

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity has reached epidemic proportions in many parts of the world; in 2018, 39% of adults were overweight and 13% were obese [1]. The Global Burden of Disease Study [2] reported that the prevalence of overweight and obesity in Southeast Asia was 22.1% of men and 28.3% of women, with the highest rates in Malaysia at 48.3% and 48.6% for men and women, respectively. The Malaysian National Health and Morbidity Survey (NHMS) 2015 reported a 30.0% prevalence of overweight among adults, while the prevalence of obesity was 17.7% [3]. The report suggests that the prevalence of overweight was significantly higher among males, whereas the prevalence of obesity was significantly higher among females [3]. In addition, the national prevalence of abdominal obesity (waist circumference measurement cut-off values of > 90 cm for males and > 80 cm for females) was 48.6% with a significantly higher prevalence among females [3].
Obesity was quite rare among earlier human populations (hunter-gatherers) because of their active lifestyles that involve physical activity and occasionally unpredictable diet and food shortages [4]. Their dietary requirements were met by consuming uncultivated plants and hunted animals that were extremely lean and low in fats Simple sugars in the form of honey was rare, and there were no dairy foods because of the lack of domesticated animals [4]. Lifestyle changes occurred with the emergence of agriculture during the Neolithic transition, where the cultivation of plants and domestication of animals produced a surplus of food, such as high-carbohydrate crops, including rice, wheat, barley, and tubers. In addition, humans gave up their nomadic lifestyles because of food production and sufficiency [5]. In today's modern world, however, changes in culture and technology had led to changes in the types of food consumed, reduced the need for physical activity, and increased exposure to harmful agents, such as alcohol and tobacco [4].
Poor dietary habits and inadequate physical activity are contributing factors to the development of obesity and many non-communicable diseases (NCDs) [678]. In a review paper, Swinburn et al. [6] classified the evidence of the role of diet, nutrition, and physical activity for the prevention and obesity into several categories: ‘convincing’, ‘probable’, ‘possible’, and ‘insufficient’. The intakes of dietary fiber (non-starch polysaccharides) and physical activity were categorized under the ‘convincing’ category and were highly protective against obesity, whereas high intakes of foods that are energy dense but low in micronutrients along with sedentary lifestyles were ‘convincing’ risk factors for obesity. In addition, the frequent intake of sugar-sweetened beverages and heavy marketing strategies used by fast food outlets and manufacturers of energy-dense foods were identified as ‘probably’ obesity risk factors [6]. The national policies on diet-related NCDs in low- and middle-income countries are inadequate and policy responses addressing the challenges of NCDs need to be scaled up to improve the dietary quality and physical activity [7]. The global epidemic of obesity is related to an unbalanced energy intake as the main driver of weight gain as well as dietary quality, which affects the energy balance through complex mechanisms [8]. In addition, the food environment, urbanization, reduced physical activity, and other factors in a broader environmental, societal, and policy context play important roles in explaining the rapid increase in obesity rates [89].
In this study, the dietary intakes were measured in a sample of Malaysian adults and gaps between the recommended levels and current intakes were examined. This study also comparesthe dietary intakes between male and female participants to determine the association between the dietary intake variables and the obesity indicators, i.e., body mass index (BMI) and waist circumference (WC) measurements.
SUBJECTS AND METHODS
Study design
Adults residing in two cities in Malaysia, namely in Penang and Kota Bharu, aged between 20 to 65 years of age and signed a written informed consent, were enrolled in this study using a multistage sampling method. Individuals residing in group living establishments (e.g. institutional dormitories, hostels, or nursing homes) were excluded. This study is a part of a larger research project on physical activity, nutritional status, and neighborhood environment involving 490 adults [10]. The complete profiles of dietary intake (3-day 24-hour dietary recalls with 2 weekdays and 1 weekend day) could be obtained from 422 participants.
This study was approved by the Universiti Sains Malaysia Human Research Ethics Committee (FWA Reg. No: 00007718; IRB Reg. No: 00004494) (Reference Number: (USMKK/PPP/JePeM [246.3(6)(1)])). All participants provided their consent for publication with anonymity.
