

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Using computed tomography (CT) and magnetic resonance imaging (MRI) in diagnosis and staging a tumor in the neck has become a daily medicine, and the dependence on the radiological modalities in managing patients has been only increasing. Therefore, it is essential for physicians to familiarize themselves with any variations of the neck muscles to avoid misinterpretations of the radiological images and make right treatment plans for their patients.
The digastric muscle is an important muscle in the neck, which pulls the mandible downward to open the jaw and elevates the hyoid bone for stabilization during swallowing, and it is also involved in chewing and speech [1]. The digastric muscle is also characterized to have many variations that do not necessarily produce clinical symptoms, yet recognizing its variations would help physicians to make better evaluations and treatment plans for their patients. Also, surgeons can avoid unnecessary surgeries in the neck by recognizing the variations of the digastric muscle which can be misinterpreted as metastasized lymph nodes or tumor masses [2].
With the improved plastic surgical technology and higher demand for aesthetics, the digastric muscle plays an important role in the facial reconstructive surgeries. The digastric muscle can be used as a part of the flap [3], or it can be used to lower the lip for more natural facial expressions for the patients with the facial nerve injury [4].
The aim of this study is to review the anatomy, embryology, morphological variations and growing clinical significance of the digastric muscle.
Go to : 
Historical Background
According to Yamada [5], the digastric muscle and its variations were documented by Winslow and Albinus in the 18th century, Lobegrove, Macalister, Dobson, His, Bianchi, Gegenbauer, and Bovero in the 19th century, and Toldt, Bijvoet, Stracker, Eisler, Bertelli, and Zlabek in the early 20th century.
Stracker [6] and Zlabek [7] studied the variations of the digastric muscle on 305 and 101 cadavers respectively. Yamada [5] studied the variations of the digastric muscle on 100 fetal cadavers and 50 adult cadavers. Later on, Mori [8] investigated the musculature including the digastric muscle of 262 Japanese cadavers. Since the 18th century, our knowledge on the digastric muscle has been expanding through the tremendous works done by the dedicated anatomists, scientists and physicians.
Also, Zlabek, Yamada [5], Mori [8], and De-Ary-Pires et al. [9] made their own classification system to categorize the variations of the digastric muscle according to morphology. Although there is no consensus on what classification needs to be used for categorizing the digastric muscle variations, each classification system helped anatomists and physicians understand the overall morphology of the digastric muscle better.
Even though many of physiological, anatomical and radiological characteristics about the digastric muscle have been discovered, today there is still much more to be learnt about this muscle.
Go to :
Anatomy
There is a pair of digastric muscles in the neck, and each digastric muscle has the anterior belly and the posterior belly. The anterior belly is attached to the digastric fossa on the base of the mandible close to the midline and runs toward the hyoid bone. The posterior belly is attached to the notch of the mastoid process of the temporal bone and also runs toward the hyoid bone [10]. The two bellies meet as the intermediate tendon, which penetrates the stylohyoid muscle and also passes through the fibrous loop which is attached to the body and greater cornu of the hyoid bone [1011]. However, as the study of Kim et al. [12] showed, the intermediate tendon does not have to penetrate the stylohyoid muscle. The intermediate tendon can lie medial or lateral to the stylohyoid muscle instead of penetrating it.
An important surgical landmark can be described by the digastric muscle. The submandibular triangle is a triangular area on each side demarcated by the mandible superiorly, the anterior belly of the digastric muscle medially and the posterior belly of the digastric muscle laterally. Each submandibular triangle contains the submandibular gland, submandibular lymph nodes, hypoglossal nerve, facial artery and facial vein [1113].
The submental triangle is a single triangular area created by both anterior bellies of the digastric muscle and the hyoid bone inferiorly, and it contains the submental lymph nodes and anterior jugular vein [13]. The carotid triangle is a triangular area on each side demarcated by the posterior belly of the digastric muscle superiorly, superior belly of the omohyoid muscle medially and sternocleidomastoid muscle laterally. The carotid triangle contains the common carotid artery, internal and external carotid arteries, internal jugular vein, deep cervical lymph nodes, vagus nerve, accessory nerve, and hypoglossal nerve [11].
Go to :
Nerve Innervation
The mylohyoid nerve of the inferior alveolar nerve of the mandibular nerve of the trigeminal nerve innervates the anterior belly of the digastric muscle, and the facial nerve innervates the posterior belly of the digastric muscle [10]. However, there are some reported cases that the anterior belly of the digastric muscle was innervated by the branches of the facial nerve in addition to the mylohyoid nerve [1415]. Furthermore, Kawai et al. [15] observed that when the branches of the facial nerve innervate the anterior belly of the digastric muscle, they seemed to be specifically the branches of the stylohyoid nerve.
It should be pointed out that the anterior belly of the digastric muscle and the mandibular nerve of the trigeminal nerve are derived from the first pharyngeal arch, and the posterior belly of the digastric muscle and the facial nerve are derived from the second pharyngeal arch [16].
Go to :
Arterial Supply
The anterior belly of the digastric muscle receives its arterial supply mainly from the submental artery of the facial artery, and the posterior belly of the digastric muscle receives its arterial supply from the posterior auricular and occipital arteries [16]. The submental artery, whose origin is about 1.5 mm in diameter, is the largest cervical branch of the facial artery and runs between the mylohyoid muscle and submandibular gland [17]. Faltaous and Yetman [3] studied 24 cadavers and reported that the submental artery runs deep to the anterior belly of the digastric muscle in 70% of cases and runs superficial to the anterior belly of the digastric muscle in 30% of cases. The posterior auricular artery arises posteriorly from the external carotid artery right above the posterior belly of the digastric muscle and the occipital artery arises posteriorly from the external carotid artery below the posterior auricular artery and crosses with the hypoglossal nerve [1011].
