with the infundibulum at the distal part of the right ventricular outflow tract. The main function of the pulmonary valve is preventing reverse blood flow into the right ventricle during diastole. The pulmonary valve is composed of three flexible leaflets, the anterior, right, and left leaflets which form pocket-like cusp shapes, the sinus of valsava, the annulus, the commissure, and the sinotubular junction. In each leaflet, there is a nodule of Arantii located on the middle part of the free leaflet edge. The pulmonary leaflets consist of the hinge, the belly, the coapting area, and launula with the nodule of Arantii. The hinge is the area which attaches to the pulmonary valve annulus and the belly region is located at the center of valve [23]. The anterior leaflet is attached to the anterior wall of the pulmonary trunk and the left leaflet inserts into the anterior part of the interventricular septum. The right leaflet is attached to the right part of the pulmonary wall [32]. Each leaflet has a sinus of valsava which is formed by the annulus, the leaflet commissure, and the sinutubular junction. The sinotubular junction is defined by the line at the upper part of the sinuses that is along the three commissures. The pulmonary valve annulus is crown-shaped, and it is defined as the attachment line of the leaflet to the sinus wall [33].
Go to :
Aortic Valve
The aortic valve separates the left ventricle from the aorta and it is located within the aortic root. The functions are prevention of the return of blood into the left ventricle hence maintaining the coronary perfusion [1617]. The boundaries of the aortic root extend from the lowest attachment of the aortic leaflets to the upper part of the leaflet attachment at the sinotubular junction. In general, the aortic valve consists of the three leaflets, the sinus of valsava, the annulus, an interleaflet triangle, the sinutubular junction, and the commissures that are all similar in structure and function to the pulmonary valve. Three aortic leaflets include the right coronary, left coronary, and noncoronary leaflets, named according to the relationship of the opening of coronary arteries at the sinus wall [18]. The aortic leaflets are composed of the lannula with a nodule (noduli of Arantii), the hinge, the belly, and the coapting area. The lannula is the crescent-shaped part and its margin connects to the coaptation area where each leaflet meets together to close the valve orifice. The hinge area is where the leaflets attach to the walls of the sinuses and the main area of the leaflet is the belly. The belly region is an almost transparent area which is located at the centre of the leaflet [18]. The upper part of the annulus is the commissure, where two leaflets meet. The commissure area is located above the interleaflet triangle. There are two opening orifices of coronary arteries at the walls of the sinuses. Previous studies have revealed that in most cases there are coronary ostia within the sinus wall [34]. The sinotubular junction is defined as the line of transition between the aortic root and the aorta.
Go to :
Heart Valves Morphometry Change with Age
Age is a factor which has major impact on the general morphology of the macro and microstructures of heart valves. Analysis and understanding of the relationship of the morphology and geometry of normal heart valves to age changes is essential for the surgeon and pathologist when treating cardiac conditions. Many past studies describe how morphology of human heart valves changes with age in different ways. Silver and Roberts (1985) [7] studied the detailed anatomy of the normal aortic valve in 100 human hearts. The aortic leaflet area and aortic area at the sinotubular junction were measured using a planimeter. The results showed the total areas of the three leaflets and the luminal area of sinotubular junction were all increased with age. The results of similar measurements taken from the aortic leaflets showed that in all three aortic leaflets about 16% of cases were of similar size; in 51% of cases it was found one leaflet was of a different size from the others, and in 33% of cases all three leaflets were different sizes. This indicated that the leaflets of the aortic valve are often of different sizes within the same person. Scholz et al. (1988) [8] studied age changes within the normal human heart from formalin-fixed cadavers where the age was between birth and 19 years. The circumferences of all four heart valves were measured using a flexible plastic ruler. The results found that there was a correlation between valve circumferences and age in all four heart valves in both sexes. The circumference of the valves were increased with increasing age and the tricuspid valve circumference was larger than the mitral valve; however, in contrast, in the aortic and the pulmonary valves the circumferences were similar. Other studies reported that valve dimensions were similar between autopsy and echocardiograph studies [35363738]. Another study by Kitzman et al. (1988) [9], also studied age changes from the normal human heart using cadavers in which the age range was between 20 and 99 years. The mean circumferences of the tricuspid and mitral valves increased between 30 and 70 years of life and then slightly decreased in women. In men, the mean valve circumferences of atrioventricular valves, the mitral and tricuspid valves were constant throughout life. With regard to semilunar valves, the mean valve circumferences increased progressively with age in both sexes. Since the studies into pediatric and adolescent age groups and human heart valves are few, the developments of heart valve structures and their properties from young to old individuals is unknown. Hence, van Geemen et al. (2016) [10] were interested in the structure of cryopreserved human pulmonary and aortic valves from different age groups (fetus, child, adolescent, and adult). A total of 32 specimens of aortic and pulmonary valves were examined to collect data pertinent to morphometric parameters. Valve annulus diameter, leaflet size in circumferential and radial direction, and leaflet thickness were quantified. The results showed that the diameter of the annulus increased with advancing age in both pulmonary and aortic valves. The annulus in the pulmonary valve was slightly larger than that in the aortic valve. In addition, the leaflet size of these two valves was significantly increased with age in both directions. In aortic cusps, the thicknesses were greater than those in the pulmonary leaflets particularly on the belly region of adolescent and adult groups. These data suggested that the thickness of commissural and belly regions showed no correlation with age. The summary of morphological changes with age are demonstrated in Table 1 This review provides the drawing of the heart valves showing the morphometric parameters in Figs. 1, 2, 3, 4.

