

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recently, many investigators, notably Kehlet's group in Denmark, have devised the novel concept of “multimodal rehabilitation” or “fast-track surgery” for the management of surgical patients [1]. Fast-track surgery, also known as enhanced recovery after surgery (ERAS), aims to reduce surgical stress and enhance postoperative recovery by implementing evidence-based practices in the management of surgical patients. The hallmark of ERAS lies in its comprehensive nature that encompasses the entire process of perioperative management, including preoperative patient education, anesthesia and analgesia, operation, nutrition, and hospital discharge. Several studies have indicated that ERAS can reduce postoperative complications and hospital stay, particularly in patients undergoing colorectal surgery [23].
Previous studies about the efficacy of ERAS mostly originated from colorectal surgery, which was performed by the investigators who had initially developed the concept of ERAS [234]. More recently, several randomized trials and their systemic reviews have demonstrated the clinical benefits of ERAS in other abdominal procedures, including gastrectomy [56]. However, despite the clinical benefits of ERAS, its implementation in real practice has been relatively slow for several reasons, such as lack of convincing data, low level of awareness about ERAS, or limitations in institutional experience and systems [78].
Gastric cancer surgery is one of the most widely performed operations in South Korea, and the surgical technique is highly standardized among gastric surgeons. However, the protocol for perioperative management of gastric cancer surgery is still heterogeneous among various institutions. Currently, there are no nationwide data that reflect the current status of perioperative care for gastric cancer surgery in South Korea. Therefore, in an effort to standardize perioperative care, we carried out a nationwide survey to investigate the current status of implementation of ERAS protocols in gastric cancer surgery in South Korea.
MATERIALS AND METHODS
This survey was intended for gastric surgeons who specialize in gastric cancer surgery and are currently working at referral hospitals that maintain specialized upper gastrointestinal units. Using the membership database of the Korean Gastric Cancer Association and through an internet search, we found 161 gastric surgeons from 76 institutions who were eligible for this survey.
The questionnaire of this survey consisted of 24 questions, including 3 questions about personal information of the respondents and 2 questions about their knowledge level regarding ERAS; the remaining questions investigated the implementation of the ERAS protocols in the management of patients undergoing gastric cancer surgery (Supplementary Table 1).
The questionnaire was constructed in an electrical form and sent via email, from which the surgeons could directly enter the linked site and fill out the questionnaire on the internet. The survey was conducted for 2 months between January and February 2017. Of 161 surgeons to whom the survey was sent, 89 (55.3%) surgeons from 52 institutions finally responded. We analyzed the implementation of each ERAS protocol, dividing it into three phases: preoperative, intraoperative, and postoperative management.
RESULTS
The characteristics of the respondents are summarized in Table 1. The most common age group was 40–49 years (56.2%), followed by 50–59 years (20.2%), and 30–39 years (18.0%). About half the respondents (51.7%) were experienced in the field of gastric cancer surgery for ≥11 years, and 55.1% answered that they handle ≥100 cases of gastric cancer surgery per year. Regarding their understanding of ERAS, 58 (65.2%) surgeons responded that they were well versed with the concept and details of ERAS, and 45 (50.6%) of them were currently applying ERAS for their patients (Fig. 1). With regard to the types of operations, laparoscopic distal gastrectomy was the most common procedure (42 of 45 respondents) for which ERAS was being applied (Fig. 2).
Table 1
Characteristics of respondents

Fig. 1
Level of understanding about ERAS (A) and application of ERAS (B).
ERAS = enhanced recovery after surgery.

Fig. 2
Application of ERAS according to the type of operation.
ERAS = enhanced recovery after surgery.
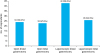
Table 2 represents the implementation of the ERAS protocols in the preoperative period. Most of the respondents (91.0%) answered they were providing preoperative education and counseling for patients. In total, 52 (58.4%) respondents did not perform routine preoperative mechanical bowel preparation, as recommended by the ERAS protocol. As for preoperative fasting, 61 (68.5%) respondents kept patients nil by mouth since the midnight before surgery. Only 9 (10.1%) respondents administered preoperative carbohydrate-rich drinks to patients.
Table 2
Implementation of ERAS protocols during preoperative period

