

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
More than 30% of patients are undernourished, not only of hospitalized patients but also of nonhospitalized patients undergoing surgical procedures [12]. It has been suggested that nutritional depletion increases the risk of postoperative complications, such as surgical site infection, infectious disease, etc. [3456]. For this reason, various screening tools have been developed and used in order to assess preoperative nutritional status. These nutritional risk screening (NRS) tools include subjective global assessment (SGA), patient-generated SGA (PG-SGA), abridged patient-generated SGA (aPG-SGA), malnutrition universal screening tool (MUST), nutritional risk index (NRI), Onodera's prognostic nutritional index (PNI), and NRS-2002 [23789101112].
Perioperative mortality has become a rare event following pancreaticoduodenectomy (PD), occurring in less than 5% of cases at high-volume pancreatic surgery centers [131415]. Despite a significant reduction in mortality after PD, however, morbidity remains high, ranging from 30%–60% in some reports [141617]. The most serious morbidity following PD is pancreatic fistula (PF), which can occur in 20% of patients [171819]. Because of serious complications such as postoperative pancreatic fistula (POPF), the perioperative mortality rate of PD in high-volume centers is reportedly 1% to 2%, and even as high as 40% [320]. This POPF is associated with prognostic nutrition indexes such as serum albumin and total lymphocyte count [32122]. Therefore, the nutritional index is a risk factor of postoperative complication after PD.
However, there is no nutritional screening tool widely accepted as the gold standard for detecting patients at risk of malnutrition and predicting postoperative complications. In previous reports, fragmentary and partial factors have been identified to assess the risk of malnutrition in the individual NRS tools mentioned above. Therefore, we investigated subjective parameters such as weight loss, dietary intake loss, and nutrition impact symptoms in addition to objective parameters such as albumin, total lymphocyte count, and body mass index (BMI). In this study, we have developed a model to analyze and evaluate nutritional indicators in an integrated manner. The aim of this study was to determine if the NRS tool could predict postoperative complications in patients who underwent PD.
Go to : 
METHODS
This study was approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (2018-06-034). Written informed consent was waived by the IRB. Since January 2010, we have prospectively investigated nutritional risk factors such as albumin, total lymphocyte count, BMI, weight loss, dietary intake loss, and nutrition impact symptoms. Patients who underwent PD for periampullary cancer in Ewha Womans University Mokdong Hospital from January 2010 to December 2016 were identified retrospectively. As a concept of PD, the operative procedures performed included conventional Whipple operation, pylorus-preserving pancreaticoduodenectomy (PPPD), and laparoscopic PPPD. Periampullary cancer included pancreatic cancer, distal common bile duct cancer, and ampulla of Vater cancer. We excluded combined surgery and any previous cancer history, except for prostate cancer, thyroid cancer, and skin cancer except for melanoma.
NRS tools such as SGA, PG-SGA, aPG-SGA, MUST, NRI, Onodera's PNI, and NRS-2002 were analyzed (Table 1). These parameters included age, albumin, total lymphocyte count, BMI, weight ratio, weight loss, dietary intake loss, nutrition impact symptoms such as dysphagia, dysfunction, physical examination, and disease severity. First, the objective parameters were age, albumin, total lymphocyte count, BMI, and weight ratio. Age was excluded because recent reports have found acceptable complications after PD in the elderly, even in patients over 80 years of age [23242526]. Moreover, we also excluded weight ratio because it overlapped with BMI. Therefore, the objective category of NRS tools was composed of albumin, total lymphocyte count, and BMI. Second, the subjective parameters included weight loss, dietary intake loss, nutrition impact symptoms such as dysphagia, physical examination, dysfunction, and disease severity. Physical examination, dysfunction, and disease severity were excluded. Physical examination includes a subjective evaluation of three aspects of body composition: loss of subcutaneous fat (below eye, triceps, biceps, and chest), muscle wasting (clavicle, scapula, ribs, quadriceps, deltoids, etc.), and fluid states (ankle edema, sacral edema, and ascites) [38910]. Dysfunction, evaluated by the patients themselves, includes working suboptimal, ambulatory, or bedridden state [810]. Disease severity, evaluated by a health professional, refers to a disease state affecting nutritional requirements. In this study, we excluded physical examination because it was performed and assessed subjectively by a health professional, e.g., physician, nurse or dietitian. Dysfunction was excluded because patients may describe it subjectively with substantial differences depending on the patient's cognitive ability and other factors. Furthermore, disease severity was also excluded because the severity of each periampullary cancer is similar, with few differences between cases. Therefore, the subjective risk factors included weight loss, dietary intake loss, and nutrition impact symptoms such as dysphagia. We defined the following variables. Definition of weight loss: If patient had a weight loss of more than 5% within the last 6 months. Dietary intake loss and nutritional symptoms were subjectively assessed by nurse or nutritionist with interview. Patients were defined as a significant decrease in the amount of food during the last 2 weeks or having complaints such as difficulty swallowing.