Instruments
Background information and characteristics
Sociodemographic data were obtained using a set of questionnaires that included information on age, sex, ethnicity, marital status, employment status, level of education, household size, and monthly income.
Anthropometric measurements
The body weight was measured to the nearest 0.1 kg using a SECA digital weighing scale (Model seca clara 803, seca gmbh & co. kg., Hamburg, Germany) according to the standard procedures. The standing height was measured using a SECA bodymeter (Model seca 203, seca gmbh & co. kg., Hamburg, Germany) to an accuracy of 0.1 cm while adhering to the standard procedures. The BMI status of the participants was assessed using the World Health Organization (WHO) BMI classification [1] for adults. The WC was measured using a measuring tape at the point of the minimal waist according to standard procedures [11]. Abdominal obesity was defined as WC measurements cut-off points > 90 cm for males and > 80 cm for females set by the International Diabetes Federation (IDF) [12].
Dietary intakes
This study conducted 3-day 24-hour dietary recalls on 422 participants. Trained enumerators or research assistants performed one-to-one interviews in three separate visits to the participants' homes, which were scheduled carefully to obtain dietary recall information for 2 weekdays and 1 weekend day. This study formed a part of a larger study that collected physical activity data from the participants via the wearing of physical activity monitoring devices for one week, which made possible the numerous home visits and dietary recall interviews.
Food models and household utensils were used to help the participants estimate the portion sizes of the foods and beverages consumed. The dietary intakes (3 recalls per participant) were analyzed using licensed Nutritionist Pro software (Version 6.2, Stafford, Texas, Axxya Systems) and the Nutrient Composition of Malaysian Foods (4th Edition) [13]. The participants' energy, macronutrients, and major micronutrients intake were evaluated and reported. In addition, the intakes of dietary fiber and sugar, as well as the number of servings of the main food groups ((i) breads, cereals, rice, and pasta; ii) Fruits; iii) vegetables; iv) milk, yogurt, and cheese; v) meat; vi) fats, oils, and sweets) were also derived from the dietary recall information.
Statistical analysis
Both descriptive and inferential statistical analyses were conducted using the IBM SPSS Statistics for Windows, Version 25.0 (Armonk, NY, USA). Unless stated otherwise, the descriptive statistics are presented as the mean, standard deviation, and 95% confidence interval. The level of significance was set to P < 0.05. The MIXED model was used to determine the associations between the dietary intake variables and the obesity indicators.
For MIXED model analysis, the responses from the participants are believed to be the sum (linear) of the fixed or random effects. A fixed effect influences the population mean (such as a medical treatment), while a random effect is linked to a sampling procedure (subject effect). The random effect in this study was the subject effect, where the participants were selected or sampled from two different cities in the country via a multistage sampling method. MIXED models can be used under conditions when clustering effects arise from a multistage sampling strategy and allow the modelling of data with skewed distributions.
Several selected dietary intake variables were included in the inferential statistical analysis (MIXED models), i.e., energy, macronutrients, dietary fiber, and total sugar intakes, as well as the average number of servings of fats, oils and sweets, fruits, and vegetables per day. These variables were entered into the MIXED model statistical test and the variables that were not significant were eliminated from the initial model using the stepwise backward elimination method. The covariates included in the MIXED models analysis were age, sex, marital status, education level, employment status, city or study site, and socioeconomic status. These covariates are commonly identified as sociodemographic factors that might affect the outcomes of the study [14].
RESULTS
Participant characteristics
Table 1 lists the general characteristics of the participants stratified according to sex. The mean age of the participants was 40.0 (14.3) years. Among the participants, 35.3% (n = 173) of them were males; 61.8% (n = 173) were married or living with a partner; 50.8% (n = 249) were employed or involved in unpaid work outside the home; and 33.9% (n = 166) had tertiary education. The participants represented various ethnicities of Malaysians, where 71.4% (n = 350) and 25.7% (n = 126) of them were of Malay and Chinese ethnicity, respectively, while the remaining percentage consisted of participants from the Indian and Sikh communities. Approximately 30.0% of the participants received a monthly income of 3,000.00 or more Malaysian Ringgit (MYR).
