

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Acquired ocular motor nerve palsy (OMNP) is a common cause of acute diplopia in neurological practice.1234 Acquired OMNP can result from various causes including trauma, intracranial tumors, stroke, aneurysm, and microvascular ischemia.1234 Prompt diagnosis and treatment are important in acquired OMNP since it can lead to death if appropriate treatment is not applied.5678 The largest series from the Mayo Clinic that included 4,278 patients identified abducens nerve palsy as the most common type of OMNP (44%), but also the cause could not be determined in 25% of cases.9 Other studies have found various etiologies depending on the included population and the criteria used to determine the etiology.1011121314151617 However, most studies of acquired OMNPs have been limited by their retrospective designs, being performed only in ophthalmology clinics, and the nonavailability of advanced neuroimaging techniques that can reliably detect small intra-axial lesions.
A few recent studies have prospectively assessed the underlying etiologies of isolated OMNP, and the efficacy of emergency neuroimaging.18192021 Isolated OMNP in patients aged ≥50 years frequently occurs from presumed microvascular ischemia of the nerve in the presence of vascular risk factors, while the reported frequency of causes other than microvascular ischemia has ranged from 4% to 17%.192021 However, there has been no prospective study of an Asian population with isolated OMNP, and no study has investigated the clinical features for guiding neuroimaging with the inclusion of a control arm.
We conducted a prospective multicenter study to investigate the underlying etiologies of acquired OMNP in neurology clinics. We also attempted to estimate the frequency of microvascular ischemia and other causes in a Korean population with isolated OMNP, and sought to determine the clinical features that may predict causes other than microvascular ischemia.
Go to : 
METHODS
Study design and participants
We performed a prospective multicenter study that recruited 298 patients with acquired OMNP from the neurology clinics of 9 university hospitals in Korea between January and December 2015. The inclusion criteria were 1) acquired binocular diplopia within 30 days of onset and 2) diplopia due to OMNP. Exclusion criteria were a prior history of strabismus, orbital diseases, congenital OMNP, diplopia due to extraocular muscle disorders, neuromuscular junction (NMJ) disorders, nuclear or supranuclear disorders, inability to undergo MRI, history of neurological diseases that can influence cognitive function, or incomplete data.
During the study period, 412 patients with acquired binocular diplopia were initially recruited. After excluding 114 patients with nuclear or supranuclear palsy (n=46), NMJ disorders (n=27), other causes (n=21), extraocular muscle disorders (n=11), and incomplete data (n=9), 298 patients with acquired OMNP were finally selected for this study (Fig. 1).
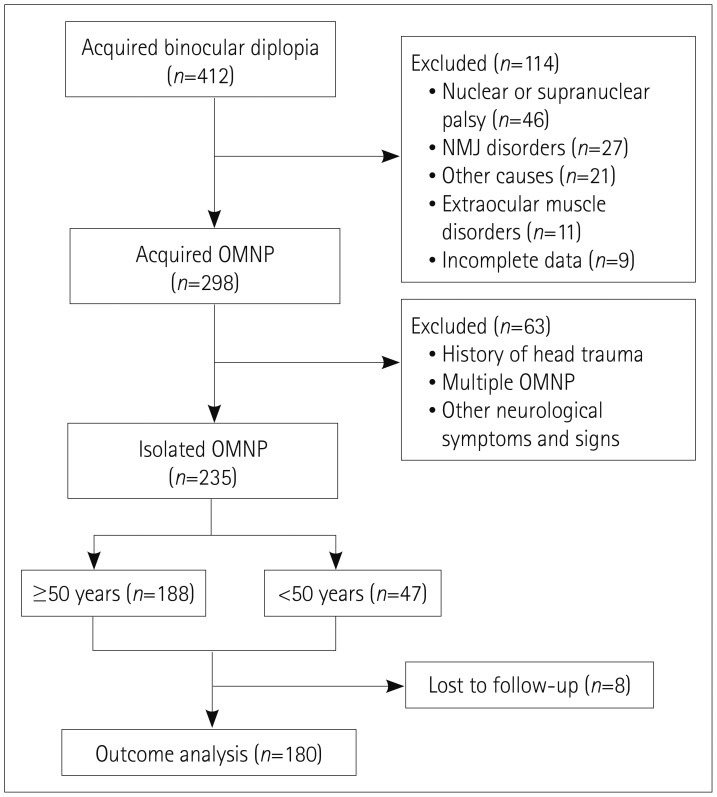 | Fig. 1Study flow diagram. Initially, 412 patients with acquired binocular diplopia were recruited, and 298 with acquired OMNP were selected for this study after excluding those with nuclear or supranuclear palsy, neuromuscular junction disorders, other causes, extraocular muscle disorders, and incomplete data. Among 298 patients with acquired OMNP, we further selected 235 with isolated OMNP after excluding patients with a history of preceding head trauma, multiple OMNPs, or other neurological symptoms and signs. We divided the patients with isolated OMNP into two groups according to their age: <50 years and ≥50 years. The outcome analysis was applied to 180 patients with isolated OMNP. NMJ: neuromuscular junction, OMNP: ocular motor nerve palsy.
