

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alzheimer's disease (AD) is a debilitating neurodegenerative disease that leads to serious limitations in everyday functioning due to an irreversible deterioration in cognitive impairment. The burden on the caregivers of people with dementia (CGPWD) may be far greater for AD than for any other disease. About 3.5 million family members—including spouses, children, and grandchildren—are involved in dementia care, spending average times of 6–9 hours per day.1 Many CGPWD are not professional caregivers, and most of them do not receive adequate training or education on how to care for dementia patients. In addition, dementia patients inevitably deteriorate during the natural course of the disease. This situation makes CGPWD vulnerable to increased physical, psychological, social, and financial burdens,2 which affect not only the primary caregivers but also all of the family members of dementia patients. CGPWD have been referred to as ‘hidden patients’345 due to their reduced quality of life and increased risks of severe depression, cardiovascular morbidity, and mortality associated with caregiving. Other detrimental consequences such as negative self-emotion and dysfunctional thoughts about the patient are also reported frequently.6
Behavioral and psychological symptoms of dementia (BPSD) that are exhibited by 80–90% of dementia patients78 are the most significant factor influencing the caregiver burden of dementia3 and the institutionalization of dementia patients.910 The primary care for patients is provided in the home since most caregivers are the family members of dementia patients. The long-term increased burden of dementia care reduces the actual quality of the care provided, which has a negative impact on the patient either directly or indirectly. Multicomponent programs that include education, psychosocial support, and cognitive behavioral therapy (CBT) are known to have positive effects on CGPWD. A recent systematic review demonstrated that CBT was an effective intervention tool for reducing various the emotional burdens experienced by CGPWD.11
While multicomponent intervention programs including CBT are well known to have positive effects on CGPWD in many countries worldwide, their effectiveness has not yet been demonstrated in randomized controlled trials in South Korea. We therefore developed a therapeutic intervention program for caregivers of people with dementia (I-CARE), focusing on reducing the burden experienced by the dementia caregivers.12 We aimed to determine the efficacy of the I-CARE program through a multicenter, randomized clinical trial.
METHODS
Participants
The caregivers of possible and probable AD patients based on the criteria of the National Institute of Neurological and Communicative Disorders and Stroke-Alzheimer's Disease and Related Disorders Association and the Diagnostic and Statistical Manual of Mental Disorders (fifth edition) were enrolled between May 2014 and January 2017. Eligibility criteria for dementia patients were as follows: 1) the severity of dementia as assessed by a score on the global Clinical Dementia Rating Scale13 of 0.5–2.0, 2) a total score of 10–26 on the Korean version of the Mini Mental State Examination (K-MMSE),14 and 3) presence of BPSD within last 6 month to 1 year. Inclusion criteria for the dementia caregivers was as follows: 1) a primary caregiver who has been taking care of a patient for longer than 6 months, 2) providing an average of >4 hours of care per day, 3) caring for an immediate family member aged 30–80 years, 4) literate and normal cognition as assessed by the score on the K-MMSE (within one standard deviation above), 5) difficulties in coping with BPSD as evaluated by a distress score of >2 on the Resources for Enhancing Alzheimer's Caregiver Health II scale,15 and 6) providing informed consent for participating in this study. Subjects were excluded if either a patient or a caregiver had a serious medical condition that could interfere with the study, any neurological or psychiatric disorder, or did not provide informed consent. Physicians kept the doses of medications taken by the dementia patient stable throughout the study.