Anthropometric measurements
Table 2 lists the anthropometric measurements of the participants stratified according to sex. The body weight, height, and WC measurements were significantly higher among the male participants, but the BMI was significantly higher among the female participants. Using the WHO BMI classification, 30.8% of participants were overweight and 22.0% were obese. Based on the WC measurements and cut-offs, 47.5% of them had abdominal obesity.
Dietary Intakes
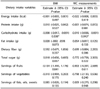
Table 3 summarizes the dietary intakes of the participants obtained from their 3-day 24-hour dietary recall profiles, also stratified according to sex. An additional column showed the summarized recommended range of intakes for both males and females (19 to 65 years old) according to the Recommended Nutrient Intakes for Malaysia (RNI) [15] and the recommendations made by the Malaysia Dietary Guidelines (MDG) [16]. The overall mean and median energy intakes were 1,550 kcal/day and 1,480 kcal/day, respectively. The mean energy intake was lower than the recommended energy intake in the RNI ranging between 63% and 87% of the RNI values, with male participants having a significantly higher energy intake than female participants. In addition, the mean intakes of protein (P < 0.05), carbohydrates (P < 0.001), and fat (P < 0.01) were also significantly higher among the males. The mean protein intakes of the participants exceeded the amount recommended by the Malaysian RNI [15]. In the meantime, the participants had very low dietary fiber intakes than the recommended intake [16] with only a mean of 3.0 ± 2.6 g per day. From dietary intake analysis, the mean intake of total sugar was approximately 28.5 ± 23.3 g per day. No significant differences in dietary fiber and total sugar intakes were detected among both sexes.
With regards to micronutrients, the mean intakes of calcium, Vitamin D, Vitamin E, and folate were lower than the recommended values. The mean intake of calcium was substantially low (490.3 mg) and did not meet the recommended RNI of 800–1,000 mg of calcium for adults. The mean folate intake was also substantially low (87.7 µg) compared to the recommended RNI value (400 µg). The micronutrient intakes were similar in both genders, except for calcium (P < 0.05), niacin (P < 0.05), phosphorus (P < 0.05), and zinc (P < 0.05).
The mean number of servings of fruits consumed by the participants was 0.7 ± 1.0 servings per day, and the number of servings of vegetables consumed was 1.3 ± 1.0 servings per day. The MDG recommends at least five servings of fruits and vegetables every day [16], indicating that the participants' intakes did not reach the recommendations. The MDG and the Malaysian Food Pyramid suggests that Malaysians consume milk and milk products every day, and the participants consumed only a mean of 0.1 ± 0.2 servings of milk, yogurt, and cheese per day. The mean number of servings of fats, oils, and sweets consumed by the participants was 8.9 ± 5.4 servings per day. The male participants consumed a significantly larger number of servings of meat (P < 0.05) and bread, cereals, rice, and pasta (P < 0.001), as well as fats, oils, and sweets (P < 0.01) compared to female participants.
The mean percentage of total energy contributed by macronutrients was 52.4% for carbohydrates, 18.4% for protein, and 29.2% for fat. The percentage of energy contribution recommended by the existing guidelines is 55.0–70.0% for carbohydrates, 10.0–15.0% for protein, and 20.0–30.0% for fat [15]. The mean percentage carbohydrate intake was lower than the recommended percentage, whereas the mean percentage of protein exceeded the suggested percentage range. No significant difference in the percentage of energy contribution by carbohydrate, protein, and fat was found between the sexes.
Differences in anthropometric measurements
Table 4 lists the mean differences in the BMI and WC measurements according to the characteristics of the participants. The participants residing in Kota Bharu had significantly higher BMI and WC measurements than those residing in Penang Island (P < 0.01). Participants who were married or living with a partner had significantly higher BMI and WC measurements (P < 0.001). In addition, participants who were employed in the job market or had unpaid work outside the home had significantly higher WC measurements (P < 0.01), but not BMI. Participants with higher educational qualifications had significantly lower BMI and WC measurements. Moreover, participants of Malay ethnicity had significantly higher BMI and WC measurements than the other ethnicities (P < 0.001). No significant differences in BMI and WC measurements were found between the two income groups.