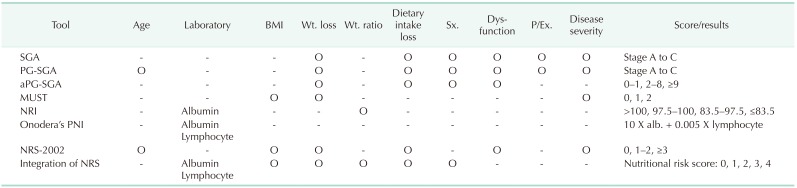
Table 1
Comparison of nutritional risk screening tools
BMI, body mass index; Wt., weight; Sx., symptom; P/Ex., physical examination; SGA, subjective global assessment; PG-SGA, patient-generated subjective global assessment; aPG-SGA, abridged patient-generated subjective global assessment; MUST, malnutrition universal screening tool; NRI, nutritional risk index; PNI, prognostic nutritional index; NRS, nutritional risk screening.
![]()
We analyzed 128 patients who underwent PD for periampullary cancer. The patients were divided into two groups according to the risk factors: the non-risk group (65 patients) and the NRS risk group (63 patients). The nonrisk group was defined as patients without NRS risk factor, and the NRS risk group was defined as patients with at least one NRS risk factor. Following this classification, patient characteristics and postoperative complications were retrospectively investigated in each group.
Patient characteristics included sex, age, BMI, weight loss, pancreatic duct size, preoperative laboratory findings such as albumin and lymphocyte, and postoperative outcomes such as total complications, serious complications, estimated blood loss (EBL), POPF, clinically relevant POPF (CR-POPF), readmission, and postoperative hospital duration. We reviewed CT images to measure pancreatic duct size at the portal vein level, and confirmed the EBL in surgical records and anesthesia records. Statistical analysis was also performed to analyze the risk factors of POPF. However, the textures of pancreas were not recorded during surgery, so it could not be analyzed for prediction of POPF.
Postoperative complications included general complications and complications specific to pancreatic surgery. General complications included wound dehiscence, complicated fluid collection, ileus, delayed gastric emptying, biliary leakage, incisional hernia, pleural effusion, pneumonia, voiding difficulty, glucose intolerance, portal vein thrombosis, sepsis, colitis, and acute cerebral infarction. Complication severity was classified according to Clavien-Dindo classification grade [27]. Clavien-Dindo classification grade II or more was considered significant. In addition, the specific complication of pancreatic surgery included only POPF after PD. The diagnosis of POPF was made with the drain output of any measurable volume of fluid on or after postoperative day 3 with amylase content 3 times greater than serum amylase activity, according to the International Study Group for Pancreatic Fistula (ISGPF) [2128]. Severity of POPF was graded as grade A, B, or C [152128]. Grades B and C POPF was defined as CR-POPF. Postoperative complications were investigated for 30 days after surgery. Mortality was defined as death within 90 days following surgery.
The primary end-point of the study was overall complications. The second end-point was the postoperative recovery course such as readmission, postoperative hospital duration, and complication severity.
The categorical variables are presented as number (percent). The continuous variables are presented as mean ± standard deviation. The categorical variables were compared with the Chi-square, Fisher exact, or Student t-test. Multivariate analysis was performed for all variables using a logistic regression test. All statistical significances were determined at P < 0.05.