Study design
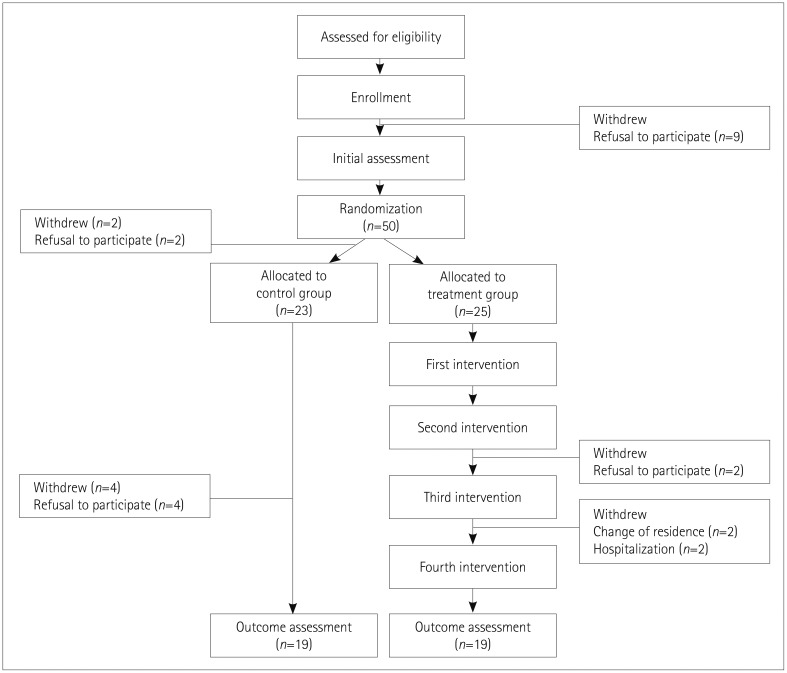
This multicenter, randomized, clinical controlled study was performed in eight dementia specialized centers of neurology and neuropsychiatry departments (Fig. 1). When the eligible caregivers were recruited by the principal investigators, the dementia-specialized clinical research coordinator (CRC) at each center evaluated the inclusion and exclusion criteria. If the decision to be included in the study is made, informed consent was obtained and the baseline evaluation was performed by the CRC. These decisions were made and the information about the participant obtained by the psychologist of each center. Finally, the information was sent to the main investigation center (Ewha Womans University Mokdong Hospital, EWU-MH) by the psychologist at each center. The participating clinical research associate at EWU-MH generated a random allocation sequence using the SAS program (version 9, SAS Institute Inc., Cary, NC, USA) to randomly assign subjects to either the immediate intervention group (treatment condition) or a wait-list control group (control condition) using a fixed randomization scheme with assignment based on a table of random numbers generated by a psychologist of each institution. The interventions were then administered to the participants in the treatment group by the psychologists. The outcomes of both groups were measured twice—at baseline and within 2 weeks after the last visit—by the CRC at each center who was blinded to the status of each group.
The study was conducted in accordance with the International Harmonization Conference Guideline on Good Clinical Practice and was approved by the Institutional Review Board of EWU-MH (IRB No. 2014-12-028). Informed consent was provided by all the participating subjects.
Therapeutic intervention program for caregivers of people with dementia
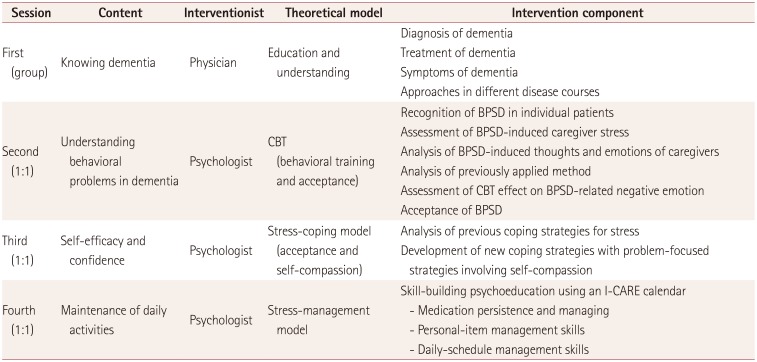
The I-CARE program was mainly developed by EWU-MH based on experience of previous research16 by two neurologists (J.H. Jeong & G.H. Kim) and two neuropsychologists (J. Yeom & R. Yoo). The final program was revised according to feedback from an experienced psychologist (Y. Kang). The I-CARE program is a comprehensive multimodal intervention that includes education, psychological support, and daily memory training, and each session takes 60 minutes (Table 1). The first and fourth sessions were typically separated by 8–10 weeks. The first session was performed in a group by the patient's physician, while the remaining three sessions were carried out individually by a trained psychologist.
The first educational session provided basic information about diagnosis of dementia, clinical symptoms, behavioral changes, management, prognosis, and future expectations based on current scientific developments. This session comprised a lecture lasting 40 minutes followed by 20 minutes for questions and answers. The goal of the second session was to minimize the negative thoughts about dementia of CGPWD through understanding the behaviors of patients using CBT. Caregivers were asked about the most disturbing BPSD of the patient and their emotions. They were then also requested to explain how negative emotions or thoughts would affect their lives. When a caregiver made inquiries about the appropriate coping strategies, a psychologist and the caregiver discussed how to avoid the situation, which was mostly related to problematic behaviors of a patient. They also talked about how to accept that those disabling symptoms were unintentional since they were simply caused by organic brain damage.