|
We defined isolated OMNP as the absence of neurological signs and symptoms other than headache or periorbital pain. Among 298 patients with acquired OMNP, we further selected 235 with isolated OMNP after excluding 63 patients with a history of preceding head trauma, multiple OMNPs, or other neurological symptoms and signs. We divided the patients with isolated OMNP into two groups according to their age: <50 years (n=47) and ≥50 years (n=188).
We collected data using a structured registration form that included demographic features, clinical characteristics (the frequency and intensity of headache, ocular pain, neurological signs, vascular risk factors, and a history of previous infection, head trauma, or cancer), the results of radiological and laboratory evaluations, treatments, and prognosis.
This study followed the tenets of the Declaration of Helsinki and was approved by Institutional Review Board of Pusan National University Hospital (approval no. 1605-001-041). Informed contents were obtained after the nature and possible consequences of this study had been explained to the participants.
Diagnostic procedure
All participants underwent imaging of the brain and orbit with MRI including diffusion-weighted imaging (DWI) and MR angiography. The laboratory evaluation included complete blood counts, routine chemistry, thyroid function tests, antithyroid antibodies, serum anti-acetylcholine-receptor antibody, repetitive nerve stimulation test, and neostigmine test to exclude extraocular muscle or NMJ disorders. Vascular risk factors were defined: aged ≥60 years, hypertension, diabetes mellitus, smoking, previous stroke or myocardial infarction, coronary artery disease, and dyslipidemia. We assessed the serum anti-GQ1b antibody level in patients with antecedent infection or decreased deep tendon reflexes, and performed CSF analysis in patients with accompanying headache.
Using the previously reported criteria for the etiologies of ophthalmoplegia, the cause of each type of acquired OMNP was assigned according to the medical history, results of radiological and laboratory evaluations, and clinical course.591722 Appropriate lesions should have been documented in neuroimaging to diagnose cerebral infarctions, brain tumors, inflammation, and vascular disorders. A diagnosis of Tolosa-Hunt syndrome was based on the 2018 criteria of the International Headache Society.23 A diagnosis of microvascular ischemia required no alternative cause in MRI and clinical tests, the presence of at least one vascular risk factor, and spontaneous resolution. When there were no identifiable causes, the etiology was classified as undetermined.
In patients with isolated OMNP, we used the recently reported criteria for a diagnosis of presumed microvascular ischemia that was assigned to those patients for whom MRI and clinical testing did not reveal an alternative cause, other neurological signs remained absent, and the ophthalmoparesis resolved spontaneously.1921
Treatment strategy and outcome measurement
Patients with isolated OMNP due to other causes received conservative, medical, or surgical treatments according to the underlying etiologies, while the remaining patients with microvascular ischemia were followed up without receiving any specific treatment.
All of the patients who were diagnosed with isolated OMNP were followed up for at least 6 months, and the outcome was considered as resolved when both the tropia and diplopia disappeared.
Statistical analysis
A logistic regression analysis was used to assess the independent predictors of other causes in patients with isolated OMNP. Variables with p<0.05 in the univariate analysis were considered to represent explanatory variables. Chi-square or Fisher's exact tests were used to compare the proportion of men, each OMNP, and etiologies between the younger (age <50 years) and older (≥50 years) patients. Statistical analyses were performed using SPSS (version 18.0, SPSS Inc., Chicago, IL, USA), and p<0.05 was considered significant.
Go to :
RESULTS
The patients with acquired OMNP comprised 185 men (62%) and 113 women (38%) aged 58±15 years (mean±SD), with a median age of 59 years and an age range of 9 to 88 years. The acquired OMNPs included abducens nerve palsy (40%), oculomotor nerve palsy (27%), trochlear nerve palsy (23%), and multiple OMNPs (10%) (Table 1). The etiologies of acquired OMNP were microvascular ischemia (47%), inflammation (21%), undetermined (13%), stroke (5%), trauma (5%), neoplasm (3%), others (2%), carotid cavernous fistula (CCF, 2%), and aneurysm (1%). The causes of each OMNP were mainly microvascular ischemia, inflammation, and undetermined, but the frequencies of trauma and neoplasm were somewhat higher in trochlear nerve palsy and abducens nerve palsy, respectively. The main cause of multiple OMNPs was inflammation (73%).