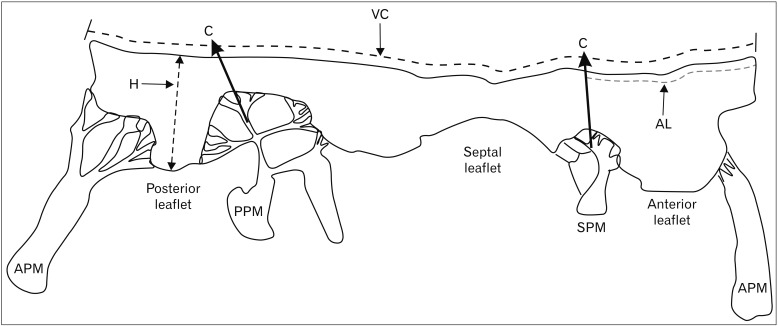 | Fig. 1Drawing of the tricuspid valve showing the morphometric measurements of valve circumference (VC), maximum height of leaflet (H), and attachment length of each leaflet (AL). APM, anterior papillary muscle; C, commissure; PPM, posterior papillary muscle; SPM, septal papillary muscle.
|
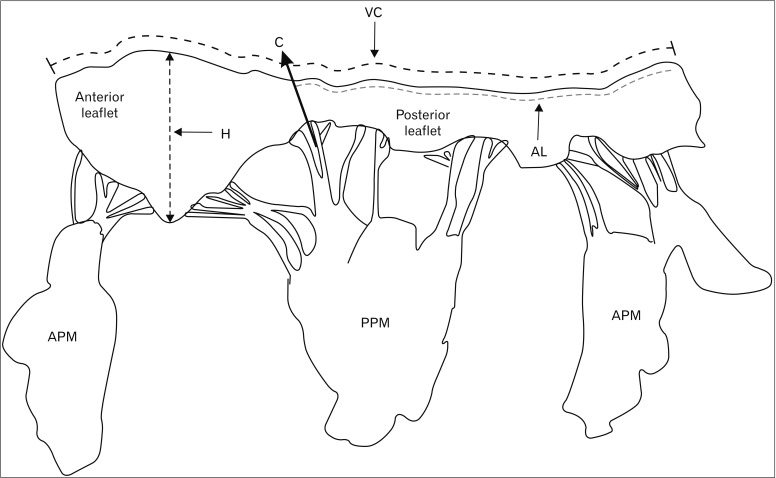 | Fig. 2Drawing of the mitral valve showing the morphometric measurements of valve circumference (VC), maximum height of leaflet (H), and attachment length of each leaflet (AL). APM, anterior papillary muscle; C, commissure; PPM, posterior papillary muscle.
|
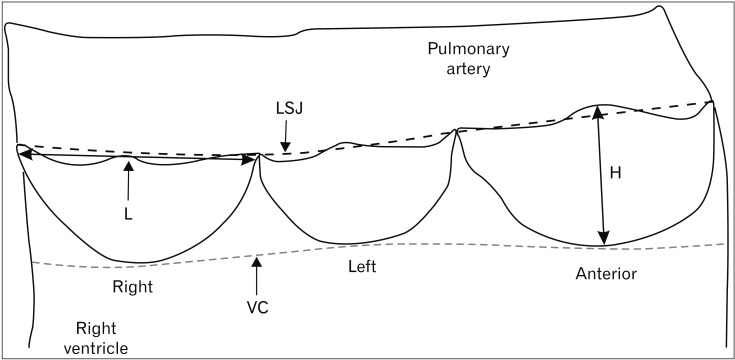 | Fig. 3Drawing of the pulmonary valve showing the morphometric measurements of valve circumference (VC), maximum height of leaflet (H), length of leaflet (L), and length at sinotubular junction (LSJ).