The third session focused on stress experienced by the caregivers. The question, “what would you do if you get free time?” was given to discover new activities that the caregiver desired to relieve stress. A psychologist then explained the reasons why realistic stress-coping activities were necessary for caregivers. Obstacles to implementing stress-coping activities were explored, and discussion was carried out on how to eliminate or reduce these obstacles.
The fourth session was targeted at teaching daily activities that could compensate the memory impairments of dementia patients. Caregivers were asked about whether they had ever applied any method to help or enhance the memory ability of their dementia patients. Caregivers were encouraged to apply nonpharmacological treatments of dementia, such as daily activity training in order to maximize the residual memory ability of the patients. Information about the following three memory training methods was provided:
1) Memory training for taking medications: The caregiver was taught how to encourage the patient to take drugs by themselves and mark this on a calendar. For example, if a patient takes medications three times per day, they should be trained to mark the dates with different signs, such as to draw a circle on the date for the morning drug, to mark a cross inside the circle for the daytime drug, and to color the circle for the night drug. The caregiver was asked to check and train the patient until they learned to do it by themselves.
2) Memory training to manage belongings: The goal of this training was to reduce the delusion of theft, which might be associated with the patient not being able to remember the place to put their personal belongings. Patients often become more obsessed about an item if it has meaning to them. A caregiver was asked to pick three important items for a patient and keep them in a place both that the patient and the caregiver knew. The next day, the patient was asked about the location, and if they could not find it, the caregiver would help the patient to find it. The same procedure should be repeated to train the patient until he or she remembers the location.
3) Memory training to manage schedule: Patients often forget dates, and so most of the caregivers provided information about the dates of doctor appointments or personal events. Together with a caregiver, a patient could learn to manage their weekly schedule by writing schedules for the next week on a calendar at the beginning of the week. The caregiver lets the patient check the schedule every morning and then remove items from it when they have been completed.
Outcomes
The primary efficacy outcomes were caregiver burden and depression. The Korean version of the Zarit Burden Interview (ZBI-K) was used to assess the caregiver burden.17 This scale evaluates the subjective perception of caregiving such as emotional and physical burdens, economic difficulties, and limitations in social activities due to caregiving of dementia patients. This self-report questionnaire consists of 22 items for measuring the subjective stress level on a 5-point Likert scale (from 0=‘never’ to 4=‘nearly always’), with a higher score indicating a higher care burden. Depression was measured by a 30-item version of the Geriatric Depression Scale (GDS).18
The secondary outcome measures evaluated the effects on the quality of life, self-emotion, acceptance, and compassion of the caregivers. The Korean version of the Philadelphia Geriatric Center Morale Scale (PGCMS) was used to assess the quality of life and subjective well-being of the elderly.19 The scale comprises 17 items that measure nonagitation, attitude toward one's own aging, and life satisfaction on a 5-point Likert scale (from 1=‘strongly disagree’ to 5=‘strongly agree’), with a higher score indicating a lower quality of life. The Caregiver-Administered Neuropsychiatric Inventory (CGA-NPI) measures the degree of burden experienced by caregivers due to 12 abnormal behaviors.20 The Positive Affect and Negative Affect Schedule (PANAS) is a self-report evaluation tool comprising adjectives representing positive and negative emotions.21 This 20-item scale has 10 positive-affect and 10 negative-affect items, each of which is evaluated on a 5-point Likert scale (from 1=‘very slightly or not at all’ to 5=‘extremely’), with a higher score indicating a higher level of affect. The Korean version of the Acceptance and Action Questionnaire-II (AAQ-II) assesses the degree of experiential acceptance and experiential avoidance. The AAQ-II measures the degree to which a person is acting in a way that is appropriate to their own values and purpose, and the degree to which they are willing to accept the pain or feelings resulting from it, or to avoid or control their personal experience.22 The scale consists of 10 items and is evaluated on a 7-point Likert scale (from 1=‘never true’ to 7=‘always true’), with a higher score indicating a higher level of psychological acceptance. The Korean version of the Self-Compassion Scale (SCS) assesses the degree of self-compassion.23 This 26-item scale captures the way of being kind and understanding toward oneself in moments of turmoil, and each statement is rated on a 5-point Likert scale (1=‘almost never’ to 5=‘almost always’), with a higher score indicating a higher level of self-compassion.
Statistical analysis
The data were analyzed using the SPSS program (version 21.0, IBM Corp., Armonk, NY, USA). The independent-samples t-test and chi-square test were applied to the demographic variables to confirm homogeneity between the treatment and control groups. The independent-samples t-test was also used to confirm the homogeneity of the two groups for the dependent variables before applying the I-CARE program. In order to confirm the changes in each group at postintervention, the pre- and postintervention results of the dependent variables were analyzed using the paired t-test, which was also used to analyze differences between the treatment and control groups.
