

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Follicular thyroid cancer (FTC) is the second most common thyroid cancer and constitutes approximately 10% of all thyroid malignancies (1). In Korea, FTC accounted for 1.6% of all thyroid cancers in 2015 (2). FTC can only be confirmed by pathological examination after diagnostic thyroidectomy and not by fine-needle aspiration cytology or frozen sections. Histologic diagnosis of FTC is based on the demonstration of follicular cells occupying abnormal positions, including capsular and/or vascular invasion. Minimally invasive FTCs have limited capsular and/or vascular invasion. Widely invasive FTCs have widespread infiltration of adjacent thyroid tissue and/or blood vessels (3). FTC typically spreads via hematogenous routes which occurs in 10% to 15% of cases with metastases to distant organs, most commonly involving the lung followed by bone rather than the lymph nodes. The brain, liver, and skin are less common sites of systemic metastases (14).
The prognoses for FTC are worse than those for papillary thyroid carcinomas (PTC). In differentiated thyroid carcinoma, follicular histology is a significant factor for survival, and the 3-year survival rate for papillary and follicular carcinomas with distant metastases was 75% and 62%, respectively, in the study of Canadian patients (5). In another study, the follicular histologic type of thyroid cancer also showed a significantly worse prognosis. The 5-year PTC survival rate with distant metastasis was 87.9% and 71.7% for FTC in the study of Korean patients (6). Furthermore, the survival rate was worse in cases of FTC with distant metastasis, while FTC without distant metastasis is a non-aggressive disease with a good prognosis (678910).
It is our opinion that predicting the occurrence of metastases and assessing distant metastases are very important in managing FTC patients. Therefore, we performed this study to evaluate the clinicopathologic factors associated with distant metastases and considered effective methods for managing FTC patients.
MATERIALS AND METHODS
A total of 5,522 thyroid carcinoma operations were performed between 2001 and 2017. In the same period, 149 primary FTC patients underwent operations, and in this study, we retrospectively reviewed the medical records of these patients.
The diagnosis of FTC was made by postoperative histologic confirmation of primary thyroid tissue or distant metastatic organ tissues. We diagnosed minimally invasive FTCs as having limited capsular and/or vascular invasion and categorized widely invasive FTCs as having widespread infiltration into adjacent thyroid tissue and/or blood vessels (>4 foci of vascular invasion) (3).
Initially, we performed a thyroid lobectomy and then a completion thyroidectomy after confirmation of the final diagnosis. Completion thyroidectomy was performed when the tumor size was >4 cm, if the FTC was widely invasive, or when multiplicity was confirmed. We could not perform a second operation if the patients refused to undergo another surgery. A total thyroidectomy was performed during the first operation in the case of accompanying bilateral indeterminate thyroid nodules, gross extra-thyroidal extension with soft tissue invasion, distant metastasis, or at the request of the patient.
Postoperative 131I radioactive iodine (RAI) therapy was applied to patients who had distant metastasis, tumors >4 cm, or widely invasive FTC. However, RAI therapy could not be performed if patients refused RAI therapy or if underlying diseases were severe.
Distant metastasis was verified using a 131I whole body scan (WBS), chest computed tomography (CT), bone scans, 18F-fluorodeoxyglucose positron emission tomography-CT (18FDG PET-CT), or histologic confirmation of metastatic lesions. Chest CTs, bone scans, and PET-CTs were used to determine the presence of distant metastasis in patients with thyroid stimulating hormone (TSH) suppression whose thyroglobulin (Tg) level was consistently increasing during the follow-up period. Synchronous distant metastasis was defined as a metastasis that was detected during the initial diagnosis or within 12 months of the initial operation. Metachronous distant metastasis was defined as a metastasis found ≥12 months after the initial operation. We analyzed synchronous and metachronous distant metastases together because of the small number of patients with metastases.
Our Institutional Review Board approved this retrospective study before the patient list was retrieved from the hospital database (GAIRB2018-429).
Statistical analysis was performed using IBM SPSS version 23.0 (SPSS Inc., Chicago, IL, USA). Pearson's χ2 test, Fisher's exact test, and the independent t-test were used to evaluate the significant differences between patients with and without distant metastasis. Logistic regression analyses were performed for multivariate analyses. P values <0.05 were considered statistically significant.