Go to :
Embryology
The prenatal life consists of the embryonic period and the fetal period. The embryonic period is the first eight postfertilizational weeks, and the fetal period begins at the 9th postfertilizational week and lasts until the birth. The embryonic period can be divided into 23 stages, which are known as the Carnegie stages [18]. During the stages 10 to 13, the five pairs of the pharyngeal arches are formed as the population of the neural crest cells migrate more caudally from the embryonic pharynx which is the most cranial portion of the foregut [16].
The anterior belly of the digastric muscle, mylohyoid muscle, tensor tympani muscle, tensor veli palatine muscle, muscles of mastication (the temporalis muscle, masseter muscle and lateral and medial pterygoid muscles), genial tubercle of the mandible and mandibular nerve of the trigeminal nerve are derived from the first pharyngeal arch which is also called the mandibular arch and first seen at the stage 10 (28 to 30 days). The posterior belly of the digastric muscle, stapedius muscle, buccinator muscle, auricular muscles, occipitofrontalis muscle, facial muscles, platysma muscle, stylohyoid muscle, stylohyoid ligament, lesser horn and upper part of the body of the hyoid bone and facial nerve are derived from the second pharyngeal arch which is also called the hyoid arch and first seen at the stage 11 (28 to 30 days). The stylopharyngeus muscle, greater horn and lower part of the body of the hyoid bone and glossopharyngeal nerve are derived from the third pharyngeal arch which is first seen at the stage 12 (29 to 31 days). The cricothyroid muscle, inferior pharyngeal constrictor muscle, levator veli palatini muscle, thyroid cartilage and pharyngeal branch of the vagus nerve are derived from the fourth pharyngeal arch which is first seen at the stage 13 (30 to 33 days) [16].
Since both the digastric muscle and mylohyoid muscle develop from the first pharyngeal arch, their anomalies are often found simultaneously [19].
Go to :
Morphological Variations
Larsson and Lufkin [2] described a case of unilateral anterior accessory belly originating from the left digastric fossa and joining the right anterior belly and a case of unilateral variation of the left anterior belly originating from the mylohyoid muscle and inserting into the ipsilateral side of the hyoid bone. Sargon and Celik [19] described a case of right unilateral anterior accessory belly originating from the digastric fossa and inserting into the middle of the hyoid bone. Sarikcioglu et al. [20] reported a case of bilateral anterior accessory muscle inserting into the myohyoid raphe, one small accessory muscle originated from the raphe and inserted into the left intermediate tendon, and one small fibrous band originated from the raphe and inserted into the right intermediate tendon. Holibková and Machálek [21] reported a case of bilateral anterior accessory belly originating from digastric fossa and inserting into the ipsilateral intermediate tendon, and a case of two left accessory bellies originating from the digastric fossa and inserting into the ipsilateral and contralateral intermediate tendon.
Sargon et al. [22] described a case of two anterior accessory bellies (right and left) crossing each other and inserting into the intermediate tendon of the other side with one small accessory muscle originating from around the middle of the left anterior belly and inserting into the right intermediate tendon, and a case of one right accessory belly bifurcating into the right and left ones that inserted into the intermediate tendon with two left accessory bellies originating from the digastric fossa inserting into the left arm of the right anterior accessory belly. Also, Sargon et al. [22] described a case of one accessory belly from the middle digastric fossa, bifurcating into the right arm joining the right anterior belly and the left arm joining the left anterior belly, and a case of one right accessory belly originating from the digastric fossa, bifurcating into the right arm joining the right anterior belly and the left arm joining the left anterior accessory belly with one left accessory belly originating the digastric fossa joining the left anterior belly, and a case of the right anterior belly originated from the mylohyoid muscle and hyoid bone. This abnormal belly fused with the posterior belly of the digastric muscle by an intermediate tendon with no presence of the left anterior belly of the digastric muscle.
Peker et al. [23] reported a case of bilateral anterior accessory muscle with left one originated from the mylohyoid raphe and inserting into the left intermediate tendon and right one originating from the myohyoid raphe and inserting into the right intermediate tendon. Guelfguat et al. [24] described a case of right unilateral accessory belly originating from the digastric fossa and inserting into the middle of the hyoid bone. Yüksel and Yüksel [25] reported a case of bilateral anterior accessory bellies originating from the mylohyoid raphe and inserting into the ipsilateral intermediate tendon. Celik et al. [26] reported a case of left unilateral anterior belly variation with four anterior bellies originating from the digastric fossa and inserting into the middle of the hyoid bone. Aktekin et al. [27] reported a case of bilateral accessory muscle crossing each other very nicely and inserts into the other side.
Fujimura et al. [28] reported a case of a variation in which one left anterior accessory muscle originated from the digastric fossa and joined the left anterior belly. The mylohyoid raphe was moved significantly to the right side, and it was the origin for five right anterior accessory muscles spreading multiple directions without having a normal right anterior belly. Turan-Ozdemir et al. [29] reported a case of one middle anterior accessory belly originating from the middle digastric fossa inserting into the right intermediate tendon. Another anterior accessory belly originated from the mylohyoid muscle and inserted into the left intermediate tendon. Almost it looks like the middle accessory muscle bifurcated into the right and left.