Go to :
RESULTS
Patient characteristics
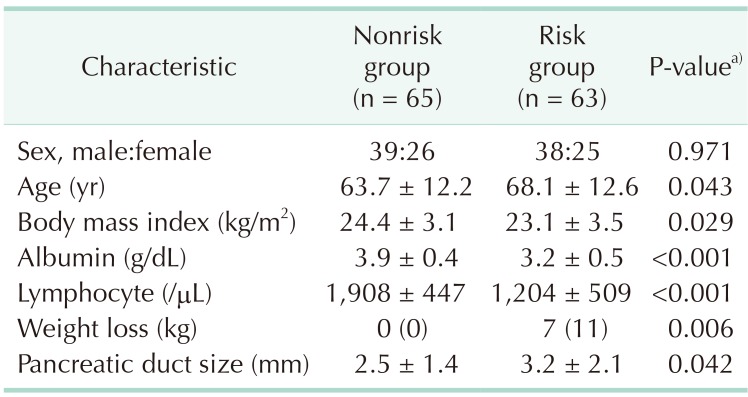
Of the 128 study patients, 65 patients (51%) were in the nonrisk group and 63 patients (49%) were in the risk group. There were 39 males and 26 females with mean age 63.7 ± 12.2 years in the nonrisk group, and 38 males and 25 females with mean age 68.1 ± 12.6 years in the risk group. There was no difference in term of gender composition between the 2 groups, however, the mean age was significantly higher in the risk group than in the nonrisk group (68.1 ± 12.6 vs. 63.7 ± 12.2, P = 0.043). BMI was significantly lower in the risk group than in the nonrisk group (23.1 ± 3.5 vs. 24.4 ± 3.1, P = 0.029). Moreover, preoperative laboratory findings were compared between the nonrisk group and the NRS risk group. There were also significant differences in albumin (3.2 ± 0.5 vs. 3.9 ± 0.4, P < 0.001) and total lymphocyte count (1,204 ± 509 vs. 1,908 ± 447, P < 0.001), favoring the nonrisk group. Furthermore, there was significantly more weight loss in the risk group than in the nonrisk group (7% vs. 0%, P = 0.006). Additionally, the diameter of pancreatic duct size was significantly larger in in the risk group than in the non-risk group (3.2 ± 2.1 vs. 2.5 ± 1.4, P = 0.042) (Table 2).
Postoperative outcomes
There were no significant differences between the 2 groups in terms of EBL, POPF, and readmission. However, CR-POPF (grade B or C) rates were significantly higher in the NRS risk group than in the nonrisk group (24% vs. 9%, P = 0.029). Also, the risk group was associated with a higher rate of overall complications (60% vs. 31%, P = 0.001) and serious complications (41% vs. 15%, P = 0.001), as well as a longer postoperative hospital duration (22.1 ± 12.0 vs. 18.1 ± 7.4, P = 0.022) (Table 3).
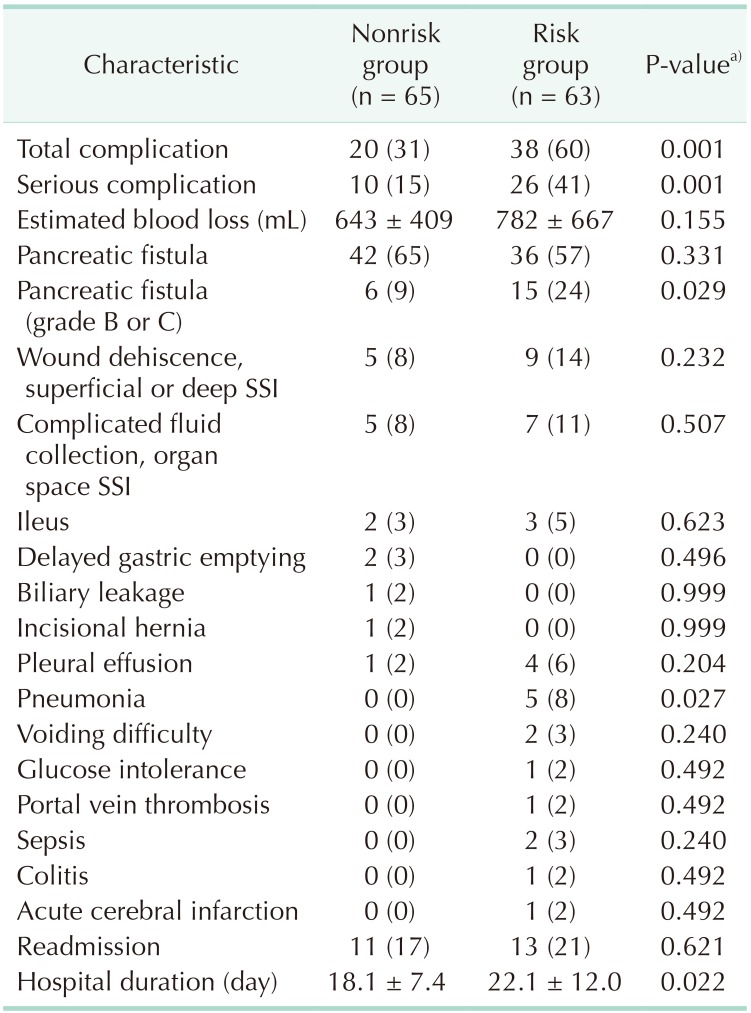
Of the postoperative general complications, there were no differences between the 2 groups in terms of wound dehiscence, complicated fluid collection, ileus, delayed gastric emptying, biliary leakage, incisional hernia, pleural effusion, voiding difficulty, glucose intolerance, portal vein thrombosis, sepsis, colitis, and acute cerebral infarction. However, postoperative pneumonia was seen significantly more in the NRS risk group than in the nonrisk group (8% vs. 0%, P = 0.027). As a concept of complications specific to pancreatic surgery, POPF was diagnosed in 78 of 128 patients (61%) according to the ISGPF criteria. If the severity of POPF was classified as grade B and C, CR-POPF (grade B or C) occurred in 21 of 128 patients (16%). In the nonrisk group, the POPF and CR-POPF rates were 65% and 9% of 65 patients, respectively. In the NRS risk group, however, the POPF and CR-POPF rates were 57% and 24% of 63 patients, respectively (P = 0.331 and P = 0.029, respectively). Therefore, the NRS risk group was associated with a higher rate of CR-POPF (24% vs. 9%, P = 0.029) (Table 3). There was no 90-day mortality in this series.