RESULTS
Fifty caregivers from eight centers agreed to participate to the program. Twelve withdrew their consent during the study due to refusal to participate, change of residence, or personal reasons (hospitalization). The remaining 38 participants were randomly assigned to either the treatment group (n=19) or the control group (n=19).
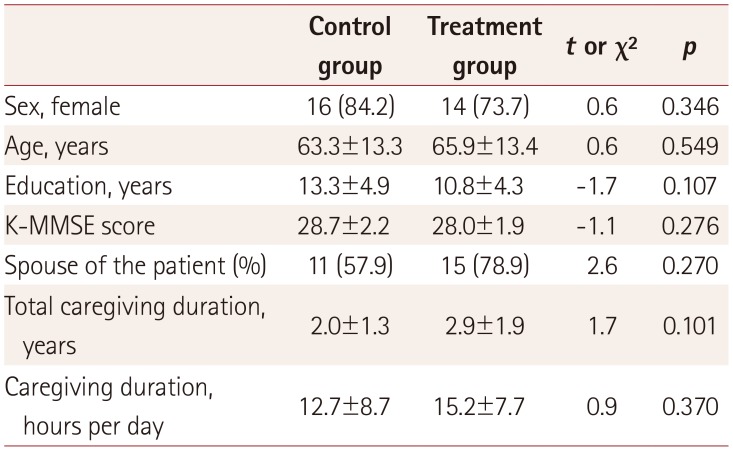
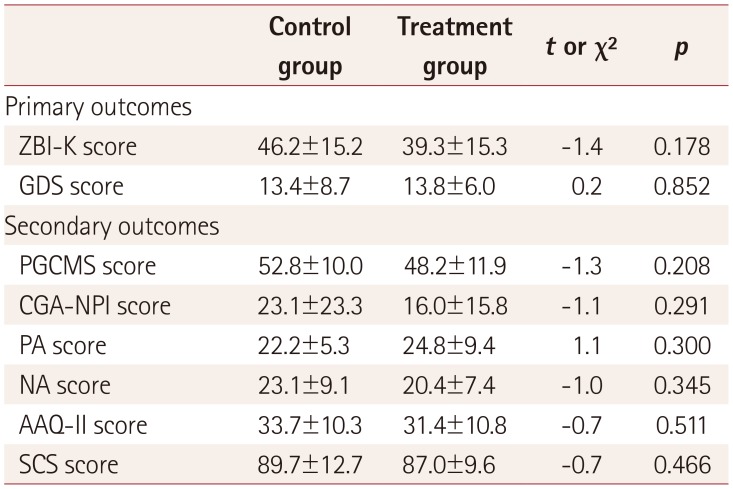
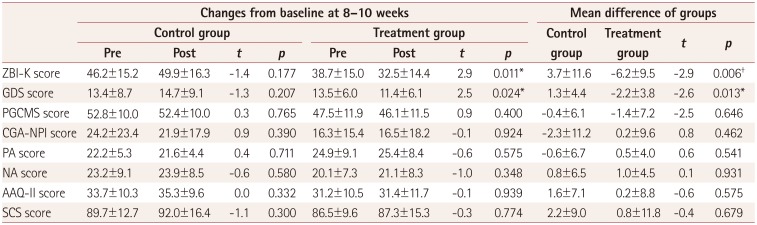
There were no significant intergroup differences in demographic variables (Table 2). The baseline outcome measures showed slightly higher scores on the ZBI-K, PGCMS, and CGA-NPI in the control group. However, there were no statistical significant differences in homogeneity tests between the treatment and control groups (Table 3). The results for the efficacy variables are presented in Table 4. Compared to the control group, the treatment group showed significant improvement in the primary outcome of the ZBI-K and GDS scores at postintervention. The score on the ZBI-K at postintervention was significantly improved in the treatment group compared to that in the control group [6.2-point decrease vs. 3.7-point increase, t(37)=−2.9, p<0.01]. In the treatment group, the burden of care was reduced after participating in the program [t(18)=2.9, p<0.05]. There was a significant difference in the GDS score between the two groups at postintervention [t(37)=−2.6, p<0.05], and this score in the treatment group was significantly reduced after the invention program (2.2-point decrease vs. 1.3-point increase, t(18)=2.5, p<0.05).
There were no significant differences in the secondary outcome measures—including PGCMS, CGA-NPI, PANAS, AAQ-II, and SCS scores—between pre- and postintervention.