Loukas et al. [30] reported a case of bilateral occurrence of an accessory head of the anterior digastric muscle which arose from the digastric fossa and inserted upon the midline raphe (on the right) and on the mylohyoid muscle. The left accessory anterior digastric muscle took its origin from a separate tendon medial to the main belly of the anterior digastric muscle and proceeded posteromedially to insert upon the midline raphe of the mylohyoid muscle. The right accessory anterior digastric muscle immediately bifurcated into two medial and lateral heads. The lateral head rejoined with the main belly of the anterior digastric muscle, while the medial head continued to insert upon the midline raphe of the mylohyoid muscle. The nerve supply was identified bilaterally and the nerve to the mylohyoid was responsible for innervating both the normal and accessary anterior belly of the digastric muscle.
Ozgursoy and Kucuk [31] described a case of left posterior accessory muscle which originated from the left mastoid process and inserted into the strap muscle (probably superior belly of omohyoid muscle or sternohyoid muscle) near the thyroid cartilage. Bakirci et al. [32] reported a case of bilateral anterior accessory bellies originating from the digastric fossa and inserting into the ipsilateral intermediate tendon, and the left side had an accessory anterior belly of the digastric muscle with an accessory muscle (i.e., transverse one that connects the right and left anterior bellies) bundle lying transversally between the two anterior bellies. Ozgur et al. [33] reported a case of three accessory anterior bellies originating from the digastric fossa and inserting into the ipsilateral intermediate tendon without crossing, and a pair of accessory muscles originating from the midline raphe and inserting into the ipsilateral side.
Reyes et al. [34] described a case of bilateral anterior accessory bellies originating from the mylohyoid raphe and inserting into the ipsilateral intermediate tendon. Mehta et al. [35] reported a case of unique variation of posterior belly of the digastric muscle with bilateral bipartite origin of the posterior belly. The bipartite origins joined to form a single posterior belly on each side. Kyung et al. [36] reported a case of three accessory anterior bellies: Two accessory bellies on each side ran ipsilaterally and attached at the mylohyoid raphe of the mylohyoid muscle, and the third accessory belly originated from the right intermediate tendon, ran horizontally, and attached at the mylohyoid raphe where two other accessory bellies inserted.
Yamazaki et al. [37] reported a case of four accessory anterior bellies. First one is a thin accessory anterior belly originating from the right digastric fossa inserting into the second anterior accessory belly. Second one is a right accessory anterior belly originating from the mylohyoid raphe and inserting into the right intermediate tendon. Third one is a left accessory anterior belly originating from the mylohyoid raphe and inserting into the left intermediate tendon. Fourth one is a transverse accessory anterior belly connecting from the left intermediate tendon to the right intermediate tendon. Quadros et al. [38] described a case of left unilateral accessory muscle of the anterior belly which originated from digastric fossa and inserted next to the left anterior belly of digastric muscle. Rani et al. [39] described a case of bilateral accessory muscle, medially located, noncrossing, and inserting into the hyoid bone.
There are numerous morphological variations of the digastric muscle described in the literature and nearly all of the variations are the variations of the anterior belly of the digastric muscle. In this section the variations of the digastric muscle are analyzed based on the male and female ratio, modality of the study, ethnicity and presentation type. Also, some of common variations are presented with figures. It is important for physicians to familiarize themselves with the variations of the digastric muscle to recognize them in the clinical setting.
Based on 10 cadaveric studies where the variations of the digastric muscle are noted for male and female, the variations of the digastric muscle are found in 35.5% of male cadavers and 33.4% of female cadavers (Table 1) [569224041424344].
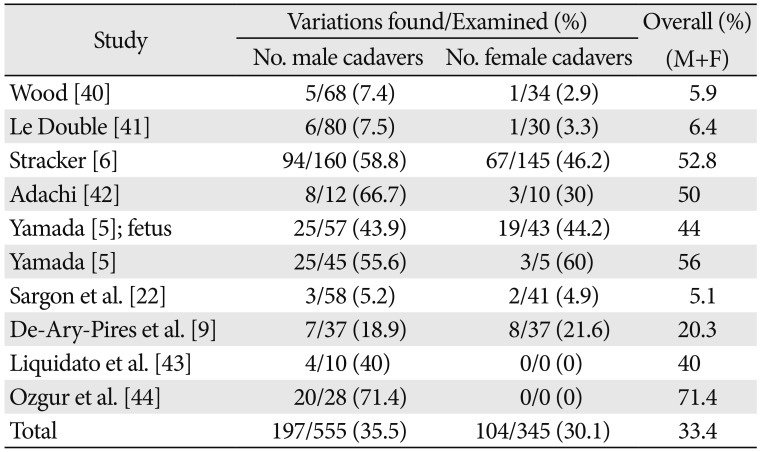
Table 1
The cadaveric prevalence rate of the digastric muscle variations for males and females
| Study | Variations found/Examined (%) | Overall (%) (M+F) | |
|---|---|---|---|
| No. male cadavers | No. female cadavers | ||
| Wood [40] | 5/68 (7.4) | 1/34 (2.9) | 5.9 |
| Le Double [41] | 6/80 (7.5) | 1/30 (3.3) | 6.4 |
| Stracker [6] | 94/160 (58.8) | 67/145 (46.2) | 52.8 |
| Adachi [42] | 8/12 (66.7) | 3/10 (30) | 50 |
| Yamada [5]; fetus | 25/57 (43.9) | 19/43 (44.2) | 44 |
| Yamada [5] | 25/45 (55.6) | 3/5 (60) | 56 |
| Sargon et al. [22] | 3/58 (5.2) | 2/41 (4.9) | 5.1 |
| De-Ary-Pires et al. [9] | 7/37 (18.9) | 8/37 (21.6) | 20.3 |
| Liquidato et al. [43] | 4/10 (40) | 0/0 (0) | 40 |
| Ozgur et al. [44] | 20/28 (71.4) | 0/0 (0) | 71.4 |
| Total | 197/555 (35.5) | 104/345 (30.1) | 33.4 |
![]()
CT and MRI studies were done on 110 adults by Muraki et al. [45] and Larsson and Lufkin [2] (Table 2). On the CT study of 35 adults, Muraki et al. [45] noted the anterior belly “asymmetry” on 6 patients and the posterior belly “asymmetry” on 5 patients. Since Muraki et al. [45] did not specify what exactly “asymmetry” meant, there is a possibility that “asymmetry” might indicate a mere size difference of muscles between the left anterior belly and the right anterior belly rather than indicating a true variation. Larsson and Lufkin [2] conducted the CT study of 40 adults and the MRI study of 35 adults, and found one case of a variation in each study (Table 2).