Table 5 presents the correlation table between the selected dietary variables and the BMI and WC measurements. No significant correlation was observed between these variables and the WC measurements (Table 4). Only the percentage of energy contributed by carbohydrates and fat had significant but weak negative correlations with the BMI.
Dietary intake variables associated with BMI and WC measurements
The MIXED model statistical test was applied to several dietary intake variables, including energy, protein, carbohydrate, and fat intakes, dietary fiber intake, and total sugar intake. In addition, the number of servings of vegetables, fruits, and fats, oils, and sweets were analyzed to determine their associations with the BMI and WC measurements (Table 6). Only the carbohydrate intake had a significant negative association with the BMI (Estimate b = −0.0008; P = 0.038). In the meantime, only the carbohydrate intake, but not the other dietary intake variables had a significant negative association with the WC measurements (Estimate b = −0.019; P = 0.043).
DISCUSSION
Obesity is a consequence of a prolonged positive energy balance and can be influenced by other factors, such as the host (individual), environment (surroundings to which individuals are exposed to), and vector (food and drink consumed) interacting in complex ways that affect the dietary intake and activity patterns [8]. The aims of this study were to (1) assess the dietary intakes in a sample of free-living adults in Malaysia and (2) determine the association between dietary intake variables with the BMI and WC measurements. First, an assessment of the anthropometric indices showed that the proportion of overweight (30.8%) and obese (22.0%) participants in the present study were similar to the proportion of overweight (32.4%) and obese (18.5%) in Malaysian adults in the National Health and Morbidity Survey 2014: Malaysian Adults Nutrition Survey (NHMS 2014: MANS) [17]. In this national level survey, the prevalence of abdominal obesity was 20.0% with a significantly higher prevalence among females (31.8%) and males (9.6%). The proportion of participants with abdominal obesity in the present study was 47.5% with a higher proportion among female participants (53.3%) than their male counterparts (37.0%). This is a worrying trend because the increased prevalence of obesity and abdominal obesity among Malaysians has been and will continue to be a significant burden on the medical costs to treat obesity-related conditions [17]. Sex differences in the anthropometric indicators could be distinguished in the present study, where female participants had a significantly higher BMI but lower WC measurements. Significantly higher BMI and WC measurements were also detected among participants who were married/living with a partner but lower BMI and WC measurements were observed among participants with higher education levels. In the 2014 MANS study, obesity was most prevalent among Malaysians who were married and among those with tertiary level education [17]. In addition, another health survey among adults in five different regions in Malaysia indicated a 33.6% and 19.5% prevalence of overweight and obesity, respectively, with a higher prevalence among females compared to males [18].
In this study, the median energy intake and percentage of total energy contributed by the macronutrients were comparable to the NHMS 2014: MANS, suggesting that the participants had similar dietary intakes to that of an average Malaysian adult. The median energy intake of Malaysians recorded in the NHMS 2014: MANS report [13] was 1466 kcal/day with significantly higher values among men [17]. The median intake of macronutrients among the NHMS 2014: MANS study participants were 195 g of carbohydrate, 57 g of protein, and 46 g of fat. In contrast, the median percentage of the total energy contributed by macronutrients was 55% for carbohydrates, 16% for protein, and 29% for fat. Similar to the present study, the protein intake of adults in the NHMS 2014: MANS slightly exceeded the recommended percentage of 10–15% [15], whereas the carbohydrate and fat intakes were within the recommended percentage.