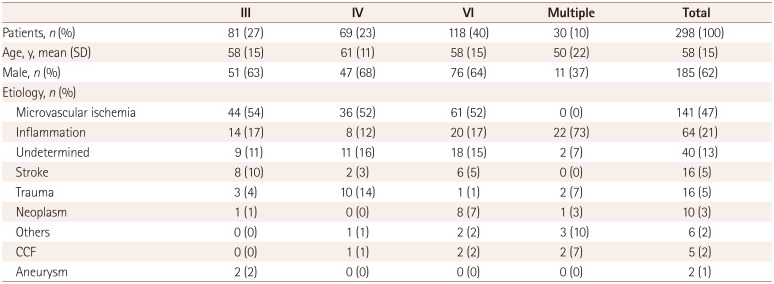
Table 1
Demography and etiologies of acquired OMNP
![]()
The 188 patients aged 50 years with isolated OMNP included 122 men (64%) and 66 women (36%) aged 65±8 years, with a median age of 64 years and an age range of 50 to 88 years. Isolated OMNP had an etiology of microvascular ischemia in 83% of cases, with the remaining 17% comprising inflammation (6%), stroke (6%), neoplasm (3%), and aneurysm (1%) (Table 2). Inflammatory disorders comprised Tolosa-Hunt syndrome (n=7), pachymeningitis (n=3), and demyelinating disease (n=1). Inflammation and stroke were the most common other causes of isolated oculomotor and trochlear nerve palsies, while neoplasm and stroke were most frequent in abducens nerve palsy.
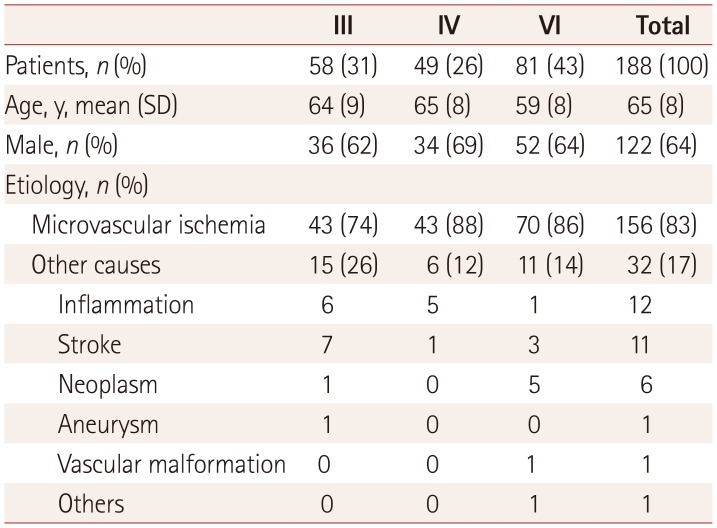
Table 2
Demography and etiologies of patients aged 50 years and older with isolated OMNP
![]()
The presence [odds ratio (OR)=2.9, 95% CI=1.3–6.3] and a higher intensity of headache significantly increased the risk of causes other than microvascular ischemia in isolated OMNP, whereas the presence of vascular risk factors (OR=0.4, 95% CI=0.2–0.9) was more likely to be associated with microvascular ischemia (Table 3). However, there were no differences in the frequency of a history of previous infection or cancer, pupillary involvement, pupil-sparing partial third-nerve palsy, or the degree (complete vs. partial) of external ophthalmoplegia between OMNP due to microvascular ischemia and OMNP due to other causes.
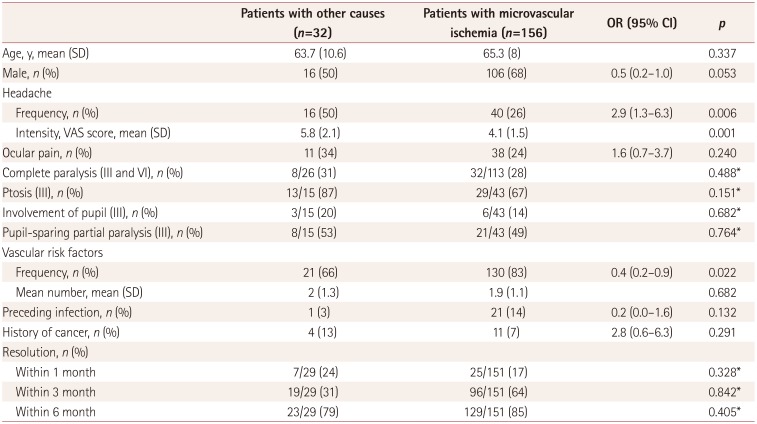
Table 3
Comparison of clinical characteristics between patients with isolated OMNP due to microvascular ischemia and other causes
![]()
Almost all of the patients (n=180) were followed up for at least 6 months. Most of them (149/180, 83%) showed complete resolution within 6 months of the symptom onset with or without receiving treatment. Complete resolution was observed in 85% of OMNP cases due to microvascular ischemia and in 69% of OMNP cases due to other causes (Table 4). The proportion of complete resolution did not differ between OMNP due to microvascular ischemia and OMNP due to other causes at 1, 3, or 6 months after the onset of symptoms.