RESULTS
1. Clinicopathologic characteristics of all 149 FTC patients
The mean age at diagnosis was 44.8±14.4 years. The proportion of patients <45 years of age was 52.3% and <55 years of age was 75.8%. There were 15 cases of widely invasive FTCs. A total thyroidectomy was performed in 41.6% of the patients. There were three cases of distant recurrences (2.01%). The mean time to recurrence was 73.7±62.7 months (34–176). A total of 8 patients suffered from distant metastases (5.4%); 5 being synchronous and 3 metachronous. Metastatic lesions in synchronous metastases included 4 in bone and 1 in the lung and for metachronous metastases, there was 1 in bone and 2 in the lung. The mean serum Tg level in the first postoperative month was 54.6±93.8 ng/mL and the Tg-antibody (Tg-Ab) level was 4.6±14.9 U/mL. The mean serum Tg level in the third postoperative month was 11.8±51.4 ng/mL and the Tg-Ab level was 4.0±11.8 U/mL. The follow-up duration was 65.4±43.5 months (Table 1).
Table 1
Clinicopathologic characteristics of follicular thyroid cancer patients (n=149)

Values are presented as mean (range) or number (%).
ETE = extrathyroidal extension; RM = resection margin; TNM = tumor-node-metastasis; TT = total thyroidectomy; RAI = radioactive iodine.
![]()
2. Risk factor analysis for distant metastasis
Clinicopathologic factors related to distant metastasis are shown in Table 2. In univariate analysis, older patients had a tendency for distant metastasis with a 45-year cut-off age being statistically significant. Patients with distant metastasis were linked to vascular invasion and widely invasive FTC. Tg levels, which was checked in patients underwent total thyroidectomy in the first postoperative month, were higher in the distant metastasis group. Five patients with high Tg level had synchronous distant metastatic lesions. Multivariate analysis indicated that old age and vascular invasion were statistically significant factors for distant metastasis.
Table 2
Risk factors for distant metastasis

Values are presented as mean (range) or number (%).
CI = confidence interval; ETE = extrathyroidal extension; RM = resection margin; Tg = thyroglobulin; Tg-Ab = thyroglobulin-antibody; TT = total thyroidectomy; n.a. = not available.
*Checked in patients underwent TT in postoperative 1 month.
![]()
3. Eight patients with distant metastases
The characteristics of the 8 patients with distant metastases: 5 with synchronous and 3 with metachronous metastasis, are described in Table 3. While they all still had the disease at the time of their final visit, none had succumbed.
Table 3
Eight patients with distant metastasis
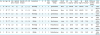
Op = operation; TT = total thyroidectomy; RL = right thyroid lobectomy; LL = left thyroid lobectomy; TNM = tumor-node-metastasis; ETE = extrathyroidal extension; RM = resection margin; RAI = radioactive iodine; Tg = thyroglobulin; Tg-Ab = thyroglobulin-antibody; ds = disease.
*Checked in patients underwent TT in postoperative 1 month; †Checked in patients underwent TT in postoperative 3 months.
![]()
Case 1
A femoral bone mass was discovered in a patient diagnosed with renal cell carcinoma. It was revealed to be a metastatic FTC. A total thyroidectomy and RAI therapy were performed. 131I WBS showed iodine uptake at the left scapula, left humeral shaft, around the anterior arc of left 3rd rib, sacrum, left ilium, and left femur. As bone metastasis progressed, despite two additional high-dose RAI therapies, radiation treatment (RT) was performed with the kinase inhibitor, lenvatinib.
Case 2
Thyroid cancer was found in a patient during a cervical (C) spine metastatic lesion work-up. A metastatic FTC was found on C5 during the spine biopsy and a total thyroidectomy and RAI therapy were performed. Since left scapular uptake was seen on 131I WBS, high-dose RAI therapy was repeated. Cervical bone RT was performed with the kinase inhibitor, sorafenib, due to uptake in multiple cervical vertebrae.
Case 3
A patient's first high dose RAI ablation showed multiple thoracic-lumbar (T-L) spine and rib metastases. As RAI avidity was seen on the 1st and 2nd 131I WBS, a 3rd RAI was planned.
Case 4
Right posterior 8th rib metastasis was found on a patient's first high-dose RAI ablation. As a left humeral uptake was observed during the 2nd RAI therapy, resection of the rib lesion was performed. A 3rd RAI therapy was scheduled.
Case 5
A patient had a large widely invasive FTC with gross muscle invasion. Although multiple pulmonary metastases were seen on her postoperative chest CT, RAI therapy could not be performed because of her psychiatric illness.