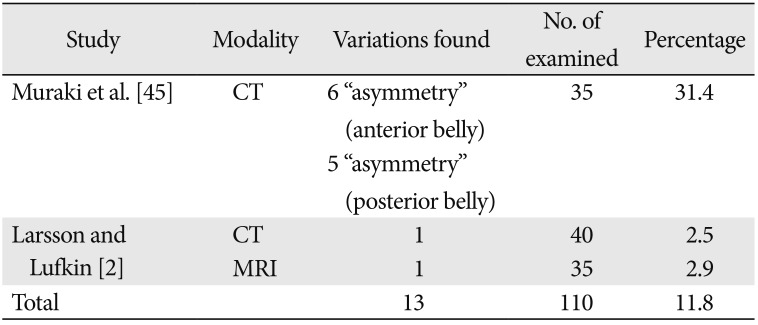
Table 2
The prevalence rate of the digastric muscle variations recognized by CT and MRI in adult population
| Study | Modality | Variations found | No. of examined | Percentage |
|---|---|---|---|---|
| Muraki et al. [45] | CT | 6 “asymmetry” (anterior belly) | 35 | 31.4 |
| 5 “asymmetry” (posterior belly) | ||||
| Larsson and Lufkin [2] | CT | 1 | 40 | 2.5 |
| MRI | 1 | 35 | 2.9 | |
| Total | 13 | 110 | 11.8 |
![]()
Table 3 shows the cadaveric prevalence rate of the variations of the digastric muscle of the Asian population, mostly Japanese population including fetuses. The variations were found in 51.7% of the population.
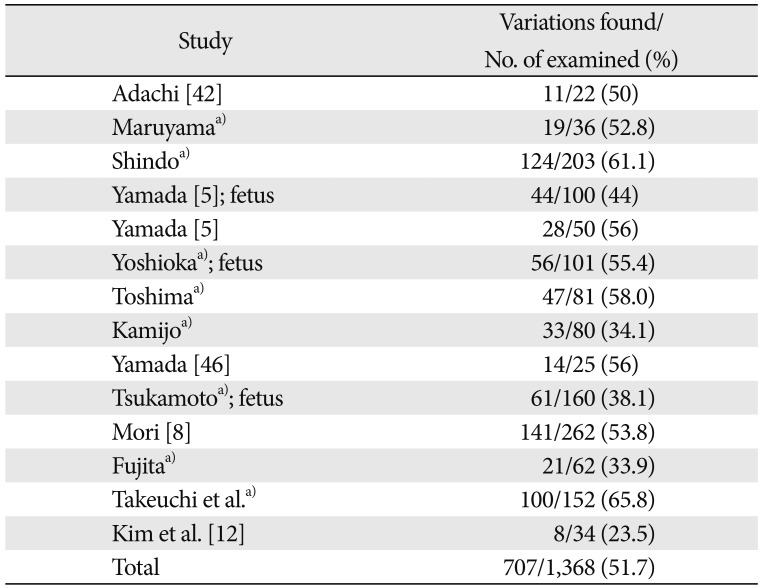
Table 3
The cadaveric prevalence rate of the digastric muscle variations in the Asian population including fetuses
| Study | Variations found/No. of examined (%) |
|---|---|
| Adachi [42] | 11/22 (50) |
| Maruyamaa) | 19/36 (52.8) |
| Shindoa) | 124/203 (61.1) |
| Yamada [5]; fetus | 44/100 (44) |
| Yamada [5] | 28/50 (56) |
| Yoshiokaa); fetus | 56/101 (55.4) |
| Toshimaa) | 47/81 (58.0) |
| Kamijoa) | 33/80 (34.1) |
| Yamada [46] | 14/25 (56) |
| Tsukamotoa); fetus | 61/160 (38.1) |
| Mori [8] | 141/262 (53.8) |
| Fujitaa) | 21/62 (33.9) |
| Takeuchi et al.a) | 100/152 (65.8) |
| Kim et al. [12] | 8/34 (23.5) |
| Total | 707/1,368 (51.7) |
![]()
Table 4 shows the cadaveric prevalence rate of the variations of the digastric muscle in the general population excluding the Asian population. The variations were found in 31.4% of population, which suggests that there is a higher frequency of the variations of the digastric muscle in the Asian population (51.7%).