Table 4
Outcome of isolated ocular motor nerve palsy
![]()
Compared to the younger patients (age <50 years) with isolated OMNP (n=47), patients aged ≥50 years had a significantly higher frequency of microvascular ischemia (83% vs. 49%, p<0.001) and a lower prevalence of other causes (17% vs. 51%, p<0.001) (Table 5). The frequency of each OMNP did not differ between the two age groups.
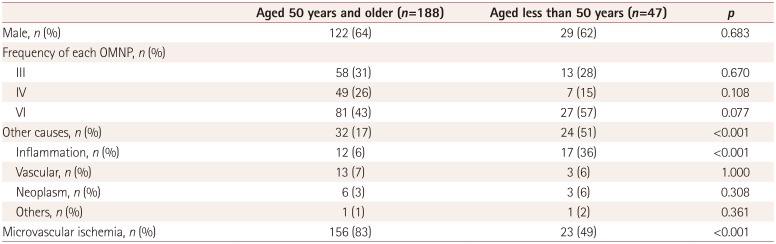
Table 5
Comparison of characteristics between patients aged 50 years or more and less than 50 years in isolated OMNP
![]()
Go to :
DISCUSSION
This prospective study found that abducens nerve palsy was the most common (40%) type of OMNP in neurology clinics, and that multiple OMNPs occurred in 10% of cases. The etiologies included microvascular ischemia (47%), inflammation (21%), stroke (5%), trauma (5%), neoplasm (3%), and others (2%), with the cause not being determined in 13% of the patients. Compared to previous retrospective studies from ophthalmology clinics, the prevalence of multiple OMNPs, vascular disorders (microvascular ischemia, stroke, CCF, and aneurysm), and inflammation was higher in our study, whereas those of trauma and undetermined cause were lower.91011121314151617 These discrepancies in the distribution of the affected nerves and underlying etiologies may be due to differences in the study populations, designs, and inclusion criteria applied for a cause of microvascular ischemia. Vascular risk factors were defined more broadly in the present study than in previous studies. Furthermore, the entire population in this study received MRI including DWI, and we systematically assessed serum anti-GQ1b antibody levels and CSF. These procedures might have increased the prevalence of vascular and inflammatory disorders and other causes, while decreasing the proportion of cases with an undetermined cause. A lower prevalence of trauma may indicate that patients with traumatic OMNP are more likely to be managed by ophthalmologists. Our results necessitate the assessment of vascular and inflammatory causes of patients with acquired OMNP in neurological practice.
Since the possibility of secondary causes has been considered to be higher in acquired OMNP associated with neurological findings or multiple OMNPs, attention has recently been paid to isolated OMNP. Three prospective studies of Western populations found that when OMNP was isolated in patients aged ≥50 years, microvascular ischemia accounted for more than 80% of cases (Table 6),192021 with the frequency of causes other than microvascular ischemia varying from 4% to 17%. Consistent with this, in our Korean population we found a frequency of causes other than microvascular ischemia of 17%. However, the distribution of other causes in this study differed from that in the previous studies. In our study, the other causes were mostly vascular disorders (13/32, 41%) and inflammation (12/32, 38%), while common causes in the previous studies were tumors (14/31, 45%) and inflammation (7/31, 23%).192021 Furthermore, the main causes of inflammation were Tolosa-Hunt syndrome and pachymeningitis in our study, and giant-cell arteritis in previous ones.