Case 6
After a patient underwent a right thyroid lobectomy during her first operation, a Tg level increase up to 240.78 ng/mL was detected on postoperative month 146 while under TSH suppression. As a chest CT showed multiple pulmonary metastatic nodules, completion thyroidectomy was performed. RAI therapy was planned.
Case 7
A patient's chest CT showed multiple pulmonary metastases in postoperative month 34. Tg levels rose to 34.47 ng/mL under TSH suppression. A completion thyroidectomy and two cycles of high-dose RAI therapy were performed. However, persistent lung metastases were seen on 131I WBS.
Case 8
A patient had a left thyroid lobectomy. Although a 1.8-cm widely invasive FTC was revealed on pathologic examination, completion thyroidectomy was not performed because of its small size and patient refusal. Follow-up PET-CT scans showed multiple skull, rib, T-L spine, ischium, and femoral bone metastases in postoperative month 41. Tg levels increased to 52.38 ng/mL. Completion thyroidectomy and 3 high doses of RAI therapy were performed. However, lesion progression into the thoracic spine and ischium were detected.
4. Clinicopathologic factors associated with vascular invasion
There were more male patients with vascular invasion than female patients (26.4% [14/53] vs. 12.5% [12/96], P=0.042). Patients with vascular invasion had larger tumors than patients without vascular invasion (4.18±1.65 cm vs. 3.04±1.71 cm, P<0.001). The proportion of tumors >4 cm was 49.1% (26/53) for patients with vascular invasion vs. 22.9% (22/96) for patients without vascular invasion (P=0.002). T stage was more advanced in patients with vascular invasion (P<0.001). Distant metastasis occurred more commonly in patients with vascular invasion than in those without vascular invasion (13.2% [7/53] vs. 1.0% [1/96], P=0.003). Synchronous distant metastasis was detected only in patients with vascular invasion (9.4% [5/53], P=0.005). However, metachronous distant metastasis occurred to the same extent in both groups (3.8% [2/53] vs. 1.0% [1/96], P=0.288).
DISCUSSION
In this study, old age and vascular invasion were significant factors for distant metastasis in FTC. Univariate analysis showed that age ≥45 years and widely invasive FTC were associated with distant metastasis. Tg levels in the first postoperative month in patients with a total thyroidectomy were associated with synchronous distant metastasis in univariate analysis.
According to FTC studies with distant metastasis, old age (≥45 years), larger tumor size (>4 cm), the presence of vascular invasion, extensive vascular invasion (≥4 foci), incomplete resections, lymph node metastasis, and loco-regional recurrence were significantly associated with distant metastases (9111213141516).
Survival rates of FTC patients with distant metastases were worse than for FTC patients without distant metastases. Synchronous distant metastasis was a strong prognostic factor for cause specific survival (CSS). Ten-year CSS rates of FTC patients with and without synchronous distant metastasis were 21% and 99%, respectively (10). Five-year CSS rates for synchronous distant metastasis groups, metachronous distant metastasis groups, and groups with no distant metastasis were 58%, 80%, and 100%, respectively, and 10-year CSS rates were 34%, 64%, and 100%, respectively. Groups with no distant metastasis showed significantly better survival than distant metastasis groups (P<0.001). Disease-specific deaths were found in 18% of patients in the distant metastasis group (7). Cumulative survival rate was significantly poorer in synchronous distant metastasis patients. Patients aged ≥45 or ≥50 years, tumor size >4 cm, combined capsular and vascular invasion, and of the male sex were linked to an increased risk of death from FTC (1718).
It would be advantageous to determine the adverse influence of synchronous or metachronous distant metastasis on the disease prognosis. Synchronous distant metastasis appears to show a more severe disease status in our study. Four out of five with synchronous distant metastasis had bone metastasis. Progression of the disease continued despite repeat RAI therapy and kinase inhibitor administration. In metachronous distant metastasis patients, only one suffered from bone metastasis, but also showed disease progression after RAI therapy. Because of the rarity of the disease, most of the previous studies did not distinguish between synchronous and metachronous distant metastasis. In one study, the authors claimed that these two groups had different disease entities, disease characteristics, and prognoses. Differentiated thyroid carcinoma patients presenting with initial distant metastasis appear to have relatively favorable outcomes compared with patients who developed distant metastasis after their initial treatment (19). However, this study dealt with all differentiated thyroid carcinomas including PTC. In one FTC study, synchronous and metachronous distant metastasis groups showed no significant difference in disease specific survival rates between the two groups (P=0.15) (7). There was no significant difference in mortality between those who presented with metastatic disease and those who developed metastasis during the follow-up period (33% vs. 50%, P=0.61) (20). We could not determine different adverse survival effects between synchronous and metachronous patients because all our patients survived.