DISCUSSION
The application of the I-CARE program in this study produced a significant improvement in the burden of care and depression among caregivers as a primary efficacy assessment in the treatment group compared to the controls. This result suggests that participation in such a program may help to reduce the psychological burden and the severity of depression by providing active interactions with professionals and increasing the understanding of dementia. Furthermore, these results are in accordance with the goals of the I-CARE program to alleviate the burden of care for the CGPWD by increasing their knowledge, psychological intervention using CBT, stress management, and learning skills for the daily activity. Although we provided only minimal short-term interventions, they produced positive results for the primary outcome measures.
The ‘National Responsibility System for Dementia’ policy launched in September 2017 by the Korean government presented several methods for promoting a dementia-friendly social environment and improving the awareness of dementia.1 Emotional support bases such as counseling and case management have been offered in order to reduce the psychological and physical burdens on dementia caregivers. The I-CARE program is expected to further improve the management of dementia patients at the national level and to alleviate the social burdens experienced by the increasing number of CGPWD. It is important to change negative emotions and behaviors toward dementia as well as to provide caregivers with accurate information about dementia. Therefore, by providing an education session by a dementia specialist, the I-CARE program helps the caregiver to understand the disease. In addition, through repetitive individual sessions run by a psychologist, a caregiver can learn not only realistic coping strategies for abnormal behaviors exhibited by a dementia patient, but also the skills to maintain the remaining abilities of a patient. Such support with empowered knowledge can encourage a caregiver to have positive attitudes toward both the patient and themselves. If all dementia clinics provide these programs, this will reduce or delay the institutionalization of dementia patients and facilitate long-term family care.
This study has important implications in that the I-CARE program provided a systematic and effective framework for reducing the burdens on CGPWD based on a variety of psychotherapeutic approaches used in current clinical practice, although there is no reimbursement support for providing programs to CGPWD in dementia special-care centers. It is also meaningful that the I-CARE program could provide detailed methods of intervention, such as videos or manual, for use in clinical practice. These valuable results have been attributed to the investigators overcoming many difficulties such as a lack of trained psychologists or clinical overload in the setting of the study.
Unfortunately, there were no significant intergroup differences in the quality of life of the caregivers, abnormal behaviors of AD patients, positive and negative emotions, experiential acceptance and avoidance, and finally self-compassion. These findings could be related to the methods applied in this study and the cause of the disabling symptoms. The intervention in this study might have been too short to elicit changes in coping style or the stress that has lasted for months or longer, thereby producing negative results for all secondary outcomes. In particular, BPSD, which are the most common cause of caregiver burden, are induced by pathological changes in degenerative brains. In addition, the CGPWD seemed to have more negative attitudes both emotionally and behaviorally when dealing with dementia patients.24 These factors make it difficult to produce positive changes only by changing the attitude of caregivers in a short period of training. It is important for CGPWD to change their negative attitudes toward dementia because these attitudes considerably impact the caregiver burden as well as the disease progression.
CBT is undoubtedly one of the primary treatment strategies and is used to facilitate the cognitive and behavioral coping skills of individuals facing problematic personal issues and life circumstances. CBT addresses the stressors by improving both cognitive and behavioral skills. The cognitive skills of CBT are helpful in overcoming dysfunctional beliefs and automatic thought processes,12 while behavioral skills are beneficial in reinforcing clients to take alternative actions/choices and thus feel more at ease in situations that are otherwise stress-inducing. Because people with dementia often require a huge amount of support from others in various dimensions, psychological and physical skills in overcoming these difficulties are inevitably required for CGPWD. While studies of the treatment efficacy in CGPWD are not uncommon, research producing clinically significant results using CBT is still scarce. Above all, our study is the first to apply an intervention program including CBT in South Korea.
This study was subject to a few limitations. The small number of participants hampered the ability to verify the severity of dementia and the effectiveness of the relationship between the caregiver and the patient. Also, the long-term effect of the I-CARE program was not evaluated in this study. A follow-up study needs to investigate the effectiveness of the program based on the relationship with the patient and the personal characteristics of the caregiver. A comparative investigation should be conducted of the most appropriate intervention method considering the cognitive changes according to the severity of dementia in future studies in order to replicate these results. It is also required to examine how long the effects last for through continuous follow-up after the program finishes. Lastly, whether a direct or indirect intervention (e.g., telephone interview, use of application, or brochure provision) could prolong the effect of the program after the end of the session should also be studied in the future.
 XML Download
XML Download