The mean protein intake of the participants in the present study exceeded the amount recommended by the RNI for Malaysian adults, as well as the percentage of energy contribution for protein that ranged from 10–15% [15]. The mean percentage of energy contributed by fat intake at 29.2% almost exceeded the recommended range of 20–30% [15]. The carbohydrate intake of the participants appeared to have been displaced by the higher protein and fat intake in the diets. As a side note, the average serving of meat consumed among the participants was relatively high with 2.0 ± 1.0 servings per day, which was significantly higher among males. The trend of lower carbohydrate and higher protein intake was also observed in a sample of government servants in an urban area in Malaysia [19], as well as in a larger national survey [17].
A trend of higher protein intake or nutrition transition of increased protein intake from meat and poultry with a decreased carbohydrate intake has been observed globally and was reported in the national food balance sheet [20]. The Food and Agriculture Organization of the United Nations (FAO) [20] reported that the dietary patterns are shifting towards increasing demands and consumption of food from animal origins, including fish. For example, the World Resources Institute reported that the global demand for beef and animal-based foods will likely increase by 95% and 80% between 2006 and 2050 [21]. The growth is expected to be concentrated in urban areas of emerging economies, such as China and India [16]. Malaysia is an upper-middle income country [22] with a thriving economy and its society is currently experiencing a nutrition transition [23]. Indonesia is also undergoing a nutrition transition, where the total energy intake was comprised higher proportions of protein and fat consumption in recent years [23]. The increase in protein intake is consistent with the increased consumption of meat and dairy products, which was parallel to the improving economy and living standards [23]. Nevertheless, more evidence-based prospective observational studies will be needed to confirm this trend. A systematic review and meta-analysis of observational studies confirmed that red and processed meat consumption is associated directly with a higher BMI and WC [24]. In addition, a high intake of meat also predicted more weight gain [25].
An assessment of the dietary intake showed that the consumption of fruits (< 1 serving) and vegetables (< 2 servings) by the study participants was substantially lower than the levels suggested by the MDG, which recommended two daily servings of fruits and three daily servings of vegetables [16]. This has also contributed to the low dietary fiber intake among the participants. Low fruit and vegetable consumption patterns were also observed among the local Malaysian communities in other studies [192627] as well as in the neighboring country of Indonesia, which shares similar socio-cultural practices with Malaysia [28]. The health benefits of a sufficient daily intake of fruits and vegetables in the prevention of major diseases, as well as morbidity and mortality, have been well documented [1629] and the higher consumption of non-starchy vegetables and fruits have been associated with a lower risk of weight gain and obesity [25]. The high intake of dietary fiber was associated with less weight gain, while the intakes of both fruits and dietary fiber were protective against large increases in WC measurements [25]. Therefore, the consumption of fruits and vegetables, as well as foods high in fiber, such as whole grains, should be strongly encouraged and advocated.
In terms of other food groups, the participants had low intakes of milk and milk products that contributed to the low calcium intakes. The number of servings of fats, oils, and sweets combined was approximately nine servings per day, whereas the recommendations clearly indicated that the items from this food group should be consumed in limited amounts. With the mean total sugar intake at 28.4 ± 23.3 g per day and approximately 30.0% of the total energy intake was from fat, it is fair to say that the calorie intakes of the participants of this study were mainly from a high proportion of energy from sugars and fats. Studies have suggested that high intakes of sweets and desserts are linked to more weight gain [2530]. With regards to the correlations between the dietary intakes with obesity indicators, there were no correlations between the total energy intake and macronutrient intakes with the BMI and WC measurements in this study (Table 5). On the other hand, a local study conducted on overweight and obese Malay women reported that the respondents' body weight status is affected by the energy intake, not the macronutrient composition because significant correlations were detected between the total energy intake with the BMI and WC measurements [31].
Further statistical analysis of the data showed that among the dietary intake variables, only the carbohydrate intake was inversely associated with the BMI (Estimate b = −0.008) and WC measurement (Estimate b = −0.019). Other studies also demonstrated associations between the carbohydrate intake and obesity. For example, the cross-sectional Canadian Community Health Survey Cycle 2.2 reported that the risk of overweight and obesity problems was reduced in all quartiles of the carbohydrate intake (between 290 to 310 g/day carbohydrates) compared to its lowest intake category [32]. The authors concluded that a low carbohydrate intake (below 47% of total energy) in healthy adults was associated with a higher likelihood of being overweight or obese. Furthermore, the risk of overweight and obese was reduced to the lowest rate by consuming 47% to 64% of the energy intake from carbohydrates, after accounting for age, sex, income, education, physical activity, and total energy intake [32].