|
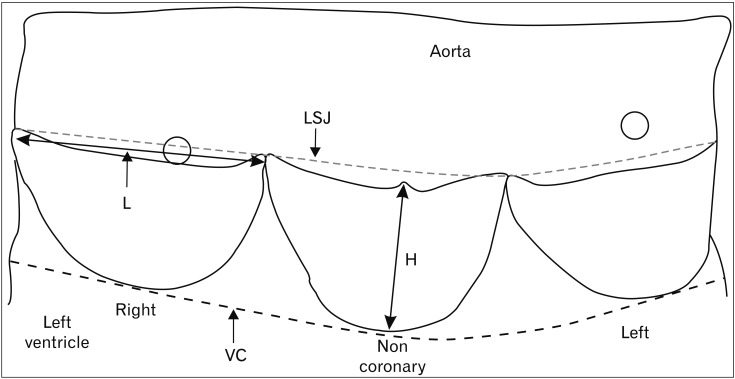 | Fig. 4Drawing of the aortic valve showing the morphometric measurements of valve circumference (VC), maximum height of leaflet (H), length of leaflet (L), and length at sinotubular junction (LSJ).
|
Table 1
Summary of age-related changes of the heart valves morphology
| Study | Age range (yrs) and number of specimen | Structure | Result |
|---|---|---|---|
| Silver and Roberts (1985) [7] | 18–100 (n=100) | Aortic valve | Total area of 3 aortic leaflets and luminal area of sinutubular junction increased with age. |
| Scholz et al. (1988) [8] | Birth–19 (n=200) | Tricuspid, mitral, pulmonary, aortic valves | The valve circumferences increased with age. |
| Kitzman et al. (1988) [9] | 20–99 (n=765) | Tricuspid, mitral, pulmonary, aortic valves | The valve circumferences increased with age. |
| Van Geemen et al. (2016) [10] | 0–53 (n=32) | Pulmonary and aortic valves | Annulus diameter, leaflet size in circumferential and |
![]()
Go to :
Diseases Affecting Heart Valves
Heart valve diseases are an important clinical problem that leads to a high rate of mortality in the global population. More than 100 million people suffer from valve diseases and aortic valve disease are the most common cause of death [3940]. Heart valve replacement is the most common surgical treatment option for valve diseases because a large number of abnormalities associated with heart valves cannot be repaired. Pathology of the valve diseases is associated with the correlation between disruption to structure and function by various factors for example immune, genetic, and inflammatory responses [6]. In low- and middle-income countries, rheumatic heart disease and endocarditis (infective conditions of the valve) are important problems that cause a high rate of mortality and exacerbate the need for valve replacement [41].
Go to :
Rheumatic Valve Disease
Disease of rheumatic valve results from the immunologic complications of rheumatic fever. Rheumatic fever is an immunologically mediated condition from the antibodies released in an immune response against the bacterium group A streptococcus. The inflammatory reaction associated with rheumatic fever involves various structures including the heart, joints, skin, and brain [642]. Rheumatic fever may develop into chronic fibrotic valvular disease which is called rheumatic heart disease and it occurs approximately 20 days after infection (in 40%–50% in patients) [43]. Progression of rheumatic heart disease can cause damage to the heart valves and lead to permanent valve dysfunction later. About 20% of first attacks of rheumatic fever occur in the middle to older age group the highest frequency of the disease usually occurring in children (5–15 years) [44]. The gross characteristic pathology of rheumatic heart disease that affects heart valves is as follows: small vegetations occur at the leaflet at the line of closure region, shortening of the leaflet, thickening of the leaflet, and the commissure fuse, the fusion being caused by fibrous tissue [45].