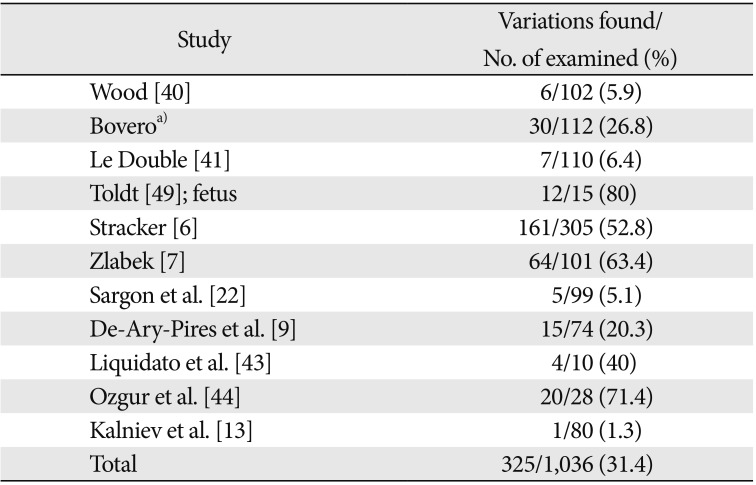
Table 4
The cadaveric prevalence rate of the digastric muscle variations in the general population excluding the Asian population
| Study | Variations found/No. of examined (%) |
|---|---|
| Wood [40] | 6/102 (5.9) |
| Boveroa) | 30/112 (26.8) |
| Le Double [41] | 7/110 (6.4) |
| Toldt [49]; fetus | 12/15 (80) |
| Stracker [6] | 161/305 (52.8) |
| Zlabek [7] | 64/101 (63.4) |
| Sargon et al. [22] | 5/99 (5.1) |
| De-Ary-Pires et al. [9] | 15/74 (20.3) |
| Liquidato et al. [43] | 4/10 (40) |
| Ozgur et al. [44] | 20/28 (71.4) |
| Kalniev et al. [13] | 1/80 (1.3) |
| Total | 325/1,036 (31.4) |
![]()
Table 5 shows the cadaveric studies of the unilateral and bilateral presentations of the variations of the digastric muscle. The left unilateral presentation rate was 20.6% and the right unilateral presentation rate was 20.2%. Overall, the unilateral presentation rate was 46.3% and the bilateral presentation rate was 53.7%.
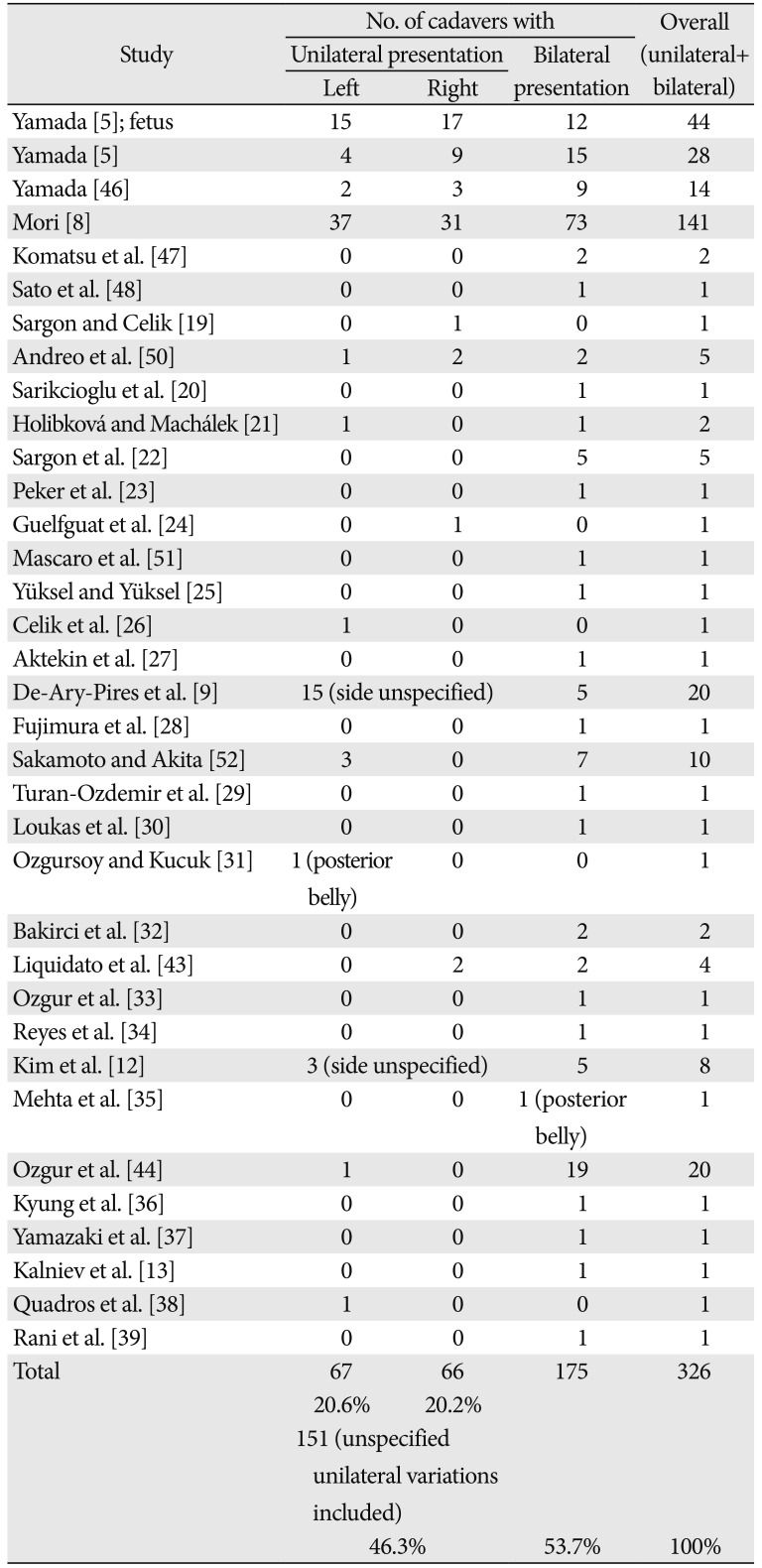
Table 5
The review of the literature on the frequency of unilateral and bilateral cadaveric presentation of the digastric muscle variationsa)
| Study | No. of cadavers with | Overall (unilateral+bilateral) | ||
|---|---|---|---|---|
| Unilateral presentation | Bilateral presentation | |||
| Left | Right | |||
| Yamada [5]; fetus | 15 | 17 | 12 | 44 |
| Yamada [5] | 4 | 9 | 15 | 28 |
| Yamada [46] | 2 | 3 | 9 | 14 |
| Mori [8] | 37 | 31 | 73 | 141 |
| Komatsu et al. [47] | 0 | 0 | 2 | 2 |
| Sato et al. [48] | 0 | 0 | 1 | 1 |
| Sargon and Celik [19] | 0 | 1 | 0 | 1 |
| Andreo et al. [50] | 1 | 2 | 2 | 5 |
| Sarikcioglu et al. [20] | 0 | 0 | 1 | 1 |
| Holibková and Machálek [21] | 1 | 0 | 1 | 2 |
| Sargon et al. [22] | 0 | 0 | 5 | 5 |
