

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Panoramic radiography is used for many clinical purposes in dentistry, since it permits visualization of the upper and lower teeth, maxilla, mandible, and adjacent anatomical structures, such as the maxillary sinuses and hyoid bone. Radiopacities suggestive of soft tissue mineralization in adjacent anatomical structures are seen on 4%–19% of panoramic radiographs, and include salivary stones, mineralized lymph nodes, tonsiloliths, phleboliths, calcified carotid atherosclerotic plaques (CCAPs), and mineralized laryngeal cartilages (MLCs).123 The differential diagnosis is important because some of these conditions have a similar appearance, but only few require immediate intervention.4
CCAPs are caused by endothelial injury and appear as irregular and heterogeneous radiopaque images on panoramic radiographs, projected between the third and fourth cervical vertebrae inferior to the mandibular angle.4 CCAPs can cause ischemic stroke, and more commonly affect older male patients.5 Other risk factors include diabetes, hypertension, obesity, a sedentary lifestyle, and alcohol and tobacco consumption.5 If a CCAP is suspected, the patient should be referred to a physician for further evaluation.56
The laryngeal cartilages provide physical support to the larynx, and include the arytenoid, corniculate, cuneiform, cricoid, epiglottis, and thyroid cartilage. Mineralization of the superior horn of the thyroid cartilage appears as a vertical radiopacity measuring 4 mm in width and 15 mm in length, medial to the fourth cervical vertebra.4 The triticeous cartilages are other small cartilages located in the lateral thyrohyoid ligament that appear as radiopaque images measuring 2 to 4 mm in width and 7 to 9 mm in length when mineralized, also at the level of the fourth cervical vertebra.4
The radiographic appearance of CCAPs is quite similar to that of some MLCs, such as the thyroid and triticeous cartilages. Characteristics such as morphology and location may aid in the differential diagnosis, since MLCs are mostly limited to the greater hyoid horn and the thyroid cartilage, while CCAPs are usually not restricted to the hyoid level.7
As film-based radiographs are being replaced with digital radiographs, our experience has shown an increasing frequency of cervical radiopacities on digital panoramic radiographs. Studying a similar population that had been previously examined, Beckstrom et al.8 in 2007 likewise reported a higher prevalence of CCAPs on digital panoramic images than on film-based radiographs. In terms of the clinical relevance of this issue, we hypothesize that some of these radiopacities may correspond to medium-density tissues that are not necessarily mineralized, and appear to be more frequently detected on digital radiographs due to technical differences in image processing between analogue and digital technologies.
This study aimed to assess whether CCAPs and MLCs were more frequently detected on digital than on film-based radiographs using samples of 2 populations from distinct geographic regions.
Materials and Methods
This cross-sectional observational study was approved by the local Research Ethics Committee. The sample consisted of panoramic radiographs and reports obtained from 2 private oral radiology centers located in the northeast (C1) and southeast (C2) regions of Brazil, which had replaced film-based systems with digital systems 3 years before the study. Film-based radiographs were obtained using the Orthophos 3 machine (Sirona Dental Systems, Bensheim, Germany) and Kodak T-MAT 15-×30-cm films (Eastman Kodak, Rochester, NY, USA) processed in an A/T 2000 XR automatic film machine (Air Techniques, Melville, NY, USA) at both centers. Digital radiographs were acquired with the Kodak 8000 digital panoramic system (Eastman Kodak, Rochester, NY, USA) at C1 and with the Orthophos XG5 system (Sirona Dental Systems, Bensheim, Germany) at C2. The mean exposure parameters used for these machines are shown in Table 1.
Patients older than 30 years of both sexes, whose radiographs and reports were analyzed and issued by the same oral radiologist with more than 5 years of clinical experience, were included. Reports mentioning difficulties during patient positioning and radiographs with significant technical and processing errors were excluded from the study. The final sample consisted of 388 panoramic radiographs and 388 reports, corresponding to the calculated sample size. The reports and radiographs included in the study were assigned to 2 groups: film-based panoramic radiographs and their reports (n=188; group A), and digital panoramic radiographs and their reports (n=200; group D).
First, all reports were analyzed by an investigator who counted the presence or absence of CCAPs and MLCs in a 2×2 table. Prior to the study, radiographs from group A were routinely digitized at C1 and C2 using an HP Scanjet G4050 scanner with a transparent materials adapter (Hewlett Packard Enterprise, San José, CA, USA) at 300 DPI resolution and saved as TIFF files.
The digitized radiographs from groups A and D were assessed on a desktop computer (Optiplex 790; Dell Inc., Round Rock, TX, USA) on a 19″ monitor with a standard resolution of 1366×768 (E1916H; Dell Inc., Round Rock, TX, USA), using the Windows imaging viewer and the zoom tool. Two oral radiologists with 10 to 20 years of experience with panoramic radiographs assessed the images in a silent room under dim lighting conditions. Without prior knowledge of the content of the reports, the oral radiologists assessed all panoramic radiographs to ensure the consistency of the data collected in the reports. They also analyzed the radiographic features of CCAPs and MLCs and indicated their most likely diagnostic impression (i.e., whether radiopacities were suggestive of CCAP, mineralized triticeous cartilage, or mineralized superior horn of the thyroid cartilage) according to the criteria described by Carter et al. (2000).4 The pooled data were analyzed according to population (C1 vs. C2), group (A vs. D), side (right vs. left vs. both), sex (male vs. female), and age.