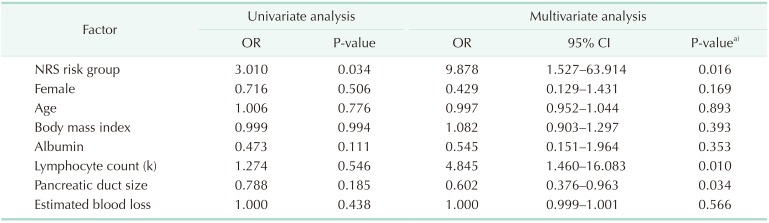
Univariate analysis showed a significant difference in the NRS risk group (odds ratio [OR], 3.010; P = 0.034). Furthermore, multivariate analysis revealed being in the NRS risk group, a lower total lymphocyte count, and a larger pancreatic duct size to be significant risk factors for CR-POPF (NRS risk group: OR, 9.878; 95% confidence interval [CI], 1.527–63.914; P = 0.016; lower total lymphocyte count: OR, 4.845; 95% CI, 1.460–16.083; P = 0.010; larger pancreatic duct size: OR, 0.602; 95% CI, 0.376–0.963; P = 0.034). In other words, NRS risk group was a significant factor of CR-POPF (Table 4).
Go to :
DISCUSSION
We have prospectively investigated preoperative nutritional status since January 2010. We retrospectively reviewed our series of 128 patients to analyze whether nutritional risk factors are associated with postoperative complications. Of the 128 patients, 65 patients (51%) had no NRS risk, and 63 patients (49%) had at least one NRS risk factor according to the integration of NRS tools. Among the preoperative variables, BMI and laboratory findings such as albumin and total lymphocyte count were significantly lower in the NRS risk group than in the nonrisk group, while age was significantly higher in the NRS risk group. There was significantly more weight loss in the NRS risk group than in the nonrisk group. In addition, NRS risk group was associated with a larger pancreatic duct diameter size. Regarding the postoperative variables, NRS risk group was associated with a higher rate of total complications, serious complications, CR-POPF (grade B or C), and a longer postoperative hospital duration. In other words, CR-POPF, the only specific complication following PD, was seen significantly more in the NRS risk group (24% vs. 9%, P = 0.029). Of the individual general complications, only pneumonia was seen significantly more in the NRS risk group (8% vs. 0%, P = 0.027). As a result, postoperative complication and CR-POPF rates were significantly higher in the NRS risk group with one or more nutritional risks as identified by the objective factors of NRS tool. As analyzed in Table 4, being in the NRS risk group was identified as a statistically significant and independent predictor of CR-POPF after PD in multivariate analysis (P = 0.016) as well as univariate analysis (P = 0.034). Therefore, these findings suggest that the integration of NRS system can be a preoperative predictive model for postoperative complications and CR-POPF in patients undergoing PD.