| Peker et al. [23] | 0 | 0 | 1 | 1 |
| Guelfguat et al. [24] | 0 | 1 | 0 | 1 |
| Mascaro et al. [51] | 0 | 0 | 1 | 1 |
| Yüksel and Yüksel [25] | 0 | 0 | 1 | 1 |
| Celik et al. [26] | 1 | 0 | 0 | 1 |
| Aktekin et al. [27] | 0 | 0 | 1 | 1 |
| De-Ary-Pires et al. [9] | 15 (side unspecified) | 5 | 20 | |
| Fujimura et al. [28] | 0 | 0 | 1 | 1 |
| Sakamoto and Akita [52] | 3 | 0 | 7 | 10 |
| Turan-Ozdemir et al. [29] | 0 | 0 | 1 | 1 |
| Loukas et al. [30] | 0 | 0 | 1 | 1 |
| Ozgursoy and Kucuk [31] | 1 (posterior belly) | 0 | 0 | 1 |
| Bakirci et al. [32] | 0 | 0 | 2 | 2 |
| Liquidato et al. [43] | 0 | 0 | 2 | 4 |
| Ozgur et al. [33] | 0 | 2 | 1 | 1 |
| Reyes et al. [34] | 0 | 0 | 1 | 1 |
| Kim et al. [12] | 3 (side unspecified) | 5 | 8 | |
| Mehta et al. [35] | 0 | 0 | 1 (posterior belly) | 1 |
| Ozgur et al. [44] | 1 | 0 | 19 | 20 |
| Kyung et al. [36] | 0 | 0 | 1 | 1 |
| Yamazaki et al. [37] | 0 | 0 | 1 | 1 |
| Kalniev et al. [13] | 0 | 0 | 1 | 1 |
| Quadros et al. [38] | 1 | 0 | 0 | 1 |
| Rani et al. [39] | 0 | 0 | 1 | 1 |
| Total | 67 | 66 | 175 | 326 |
| 21% | 20% | |||
| 151 (unspecified unilateral variations included) | ||||
| 46% | 54% | 100% | ||
![]()
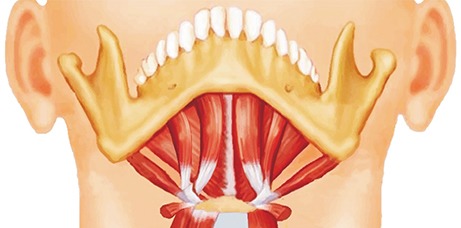
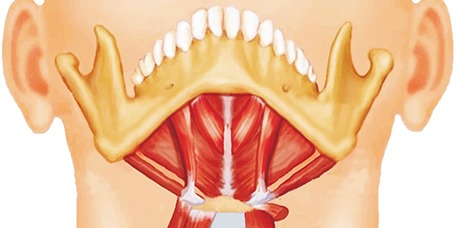
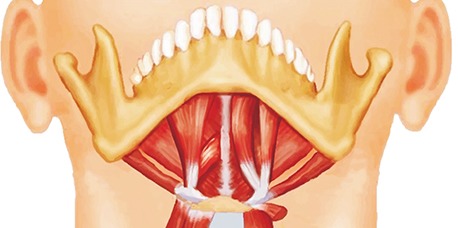
Table 6 presents some of common variations of the digastric muscle. These variations are by no means exhaustive. The figures do not necessarily represent the exact same morphological variations documented in the literature, but they rather serve as templates to help physicians to familiarize themselves with the possible morphological variations of the digastric muscle that they might encounter in the clinical setting.
