

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Citrobacter species, which are facultative anaerobic Gram-negative bacilli, exist all around us. However, Citrobacter infection is uncommon; they account for 0.8% of all Gram-negative infections and 3%–6% of all isolates of Enterobacteriaceae in nosocomial infection [123]. Furthermore, Citrobacter bacteremia is made up of only a few cases of the whole Citrobacter infection [4]. Citrobacter bacteremia usually occurs in adult patients with underlying diseases such as malignancy and intra-abdominal diseases [4567].
Although, the risk of Citrobacter infection in neonates and immunocompromised patients has been gaining attention [8910], Citrobacter infection is still out of the keen interest. Furthermore, its clinical significance, mortality, and resistance to antibiotics were not accurately evaluated because it was considered to have low virulence [11], low incidence, and to occur only in patients with comorbidities. Recently, the outbreak of Citrobacter freundii bacteremia in a neonatal intensive care unit has attracted public attention in Korea [12].
This study aimed to investigate the clinical characteristics and prognostic factors of Citrobacter bacteremia and compare them with those of C. freundii and non-freundii bacteremia. We also aimed to evaluate the antibiotic susceptibility patterns and trends.
Materials and Methods
1. Study patients
We retrospectively reviewed the medical records of patients with Citrobacter bacteremia between January 2007 and December 2017, at Yeouido St. Mary's hospital, a 450-bed (700-bed before in 2015) university-affiliated hospital. Demographic and clinical characteristics such as age, sex, underlying diseases, primary site of infection, severity of infection, treatment measures and outcome of the enrolled patients and microbiologic data such as identification of Citrobacter spp. and susceptibility to the antimicrobial agents of Citrobacter were obtained. There was one patient who had recurrent episodes of C. freundii bacteremia which were apart more than 16 months and showed different antibiogram between the two isolates. This study was approved by the institutional review board of the Yeouido St. Mary's hospital (no. SC18RESI0115) and informed consent was waived because of the retrospective design of the study.
2. Bacterial isolation and identification
Blood culture was performed using the BD BACTEC™ FX blood culture system (Becton Dickinson, MA, USA). Bacterial identification and antimicrobial susceptibility tests were performed using the Vitek 2 system (bioMérieux, Marcy L'Etoile, France) following the manufacturer's recommendation. Result of the susceptibility test was interpreted based on the Clinical and Laboratory Standards Institute guidelines (CLSI) [131415], and all results were interpreted in accordance with the changed CLSI guidelines. Intermediate susceptibility was defined being resistant.
3. Definitions
Citrobacter bacteremia was defined as detection of an organism isolated from at least one bottle of blood culture with presence of clinical symptoms and signs of infection [5616]. Nosocomial infection was defined as showing a positive result of blood culture obtained 48 hours after admission and presence of symptoms and signs of infection or transferred patients from another hospital with infection [5617]. The primary site of infection was determined based on the clinical features and that was consistent with the laboratory, radiologic and other culture results [56]. Polymicrobial infection was defined as simultaneous isolation of more than one microorganism from blood culture in which Citrobacter was identified [516]. Antimicrobial therapy, provided 3 months prior to admission was considered as recent antibiotic exposure. Appropriateness of empirical antibiotics was defined as the administration of at least one antimicrobial agent, to which Citrobacter was sensitive in vitro, with dosage appropriate for end organ function [56]. Overall mortality included in-hospital death and hopeless discharge. There was one hopeless discharge who gave up further treatment in a very unstable vital sign. Patients who refused treatment or were immediately transferred to another hospital were excluded from the prognostic factor analysis.
4. Statistical analysis
Categorical variables were analyzed using the χ2-test or Fisher's exact test. Student's t-test for parametric methods for Charlson comorbidity index or Mann-Whitney test for non-parametric methods were performed for other continuous variables. Multivariate logistic regression was performed to define the risk factors for death using all significant variables with a P-value of less than 0.1 in the univariate analysis and known risk factors in previous studies [4567]. A backward selection process was used. Multicollinearity was verified using variance inflation factors. A two-sided P-value of less than 0.05 was considered significant. All statistical analyses were performed using SPSS software 21 (SPSS Inc., Chicago, IL, USA).
Results
1. Clinical characteristics of the patients
From January 2007 through December 2017, 43 episodes of Citrobacter bacteremia were identified and annual incidence was presented in Figure 1. There was no clustering of cases, which were suspected as outbreak during the study period. The median age was 72 years with a range of 24–93. No pediatric case was observed. Twenty-nine (67.4%) cases had bacteremia caused by C. freundii and 14 had non-freundii bacteremia (six of C. braakii, five of C. koseri, two of C. amalonaticus and one of C. youngae). A total of 39 (90.7%) patients had comorbidities. Hepatobiliary and pancreatic diseases including malignancy were the most common underlying diseases (Table 1). The median age of four patients without underlying diseases was 28.5 years (range of 24-61). Three of four patients, had Citrobacter bacteremia that originated from appendicitis and one was unknown.