Table 3 represents the implementation of the ERAS protocols in the intraoperative period. During the operation, 71 (79.8%) respondents ensured maintenance of intraoperative normothermia. Avoidance of routine use of abdominal drainage and nasogastric tube were followed by 28 (31.4%) and 68 (77.3%) respondents, respectively. For pain control, intravenous analgesia was the most common method (80.7%), while epidural anesthesia was performed by only 14 (15.9%) respondents. Thromboprophylaxis was performed by most surgeons (95.5%), and mechanical devices, such as an intermittent pneumatic compression device, were more frequently used than low-molecular-weight heparin. Intravenous goal-directed fluid management was performed by only four (4.5%) respondents.
Table 3
Implementation of ERAS protocols during operation

Table 4 represents the implementation of the ERAS protocols in the postoperative period. As for postoperative oral nutrition, only 13 (14.8%) respondents answered that they provided postoperative oral nutrition on postoperative day (POD) 1; 72 (80.9%) respondents were still using prolonged prophylactic antibiotics after surgery. Implementation of early active mobilization (94.4%) and early removal of urinary catheter (67.4%) were practiced relatively frequently. In total, 51 (57.3%) respondents answered that they were using discharge criteria to make the decision of discharge from the hospital. The most common average hospital stay was until POD 7 to POD 8, after both distal and total gastrectomy.
Table 4
Implementation of ERAS protocols during postoperative period