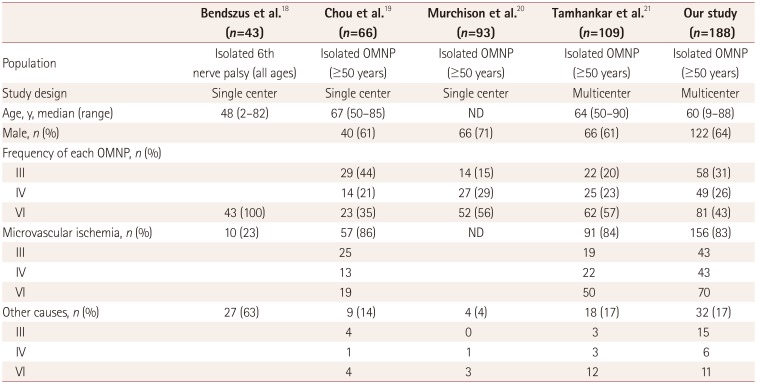
Table 6
Summary of previous and our studies on isolated OMNP
| Bendszus et al.18 (n=43) | Chou et al.19 (n=66) | Murchison et al.20 (n=93) | Tamhankar et al.21 (n=109) | Our study (n=188) | |
|---|---|---|---|---|---|
| Population | Isolated 6th nerve palsy (all ages) | Isolated OMNP (≥50 years) | Isolated OMNP (≥50 years) | Isolated OMNP (≥50 years) | Isolated OMNP (≥50 years) |
| Study design | Single center | Single center | Single center | Multicenter | Multicenter |
| Age, y, median (range) | 48 (2–82) | 67 (50–85) | ND | 64 (50–90) | 60 (9–88) |
| Male, n (%) | 40 (61) | 66 (71) | 66 (61) | 122 (64) | |
| Frequency of each OMNP, n (%) | |||||
| III | 29 (44) | 14 (15) | 22 (20) | 58 (31) | |
| IV | 14 (21) | 27 (29) | 25 (23) | 49 (26) | |
| VI | 43 (100) | 23 (35) | 52 (56) | 62 (57) | 81 (43) |
| Microvascular ischemia, n (%) | 10 (23) | 57 (86) | ND | 91 (84) | 156 (83) |
| III | 25 | 19 | 43 | ||
| IV | 13 | 22 | 43 | ||
| VI | 19 | 50 | 70 | ||
| Other causes, n (%) | 27 (63) | 9 (14) | 4 (4) | 18 (17) | 32 (17) |
| III | 4 | 0 | 3 | 15 | |
| IV | 1 | 1 | 3 | 6 | |
| VI | 4 | 3 | 12 | 11 |
![]()
We found that the underlying causes of isolated OMNP differed significantly with patient age. The prevalence of microvascular ischemia was significantly higher in the older than the younger group (83% vs. 49%, p<0.001), whereas other causes showed the opposite relationship (17% vs. 51%, p<0.001). A recent prospective study of isolated sixth-nerve palsy found a higher incidence of other causes (63%) and a lower incidence of microvascular ischemia (23%), since patients of all ages were analyzed together. Our results again emphasize the importance of considering patient age when evaluating acute isolated OMNP.
The traditional guidelines based on retrospective studies of imaging patients with acute isolated OMNP have included 1) younger than 50 years, 2) pupil-involving or pupil-sparing partial third-nerve palsy, 3) a history of any type of cancer, 4) any other localizing signs or symptoms, 5) no improvement within 1 month, and 6) no resolution within 3 months.19,20,24 The present study compared various clinical variables between patients with isolated OMNP due to microvascular ischemia and OMNP due to other causes. We found that only the presence and a higher intensity of headache were risk factors for causes other than microvascular ischemia, whereas the presence of vascular risk factors is more likely to be associated with microvascular ischemia. There were no intergroup differences in the proportion of cases that resolved at 1, 3, and 6 months after symptom onset, or in the frequency of a history of previous infection or cancer, pupillary involvement or pupil-sparing partial third-nerve palsy, or the degree of external ophthalmoplegia. Our results are consistent with previous studies also finding no difference in the degree of external ophthalmoplegia and pupillary involvement between cranial third-nerve palsies due to microvascular ischemia and other etiologies.719 Indeed, approximately one-third of patients with cranial third-nerve palsy due to microvascular ischemia are known to show some degree of pupillary involvement.62425
The present study was subject to several limitations. Since the study was based on data from the neurology clinics of tertiary-care hospitals, the obtained results might not be applicable to community hospitals or ambulatory-care units. The possibility of selection bias should also be considered when interpreting the results. Microvascular ischemia is a presumptive diagnosis based on no alternative causes and spontaneous resolution with or without the presence of vascular risk factors. Since the criteria for microvascular ischemia do not entirely rule out alternative etiologies such as myasthenia gravis, a longer follow-up may be required to establish a definitive diagnosis of OMNP due to microvascular ischemia.
Go to :
 XML Download
XML Download