Table 1
Clinical characteristics and outcome of the patients with Citrobacter bacteremia

The intra-abdominal infection (32/43, 74.4%) including the hepatobiliary tract, urinary tract, and gastrointestinal tract was the most common portal of entry. Hepatobiliary tract was the leading primary site both in community-acquired and nosocomial infections (38.5% and 52.9%, respectively). Twenty-one (48.8%) patients had polymicrobial bacteremia, which consisted of eight isolates of Klebsiella spp., seven of Enterococcus spp., three of Escherichia coli, two of Pseudomonas spp., two of Streptococcus spp., two of Enterobacter spp., one of Staphylococcus aureus, and one of Actinomyces odontolyticus. A total of 26 (60.5%) patients had community-acquired infection and 10 (23.3%) had recent antibiotic exposure. In 17 (39.5%) patients with nosocomial infections, the hepatobiliary tract (9/17, 52.9%) was the most common site of infection, followed by the central line-associated blood stream infection (4/17, 23.5%) and a case of urinary tract infection, skin and soft tissue infection, gastrointestinal tract infection, and primary bacteremia, respectively. No significant difference in clinical features was observed between C. freundii and non-freundii bacteremia. The detailed characteristics are presented in Table 1.
2. Treatment outcome and risk factors for death
Of 43 episodes, 39 (90.6%) were treated with antibiotics. Four patients were not treated because they were transferred to other hospitals or refused treatment because their underlying diseases were already at terminal stage. Out of 39 patients treated with antibiotics, 36 (92.3%) received appropriate initial antibiotics, which consisted of third-generation cephalosporins (22/39, 56.4%, such as cefoperazone-sulbactam, ceftriaxone, and ceftazidime), piperacillin-tazobactam (9/39, 23.1%), quinolones (3/39, 7.7%), carbapenems (2/39, 5.1%), ampicillin-sulbactam (2/39, 5.1%), and cefuroxime (1/39, 2.5%). Among three patients who did not receive appropriate empirical antibiotics (two isolates showed resistance to third-generation cephalosporins and one showed resistance to piperacillin-tazobactam), two patients received appropriate antibiotics within a week after the result of the susceptibility test was obtained. The time interval between blood culture and administration of appropriate antibiotics tended to be longer in the non-freundii group (mean day, 0.46 days in the freundii group vs 3.23 days in the non-freundii group, P = 0.057). Furthermore, the duration of antibiotics use and length of hospitalization were longer in the non-freundii group, but were not significant (Table 1). Nine (20.9%) patients were inserted with the following drainages; pig-tail catheter for ascites in five patients, percutaneous transhepatic biliary drainage (PTBD) or percutaneous transhepatic gallbladder drainage in four patients, and internal biliary stent in one patient. One patient was inserted with a pig-tail catheter for ascites and PTBD at the same time.
Overall mortality was (8/43, 18.6%) and was not significantly different between patients with freundii bacteremia and those with non-freundii bacteremia (4/29, 13.8% vs. 4/14, 28.6%, P = 0.454). In univariate analysis, Charlson comorbidity index, Pitt bacteremia score and undergoing invasive drainage procedures were significant predictors of patients' outcome (Table 2). The multivariate analysis did not show any independent risk factors for mortality. However, Charlson comorbidity index, Pitt bacteremia score, and undergoing invasive drainage only showed trends to be related to death (Table 2).
Table 2
Risk factors for mortality in patients with Citrobacter bacteremia

3. Antimicrobial susceptibilities
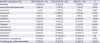
Antimicrobial susceptibility data were available in 42 blood isolates, and rate of antimicrobial susceptibility are presented in Table 3. Comparing the first 6 years (from 2007 to 2012) and the last 5 years (from 2013 to 2017), no change was observed in the rate of resistance to the tested antibiotics. Additionally, no significant difference in antimicrobial susceptibilities was observed between C. freudii and non-freundii (data not shown). Compared with community-acquired infection, Citrobacter spp. isolated from patients with nosocomial infection had decreased susceptibility to ceftazidime (22/25, 88.0% vs. 8/17, 47.1%; P = 0.011) and aztreonam (22/25, 88.0% vs. 9/17, 52.9%; P = 0.029). All isolates were susceptible to carbapenems.
Table 3
Antimicrobial susceptibility rates of Citrobacter isolates
Discussion
We analyzed the clinical characteristics, treatment outcome and antibiotic susceptibility rates of 43 patients with Citrobacter bacteremia at a single institute in Korea. No significant difference in clinical features and antimicrobial susceptibility rate was observed between C. freundii and non-freundii bacteremia. Since previous studies on Citrobacter bacteremia in Korean people had been conducted more than 15 years ago [5], our data could show recent trends.