Merchant et al. [32] and Roberts et al. [33] explained the inverse association between carbohydrate intake and body weight. Individuals who consumed more carbohydrates tend to consume larger amounts of fiber, fruits, and vegetables, and less saturated fat [3233]. Dietary carbohydrates from fruits, vegetables and whole grains also have a low glycemic load and are beneficial to human health [3233]. In addition, diets lower in total and saturated fat and higher in carbohydrate intake from whole grains or high-fiber foods, vegetables, and fruits were reported to be protective against weight gain in postmenopausal women in the Women's Health Initiative Dietary Modification Trial [34]. On the other hand, there are also contradicting opinions regarding the relationship between dietary carbohydrates and body weight. The results from an observational study in the USA suggest that the glycemic index of different types of carbohydrates was positively associated with BMI, but not the glycemic load, daily carbohydrate intake, or percentage of energy from carbohydrates [35].
Halkjær et al. [36] examined the associations between the total energy intake and energy intake from macronutrients with the 5-year changes in WC measurements in a large cohort in Denmark after adjusting for age, sports activities, and smoking habits. The authors stated that the total energy intake and energy from macronutrients were not associated with the WC among the respondents after five years, with the exception of an inverse association with animal protein [36]. The intake of refined carbohydrates, such as refined grains, potatoes, and foods with simple sugars was positively associated with the increase in WC, whereas negative associations were detected with carbohydrates from fruits and vegetables [36]. Similar to Merchant [32], only the carbohydrate quantity was investigated in this present study, not the quality or source of carbohydrates, which is a limitation of this study. Future studies should examine the association of carbohydrate or macronutrient intake with obesity to identify the sources or quality of macronutrients clearly. The association detected between the carbohydrate intake with BMI and WC measurements was also rather weak. Nevertheless, because this study was cross-sectional in nature, where the measures of BMI, WC, and dietary intakes were taken at the same point in time, it is difficult to read the association of the dietary intake to BMI and WC. For example, the participants' perception of being overweight and obese may lead the individuals to changing their dietary habits or practice dieting to reduce their body weight. Therefore, prospective observational studies or intervention studies will be needed to relate the dietary intake with body weight.
One of the strengths of this study was the use of standardized measures to obtain the dietary intake, BMI, and WC measurements. Dietary intake data were obtained through a series of 3-day 24-hour dietary recall interviews inclusive of weekdays and weekends by trained interviewers, and an analysis of nutrient intakes using the Nutritionist Pro software was performed by the researchers themselves. Because this study was cross-sectional, the cause and effect could not be inferred. The generalizability of the sample against the Malaysian population may be limited due to the small sample size and the recruitment approach. Nevertheless, this dataset of dietary intakes provides rich and reliable information on the dietary intakes of Malaysian adults. Follow-up studies will be needed to identify the dietary factors that affect obesity in Malaysian adults.
In conclusion, this study assessed the dietary intakes among a sample of free-living Malaysians and identified their dietary intake patterns in comparison to existing guidelines and recommendations. The associations of dietary intake with obesity indicators were also investigated. This study revealed high proportions of overweight and obesity among the study participants. Although the energy intake did not exceed the recommended values, the protein intake was higher than the recommended amounts. The intake of fruits and vegetables as sources of dietary fiber were below the recommendations and the intake of sugars and fats were substantially high among the participants. This study suggests higher intakes of complex carbohydrate-rich foods choices, such as whole grains, fruits, vegetables, and legumes. Overweight and obesity increase the risk of many health issues and is a significant burden on the country's economy and healthcare costs. Changes to Malaysians' dietary intake and lifestyle are urgently needed to halt the escalating prevalence of overweight and obesity.





 XML Download
XML Download