In this study, bone metastasis occurred more frequently than lung metastasis. Interestingly, the synchronous distant metastasis group showed more frequent bone metastases while the metachronous distant metastasis group had more frequent lung metastases. In one study, 12 patients were diagnosed with metastatic disease at presentation, with bone being the most common site (75%). In the remaining eight cases, metastases developed at a median of 4.5 years (range: 2–8 years) after initial thyroid surgery, with lungs being the most common site (50%) (20). In another study, when 12 out of 132 patients (9%) presented with distant metastases, they were present in the bone (5 patients), lungs (4 patients), pituitary gland (1 patient), ovary (1 patient), and scalp (1 patient) (21).
FTC metastasizes to bone more frequently than PTC. Only lung metastasis was more frequent in PTC than in FTC (79% vs. 13%, P<0.001), and only bone metastasis was more frequent in FTC than in PTC (50% vs. 8%, P<0.001) (6). The incidence of bone metastasis from thyroid carcinomas in a study of all thyroid carcinomas was 5.0%; 45.4% had follicular, 36.3% had papillary, 6.8% had anaplastic, 6.8% had medullary, and 2 had Hürthle cell carcinomas (22).
Bone metastases can occur in vertebral bodies followed by the pelvis, femur, skull, and ribs. RAI therapy for patients with bone metastases is rarely curative, but some patients with RAI avid bone metastases may benefit from RAI therapy. Patients undergoing RAI therapy for bone metastases should also be considered for directed bone lesion therapy (23). This may include surgery, external beam RT, other focal treatment modalities, and systemic therapy with bone-directed agents. As bone metastases are less likely to concentrate radioiodine, and with high dose RAI therapy effective in only 55% of patients and remission in only 17% of patients, it is associated with a worse prognosis than pulmonary metastases. Patients are rarely cured, but they may experience a partial tumor response or disease stabilization with symptomatic improvement. External beam RT may be used for palliation (4). Therefore, detection of bone metastasis in FTC at diagnosis or during follow-up is very important when managing FTC patients.
The presence of vascular invasion was a significant factor for distant metastasis in this study and was an independent risk factor for distant metastasis when using multivariate analyses (1216). It was the most powerful predictor of distant metastasis after multivariate linear regression with old age (24). Patients who had vascular invasion with or without capsular invasion had a less favorable prognosis compared with patients who only had capsular invasion (21). According to the most recent World Health Organization (WHO) guidelines, extensive angioinvasion is associated with a worse prognosis although vascular invasion alone is not a component of diagnosis for widely invasive FTC (3). Vascular invasion and extensive vascular invasion were also emphasized in the 2015 American Thyroid Association (ATA) guidelines (23). The pathological parameters emphasized by the 2015 ATA guidelines include: aggressive histology, capsular invasion, the presence and extent of vascular invasion, extra-thyroidal extension, the number of lymph nodes with metastatic disease, and the size of metastatic foci. Therefore, the presence of vascular invasion is a very important prognostic factor for FTC. It is increasingly important for pathologists to report the presence and extent of vascular invasion to help clinicians understand their potential impact on patient management.
Three patients with metachronous distant metastasis underwent lobectomy during their first operation. However, the extent of the operation did not affect distant recurrence after analyzing metachronous distant metastasis in 144 cases (3.4% [3/87] in less than total thyroidectomy vs. 0.0% [0/57] in total thyroidectomy, P=0.278). In other studies, the surgical extent did not have an influence on the development of distant metastases during follow-up using multivariate analysis (1225).
This study had several limitations. First, the mean follow-up period (66 months) was relatively short. However, more than half had a follow-up period of over 60 months and it was over 36 months in 67% of the cases. Metachronous metastasis occurred in postoperative months 34, 41, and 146. Secondly, we had a small number of FTC patients resulting in a corresponding small number of distant metastasis cases. We could not analyze respective characteristics of synchronous and metachronous distant metastasis.
CONCLUSION
In FTC, old age and vascular invasion were significant factors for distant metastasis. Univariate analysis indicated that old age (especially, ≥45 years), vascular invasion, widely invasive FTC, and Tg in the first postoperative month (synchronous distant metastasis) were associated with distant metastasis. During the care of FTC patients, it is important to predict distant metastasis. Bone metastasis was frequent in FTC, and it was difficult to cure. Bone and lung metastatic work-ups should be performed routinely to discover distant metastatic lesions.
 XML Download
XML Download