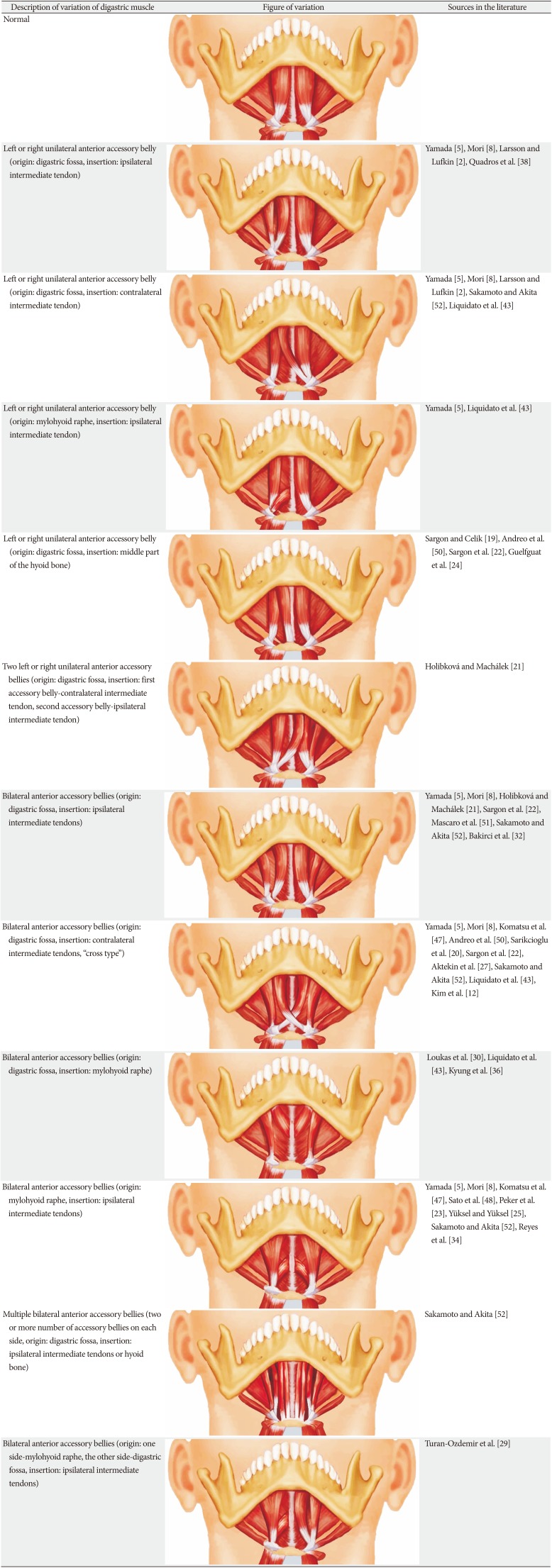
Table 6
Characteristics of common variations of the digastric muscle documented in the literature
| Description of variation of digastric muscle | Figure of variation | Sources in the literature Normal |
|---|---|---|
| Normal |
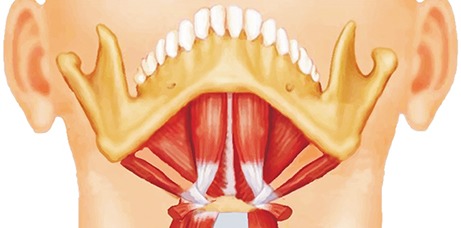
|
|
| Left or right unilateral anterior accessory belly (origin: digastric fossa, insertion: ipsilateral intermediate tendon) |

|
Yamada [5], Mori [8], Larsson and Lufkin [2], Quadros et al. [38] |
| Left or right unilateral anterior accessory belly (origin: digastric fossa, insertion: contralateral intermediate tendon) |
|
Yamada [5], Mori [8], Larsson and Lufkin [2], Sakamoto and Akita [52], Liquidato et al. [43] |
| Left or right unilateral anterior accessory belly (origin: mylohyoid raphe, insertion: ipsilateral intermediate tendon) |

|
Yamada [5], Liquidato et al. [43] |
| Left or right unilateral anterior accessory belly (origin: digastric fossa, insertion: middle part of the hyoid bone) |

|
Sargon and Celik [19], Andreo et al. [50], Sargon et al. [22], Guelfguat et al. [24] |
| Two left or right unilateral anterior accessory bellies (origin: digastric fossa, insertion: first accessory belly-contralateral intermediate tendon, second accessory belly-ipsilateral intermediate tendon) |

|
Holibková and Machálek [21] |
| Bilateral anterior accessory bellies (origin: digastric fossa, insertion: ipsilateral intermediate tendons) |
|
Yamada [5], Mori [8], Holibková and Machálek [21], Sargon et al. [22], Mascaro et al. [51], Sakamoto and Akita [52], Bakirci et al. [32] |
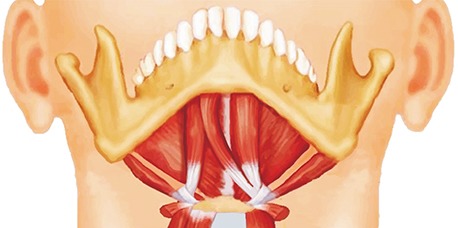
| Bilateral anterior accessory bellies (origin: digastric fossa, insertion: contralateral intermediate tendons, “cross type”) |

|
Yamada [5], Mori [8], Komatsu et al. [47], Andreo et al. [50], Sarikcioglu et al. [20], Sargon et al. [22], Aktekin et al. [27], Sakamoto and Akita [52], Liquidato et al. [43], Kim et al. [12] |
| Bilateral anterior accessory bellies (origin: digastric fossa, insertion: mylohyoid raphe) |
|
Loukas et al. [30], Liquidato et al. [43], Kyung et al. [36] |
| Bilateral anterior accessory bellies (origin: mylohyoid raphe, insertion: ipsilateral intermediate tendons) |

|
Yamada [5], Mori [8], Komatsu et al. [47], Sato et al. [48], Peker et al. [23], Yüksel and Yüksel [25], Sakamoto and Akita [52], Reyes et al. [34] |
| Multiple bilateral anterior accessory bellies (two or more number of accessory bellies on each side, origin: digastric fossa, insertion: ipsilateral intermediate tendons or hyoid bone) |

|
Sakamoto and Akita [52] |
| Bilateral anterior accessory bellies (origin: one side-mylohyoid raphe, the other side-digastric fossa, insertion: ipsilateral intermediate tendons) |
|
Turan-Ozdemir et al. [29] |
![]()
Although the most variations of the digastric muscle are the variations of the anterior belly, the variations of the posterior belly of the digastric muscle are documented in the literature. De-Ary-Pires et al. [9] observed a case of unilateral absence of the posterior belly of the digastric muscle, and Ozgursoy and Kucuk [31] reported a unilateral posterior accessory belly of the digastric muscle. Also, Mehta et al. [35] reported a case of bilateral bipartite origins of the posterior belly of the digastric muscle.
Go to :
Clinical Significance
The protection of the airway during swallowing food is essential and achieved through the laryngeal sphincter closure, laryngeal covering by the epiglottis and larynx elevation anteriorly and superiorly [53]. The elevation of the larynx can be achieved by elevating the hyoid bone from which the laryngeal cartilages are suspended, and the suprahyoid muscles consisting of the geniohyoid muscle, mylohyoid muscle and anterior belly and posterior belly of the digastric muscle are involved in elevating the hyoid bone anteriorly and superiorly [53].