DISCUSSION
This is the first Korean nationwide survey that investigated the current status of perioperative care for gastric cancer surgery. We conducted this survey to collect baseline data that would help establish proper strategy for wide implementation of ERAS in clinical practice. We found that among the ERAS protocols, preoperative education, avoidance of preoperative fasting, maintenance of intraoperative normothermia, thromboprophylaxis, early active ambulation, and early removal of urinary catheter were relatively well adopted in perioperative care. However, other practices, such as avoidance of preoperative bowel preparation, provision of preoperative carbohydrate-rich drink, avoidance of routine abdominal drainage, epidural anesthesia, prophylactic antibiotics, postoperative high-oxygen therapy, early postoperative diet, restricted intravenous fluid administration, and application of discharge criteria were less well adopted. Therefore, possible solutions to overcome the obstacles that may undermine the implementation of ERAS should be considered. Finally, a standardized care protocol for gastric cancer surgery is urgently required to improve the quality of surgical care in South Korea.
ERAS is a multimodal care pathway designed to achieve early recovery in patients undergoing major surgery. The concept of ERAS involves a multidisciplinary team approach to resolve the issues that cause complications and delay recovery, by implementing scientific evidence-based care protocols and changes in management through interactive and ongoing audits [9]. With the increasing adoption of ERAS, updated and evidence-based guidelines by the ERAS study group are currently available for several abdominal procedures, including gastric surgery [10111213]. Recently, a few randomized trials have demonstrated improvement in the physical and psychological function of patients, and early hospital discharge by ERAS in the field of gastric surgery [1415].
Current ERAS guidelines for gastric cancer surgery were developed by the European ERAS study group in 2014 [13]. Although these guidelines are limited by the relatively low evidence in many recommendations, a consensus was reached on no preoperative bowel preparation, no use of nasogastric tube or abdominal drainage, no preoperative fasting and early postoperative oral nutrition, epidural analgesia, reduced intravenous fluid administration, and early removal of urinary catheter for gastric cancer surgery. Meanwhile, there is no consensus on the standard management for gastric cancer surgery in Asia. The Japanese treatment guidelines proposed some core items in the surgical management of gastric cancer, such as removal of nasogastric tube and abdominal drainage on POD 1, intravenous fluid administration until POD 5–7, initiation of oral nutrition on POD 2–4, removal of urinary catheter on POD 1, and discharge from the hospital between POD 8 and POD 14 [16]. However, these recommendations hardly reflect the recent advances in ERAS. Therefore, an evidence-based standard care protocol that can be widely applied should be developed for patients with gastric cancer in our region.
Despite the large evidence to support ERAS, its implementation in real practice has been relatively slow in the field of gastric surgery. Although most surgeons in this study are highly specialized in gastric surgery, our results showed that only 50% of gastric surgeons are actively applying ERAS for their patients. Further, on detailed investigation of the perioperative care of such patients, we observed that several evidence-based practices, such as avoidance of mechanical bowel preparation, administration of carbohydrate-rich drink, avoidance of abdominal drainage, epidural analgesia, postoperative high-oxygen therapy, single-dose prophylactic antibiotics, and early oral nutrition, were not implemented in real practice, with an implementation rate of only 10%–40%. This suggests that many traditional practices that were proven to be unnecessary or even harmful are still being performed in many institutions. This could be attributed to several reasons, such as the lack of awareness about ERAS, insufficient evidence for convincing surgeons, or the lack of belief that their own institution can actually perform ERAS. To improve the implementation of the ERAS principle in surgical care, more efforts should be made by academic societies to provide relevant updated information and education about ERAS to healthcare providers. In addition, finding convincing scientific evidence through a large multi-institutional randomized trial is important to encourage the implementation of ERAS in real practice.
The protocols of ERAS were founded based on previous studies that revisited the efficacy of traditional care, and it suggests that several elements in conventional care need to be changed or abandoned to accelerate postoperative recovery. For instance, several randomized controlled trials (RCTs) and meta-analyses show no convincing evidence to support the routine use of abdominal drainage or nasogastric tube for gastric surgery [171819]. Mechanical bowel preparation is not recommended, because it may cause dehydration and electrolyte imbalance [20]. Some RCTs reported that removal of the urinary catheter on POD 1 lowered infection rates without increasing re-catheterization rates [2122]. Although long-term preoperative fasting has been a routine practice to avoid pulmonary aspiration in elective surgery, a systematic review of clinical trials has found no evidence to support this [23]. Thus, current guidelines recommend intake of clear fluids up to 2 hours and solid food up to 6 hours before induction of anesthesia [24]. Further, provision of a clear carbohydrate-rich drink within 2 hours before anesthesia can reduce hunger, thirst, anxiety, and length of stay, as well as postoperative insulin resistance [25]. Preventing intraoperative hypothermia during the operation can reduce wound infections, cardiac complications, bleeding, and transfusion requirement [26]. Enforced bed rest not only increases insulin resistance and muscle loss but also decreases muscle strength, pulmonary function, and tissue oxygenation [27].
Early postoperative oral nutrition is one of the most essential components to accelerate postoperative recovery in ERAS. Traditional care regimens after major operations have usually included postoperative fasting until return of bowel movement. However, this can aggravate postoperative catabolism accompanied by excessive weight loss and wasting of skeletal muscle. Several RCTs and their meta-analyses have shown no clear advantage of postoperative fasting after elective gastrointestinal surgery [282930]. Early enteral feeding can reduce both the risk of any type of infection and the mean length of hospital stay, without an increased risk of complications from anastomosis. However, considering the risk of increased vomiting in patients fed early, multimodal anti-ileus therapy might be warranted [31].
A review of the data on excess perioperative fluid administration suggests that over-hydration may have deleterious effects on cardiac and pulmonary function, as well as on recovery of gastrointestinal motility, tissue oxygenation, wound healing, and coagulation [3233]. Several studies suggest that avoidance of fluid overload and provision of no more intravenous fluid than necessary to maintain fluid balance, often guided by body weight, may significantly reduce postoperative complications and shorten the length of hospital stay [3435]. In addition, some preliminary studies have shown that intraoperative fluid administration guided by transesophageal Doppler monitoring, called “goal-directed fluid therapy,” resulted in better ejection fraction, better oxygenation, and fewer postoperative complications [3637].
Several pieces of scientific evidence support the use of continuous epidural local anesthesia for postoperative analgesia [38]. However, this survey showed that only 16% of respondents used epidural anesthesia, and most of the institutions were using intravenous analgesia. Intravenous opioids do not provide the same analgesic effect as that provided by epidural anesthetic techniques, and have fewer beneficial effects on surgical stress responses [3940]. Surgeons should appreciate the role of epidural anesthesia not only in terms of pain control but also in attenuating postoperative surgical stress response by afferent nerve block.
This study has some limitations. First, of the 161 surgeons who were selected, 89 (55.3%) surgeons responded to the survey; thus, the response rate was relatively low. Second, this survey only included surgeons who specialized in gastric cancer surgery at referral hospitals. These limitations may restrict the representativeness of the real-world situation in Korea. Nevertheless, this survey demonstrated the problems of the large heterogeneity of surgical care for patients with gastric cancer in Korea in a comprehensive manner.
In conclusion, this survey showed that there is more room for improvement to standardize perioperative care and facilitate the implementation of ERAS in the field of gastric surgery in South Korea. Despite the evidence-based benefits of ERAS, its implementation in real practice was found to be relatively low in many institutions. Therefore, active organizational efforts are required to provide information and education about ERAS to healthcare providers to improve the implementation of the ERAS program.
 XML Download
XML Download