The reported NRS tools for predicting postoperative complications include SGA, PG-SGA, aPG-SGA, MUST, NRI, Onodera's PNI, and NRS-2002 [23789101112]. Although these various NRS tools have already been recognized in preoperative risk stratification [3], NRS scoring systems collectively integrating objective parameters (albumin, total lymphocyte count, and BMI) and subjective parameters (weight loss, dietary intake loss, and nutrition impact symptoms) have not been employed in any previous studies. Of the previous NRS tools, aPG-SGA, MUST, and NRS-2002 belonged to the NRS scoring system, however, objective parameters such as albumin, total lymphocyte count, and/or BMI were excluded. In a recent investigation, scoring systems combing several factors have been proposed to more accurately predict the risk of POPF [1921]. In this study, thus, we have integrated and scored the objective and subjective parameters together to comprehensively assess preoperative nutritional status. Finally, among the various parameters, the nutritional risk tool included albumin, total lymphocyte count, BMI, and subjective risk factors (weight loss, dietary intake loss, and dysphagia). In this study, we found out the NRS risk group was shown to be independently associated with CR-POPF after PD by multivariate analysis.
The incidence of CR-POPF (grade B or C) was 16%, which was similar to that reported by previous studies (13.2%–17%) [1621]. In the nonrisk group, the CR-POPF rate was 9%. If there was at least one NRS risk factor, the rate rose to 24% (P = 0.029). The reason why being in the NRS risk group was associated with a higher rate of CR-POPF seems to be that physical tolerance against surgical trauma becomes weaker with nutritional depletion. The other reason why is that nutrition plays an integral role in PD for periampullary cancer, not only preoperatively but also postoperatively [3]. For these reasons, if patients are identified as part of the NRS risk group prior to surgery, nutritional intervention should be provided early in treatment so as to prevent CR-POPF after PD. This preoperative nutritional support may be very important in the postoperative recovery course, because CR-POPF is the principal cause of postoperative morbidity and mortality [2029].
Furthermore, postoperative pneumonia was significantly more in the NRS risk group; the reason for this may be that the undernourished patients are in poor physical condition, causing their immune systems to weaken. This finding may be associated with the lower lymphocyte count in the NRS risk group found by multivariate analysis (OR, 4.845; 95% CI, 1.460–16.083; P = 0.010). To prevent postoperative pneumonia, when we detect patients at risk of malnutrition, we should also support preoperative nutrition. Moreover, the result that the CR-POPF and pneumonia rates were higher in the NRS risk group may be associated with a longer postoperative hospital duration (22.1 ± 12.0 vs. 18.1 ± 7.4, P = 0.022). If patients are screened for NRS nutritional risk, and are appropriately supported with preoperative nutrition, then the average mortality and postoperative hospital duration as well as overall complications can be expected to decrease in the future. In future studies, the efficacy of preoperative nutritional support in patients in the NRS risk group should be prospectively evaluated.
The present study has several limitations. First, the main limitations of this study are its retrospective nature as well as selection bias. The pancreas texture, known to be associated with POPF, could not be analyzed due to the limitation of the retrospective study. Second, the possibility of bias related to the historical background cannot be eliminated. For example, it is not possible to eliminate the possibility of bias related to subjective risk factors such as weight loss, dietary intake loss, and nutrition impact symptoms such as dysphagia. In addition to these biases, patients were overestimated because a subjective risk factor is scored as one point in analysis, even if there is one of weight loss, dietary intake loss, and dysphagia. In fact, the NRS risk group was measured at 49% in our study, unlike the more than 30% rate seen in previous studies. Third, the number of patients is relatively small and may be underpowered for some statistical analyses. To further validate our present findings, a prospective study in a larger number of patients is needed.
In conclusion, there were statistically significant associations between complications and nutritional indicators. A comprehensive analysis of nutritional parameters will help predict postoperative complications and CR-POPF after PD.
Go to :
 XML Download
XML Download