A tumor can cause muscle enlargement and asymmetry, and it can be shown as an increased muscle bulk with the contrast enhancement on CT [2]. An anterior accessory muscle can be seen as a pseudomass on CT, but unlike a tumor, it does not show the abnormal contrast enhancement [2]. Also, a tumor shows higher signal on T2 weighted MRI while a pseudomass does not show the higher signal [2]. However, although the T2 weighted MRI is useful to detect the soft tissue tumors in the neck, it can still fail to detect the tumor [54].
The marginal mandibular branch of the facial nerve innervates muscles that lower the lip such as the depressor anguli oris and depressor labii inferioris muscles [455]. Therefore, an injury of the marginal mandibular branch of the facial nerve can produce an asymmetric smile [4]. When there is complete paralysis of the marginal mandibular branch of the facial nerve, the anterior belly of the digastric muscle, intermediate tendon and small portion of the posterior belly as a whole can be used as a flap. The end of the flap (i.e., the cut part of the posterior belly) is sewn on the lower lip while the anterior belly is being attached to the digastric fossa, then the lip of the patient can be lowered, thereby making the patient smile again [4].
Oral cancer sometimes necessitates the resection of the anterior mandibular arch, and postoperatively the depression of the tongue can cause the stridor, in which case the tracheostomy may be necessary [56]. The depression of the tongue can be prevented by attaching the tongue muscle to the intermediate tendon of the digastric muscle, thereby avoiding the stridor and tracheostomy postoperatively [56].
The submental flap is very useful for the facial reconstruction surgery, and the anterior belly of the digastric muscle should be included in the flap since the submental vessels often course deep to the anterior belly of the digastric muscle [3].
A bulky anterior belly of the digastric muscle can contribute to an unaesthetic neck contour by giving a bulge in the submental area. By removing a good portion of the anterior belly muscle (i.e., making the anterior belly thinner), the bulge in the submental area can be minimized, thereby giving the patient a better neck contour [57].
The posterior belly of the digastric muscle is an anatomical landmark to determine the courses of the accessory nerve, internal jugular vein, carotid arteries and hypoglossal nerve that need to be preserved during most neck dissections [31]. Also, the posterior belly of the digastric muscle is a good landmark to locate the origin of the superior root of ansa cervicalis which is an important nerve for the nerve reconstructive surgery in the neck and usually located right above or at the level of the posterior belly of the digastric muscle [5859].
Go to :
Conclusion
The variations of the digastric muscle have been recorded by the dedicated anatomists and physicians since the 18th century, and their investigations on this muscle have been a great value in diagnosis and making right treatment plans for patients. Although the variations of the digastric muscle do not necessarily produce clinical symptoms, they still play an important role in the clinical setting. Physicians need to know the normal anatomy of the digastric muscle and its variations for the optimal care of their patients.
Go to :
 XML Download
XML Download