Go to :
Endocarditis
Endocarditis caused by a bacterial infection of the heart valve resulting in microorganism incorporation and an inflammatory reaction of endothelial cells at the endocardial surface. The bacteria will enter the blood stream and pervade the inner lining of the heart, the heart valves, and blood vessels causing damage to these structures. Patients with infective endocarditis are still suffering today and the rate of mortality is approximately 40%. The infection of normal valve structures can cause valve regurgitation, perivalvular abscesses, and growth of vegetation. So, the treatment of this disease differs from other heart valve diseases [46]. Macroscopic features of endocarditis on the heart valves are vegetation on the leaflet, and calcification. The complications of infection endocarditis can lead to severe heart valve dysfunction, congestive heart failure, and death [43]. The summary of diseases affecting of the heart valves are demonstrated in Table 2.

Table 2
Diseases affecting of the heart valves
![]()
Go to :
Treatment of Heart Valves Dysfunction
Treatment of valvular heart disease depends on the severity of the condition. There is no current clear report that medical treatment can reduce the progression of valvular diseases [47]. Common interventions for treatment of valve diseases are heart valve repair and replacement. Valve repair is usually performed in the case of mitral valve diseases such as prolapsed of the mitral valve, and primary mitral regurgitation. As regards valve regurgitation, it can be repaired by resection of the damaged or prolapsed leaflet [48]. Valve replacement is the most common treatment for valve dysfunction especially in case of severe valve diseases. There are two types of prosthetic heart valves, tissue and mechanical. Tissue valves or bioprosthetic valves are harvested from tissue of animals such as pig (porcine valve) and cow (bovine valve) [17]. Tissue valves are more suitable for sedentary older patients than those of a younger age [49]. Infants and children are usually treated with heart valve replacement because the size of valve is very small [50]. In addition, there are cadaveric allograft and autograft valves [51]. Mechanical valves are made from pyrolytic carbon coated metal which can be used for many years and this valve is more durable than the tissue valve. However, there are drawbacks to each prosthetic valve. Bioprostatic and allograft valves are often susceptible to structural degeneration and calcification and mechanical valves tend be associated with inflammation, infection, and thrombosis, so when this valve is used the patient needs anticoagulant drugs to reduce the risk of thromboembolism [525354]. In addition to these valves heart valve tissue engineering is a new alternative treatment for valvular diseases which has many advantages as the valves can be grown, adapted or remodeled after implantation. The tissue engineered valve is more beneficial for children as the younger patients will grow overtime [1054].
Go to :
Future Direction
Age changes associated with heart valves can be investigated using gross morphometric features and changing in microstructural compositions. Other methods as computed tomography scan or magnetic resonance imaging usually use to study the valve diseases for diagnosis or disease assessment in patients and theses methods may not clear investigation the detailed morphology of the valve. Moreover, echocardiography method can be applied to determine some dimension of the valve as orifice area, circumference and diameter. Studies in gross morphology and histological changes can provide more distinct appearances changes in the heart valves. Analytical studies of the association of heart valves with aging are useful to give basic information of the human valve and can be applied to age estimation in forensic medicine. However, there are no studies on the age-associated changes of the heart valve in the Thai population. But, there are few reports about the valve morphology in Asians (Indians, SriLankan) [555657]. Among the differences between race, it was found that the valve dimensions in Asians were smaller than Caucasians and Africans especially in valve circumference because of racial differences in body mass index and stature [2957]. The shape of the valves is similar between the difference population. Thus, we aim to study the relationship between gross macroscopic features and age of normal human heart valves in a Thai population in future studies. In gross morphometry, the measurement parameters of the tricuspid and mitral valves include valve circumference, diameter, the attachment length, the height, area of leaflet, and total area of the valve. The measurement parameters of the pulmonary and aortic valves are similar to those atrioventricular valves except the circumference at the sinotubular junction. These parameters are measured using image analysis software. We plan to investigate the correlation between age and parameters of the valves and investigate if they are applicable for further age estimation in forensic science. One of the benefits of the study would be that it will form a new database for cardiac valves in Thai population and help in the treatment of valvular diseases. It would also benefit Cardiologists and Cardiothoracic surgeons in future.
Go to :
Conclusion
In the cardiovascular system, the cardiac valves are some of the structures which change with advancing age. The human heart valves are complex anatomical structures consisting of leaflets and many supporting structures. With advancing age, these changes can be both macroscopic and microscopic in appearances. As regards gross morphometry, valve thickness, circumference, luminal area at sinotubular junction, diameter, orifice area, and leaflet size show a correlation with increasing age especially in the case of the aortic valve. Investigation about the detailed morphometric features of the heart valves and the relationship between these parameters and age will be essential for optimal treatment of valvular diseases and may be applicable for age estimation in forensic science.
Go to :
 XML Download
XML Download