No pediatric case was observed, and there was no clustering of cases. Although the incidence of Citrobacter bacteremia appears to be high in 2014, compared to other years, species and the patterns of antimicrobial susceptibility of the isolates were diverse. We could not find any epidemiologic relations. Majority of patients were elderly people with a median age of 72 years, which was 15 years older than the average age of 55.6 years reported in the previous domestic study by Kim et al. [5]. More than 90% of the enrolled patients had at least one or more comorbidities, which was similar to those reported in previous studies [461819]. However, Citrobacter bacteremia could occur in young and healthy patients, even in neonates [8]. In our study, four patients without underlying diseases had a median age of 28.5 years, and all of them survived. Several studies reported that Citrobacter bacteremia primarily occurs in the urinary tract [471820]. By contrast, hepatobiliary tract was the most common primary site of community-acquired and nosocomial infections in our study as other reports [562122]. Polymicrobial infection accounted for almost half of Citrobacter bacteremia cases, which was relatively high, compared with 35.2% in previous study by Kim et al. [5]. The most possible reason is that Citrobacter bacteremia is mostly derived from intra-abdominal infection. Therefore, we should consider the possibility of co-infection with Enterobacteriaceae and Enterococcus spp. and choice empirical antibiotics. Unlike previous studies, in which nosocomial infection was predominant (77%–94.6%) [571823], community-acquired infection (60.5%) was dominant in our study. Our hospital was changed from a tertiary hospital to a secondary hospital in 2015, which is thought to have contributed to this finding. Because tertiary hospitals receive patients from primary and secondary hospitals in Korea, nosocomial infections are likely to be more common. Knowing whether Citrobacter bacteremia is caused by community-acquired infection or nosocomial infection is important in choosing appropriate empirical antibiotics. Although nosocomial acquisition does not affect the mortality rate, it could affect antimicrobial susceptibility rates. We presented that the rate of resistance to ceftazidime and aztreonam was significantly higher in isolates from nosocomial infections than in community-acquired infections.
The mortality of Citrobacter bacteremia was reported to be between 16.6–48.3% [56721]. Polymicrobial infection is known to increase mortality and length of hospital stay among adults. In addition, stay in the intensive care unit, nosocomial infection, and sources of bacteremia other than the urinary tract are also considered as risk factors for death [56724]. We showed that Charlson comorbidity index and Pitt bacteremia score were associated with the overall mortality. Therefore, the underlying conditions and severity of initial presenting symptoms and signs are the most important determinants of outcome. Although Charlson comorbidity index was possible factor for mortality, we could not find any statistical significance in individual underlying diseases such as metastatic malignancy or diabetes with complications. Undergoing invasive drainage procedure was a significant risk factor for death in the univariate analysis but not in the multivariate analysis, which was different from that reported in previous studies [56]. One possible reason is that six out of nine patients underwent the drainage procedure with the disease progressing considerably. Another reason is that five patients had an insertion of pigtail catheter as palliative treatment and not as an active therapeutic procedure.
Increasing resistance to extended spectrum cephalosporins in Citrobacter spp. has been reported [45252627]. Moreover, there is a consensus that Citrobacter isolates have become increasingly drug-resistant even for aminoglycosides and quinolones [2829]. However, we could not find an increase in the rate of resistance to the 15 examined antimicrobial agents (100% susceptible to ertapenem, data not shown) between the first 6 years (from 2007 to 2012) and the later 5 years (from 2013 to 2017). There has been another concern that susceptibility patterns differed substantially between C. freundii and non-freundii isolates. However, there was no significant difference in susceptibility rate between C. freundii and non-freundii isolates. Although it was lower than the previously reported data in Korea [5], the rate of resistance to second- and third-generation cephalosporins in our study was considerable; the rates of resistance to cefoxitin, cefotaxime, and ceftazidime were 85.7%, 28.6%, and 28.6%, respectively. On the contrary, carbapenems, cefepime, and amikacin were still promising against Citrobacter spp. To the best of our knowledge, the susceptibility rate of Citrobacter spp. to carbapenem is between 97% and 100% [45], although carbapenem-resistant Citrobacter infection is emerging [30]. It accounted for 1.9% of all carbapenemase producing Enterobacteriaceae reported in Korea in 2016 [31]. Thus, more attention should be paid to infection with multidrug-resistant Citrobacter spp.
This study showed the different clinical characteristics and antibiotic susceptibility rate of Citrobacter spp. between medical institutions even in the same city and country. This is the most recent clinical study in Korea, and it can serve as a basis when treating patients with Citrobacter bacteremia. Because the data in this study are limited due to the small number of patients in a single institute and retrospective study design, a multicenter study with a large sample size is ongoing.
In conclusion, Citrobacter bacteremia is predominant in the elderly with comorbidities. Hepatobiliary tract is the leading primary focus of bacteremia both in community-acquired and nosocomial infections. The clinical features of Citrobacter bacteremia were not different between C. freundii and non-freundii bacteremia. The rate of susceptibility to antibiotics has not changed during the last 11 years. Isolates that cause nosocomial infections are more resistant to third-generation cephalosporin and aztreonam. Co-morbidity and severity of initial manifestations are critical for outcome.
 XML Download
XML Download