Data were tabulated in Microsoft Excel (Microsoft Corp., Redmond, WA, USA) spreadsheets and analyzed using the Fisher exact test; odds ratios were also calculated, adopting a significance level of 1%. The descriptive analysis included the absolute and relative frequency, mean, and standard deviation. The null hypothesis was that CCAP/MLC detection would not differ between groups A and D.
Results
Table 2 shows the age and sex of the patients in the sample. There was a predominance of female patients at both centers, and the patients' age ranged from 31 to 87 years. The mean age of groups A and D was similar at C2, but group A had a lower mean age and a smaller standard deviation than group D at C1.
All reports matched the opinion of the oral radiologists when the radiographs were assessed for the presence or absence of CCAPs and MLCs. Table 3 shows the frequencies of CCAPs and MLCs. At C1, CCAPs and MLCs were detected on 17 panoramic radiographs from group D, but on none of the radiographs from group A. At C2, CCAPs and MLCs were detected on 30 radiographs from group D, but on only 9 radiographs from group A. Therefore, CCAPs and MLCs were more frequently detected on digital panoramic radiographs at both C1 and C2 (P<0.01). The odds ratio could only be calculated for C2 because of the absence of positive cases in group A at C1. The detection of CCAPs and MLCs was 4.33 times more frequent in group D than in group A at C2.
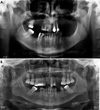
Table 4 shows the pooled data of positive cases. The frequency of CCAPs was the same in both populations. CCAPs were more frequent on the right side and in male patients, and the mean age of patients with CCAPs was 54.1 years. Mineralized triticeous cartilage was more frequently detected at C2 and in female patients, and the mean age of patients with mineralized triticeous cartilage was 53.5 years. Three cases were found on the left side, and the other 3 on both sides. Mineralized superior horn of the thyroid cartilage was also more prevalent at C2, on both sides, and in female patients; the mean age of the affected patients was 50.1 years. The frequency of all types of radiopacities was higher in group D than in group A. Figure 1 shows examples of radiopacities suggestive of mineralized superior horn of the thyroid cartilage on film-based and digital panoramic radiographs. Radiopacities seemed to be more evident on digital images than on film-based radiographs.
Discussion
Our hypothesis was confirmed, since statistically significant differences in CCAP/MLC frequencies were found between groups A and D at both centers (P<0.01). A calculation of the odds ratio revealed that 4 times more cervical radiopacities were detected on digital panoramic radiographs than on film-based images. This ratio could only be calculated for C2, since no positive cases were found in group A at C1. Interestingly, at C1, the patients in group A were younger than those in group D. Our hypothesis arose from our daily practice in oral radiology and imaging reports, which gave us the impression that we were seeing more images consistent with CCAPs/MLCs on digital radiographs. Since no studies on the subject were available in the literature, we decided to evaluate whether our impression was correct. Two oral radiology centers located in distinct geographic regions were included in the study. Film-based panoramic radiographs were compared to digital radiographs obtained at the same center to rule out the influence of local factors on the variables studied.
CCAPs and MLCs were counted together for statistical purposes because most of the reports did not describe whether the radiopacity was a CCAP or MLC. Furthermore, the radiographic appearance of CCAPs and MLCs is very similar, and both are included in the differential diagnosis.910 Two oral radiologists (independent examiners) also assessed all panoramic radiographs, and the most likely diagnostic impression was considered to generate the pooled data shown in Table 4.
Considering all 56 radiopacities found in the study, 8 were suggestive of CCAP (14.3%), 6 were suggestive of mineralized triticeous cartilages (10.7%), and 42 were suggestive of mineralized superior horn of the thyroid cartilage (75.0%). Most patients with CCAP were male (87.5%), in agreement with Friedlander et al. (2005)5, but we found a lower mean age than those authors. This difference is probably due to the fact that our patients were older than 30 years, while the patients analyzed by Friedlander et al. were older than 50 years. MLCs were more prevalent in female patients (72.9%); the mean age was 53.5 years for mineralized triticeous cartilage and 50.1 years for mineralized superior horn of the thyroid cartilage. Although the occurrence of mineralization tends to increase with age, the degree of mineralization and chronological age are not well correlated.4 In the study of Claassen et al. (2014)11, both male and female subjects in the fourth and fifth decades of life were more likely to exhibit mineralized superior horn of the thyroid cartilage, which is in accordance with the respective mean age found in the present study. However, in our study, more female patients had mineralized superior horn of the thyroid cartilage, whereas mineralized thyroid cartilage was more frequent among men in the study of Claassen et al. (2014).11 Regarding location, most CCAPs were seen on the right side (62.5%), while mineralized superior horn of the thyroid cartilage was found on both sides (69.0%).
A modified anteroposterior radiograph of the skull can be used to differentiate between CCAP and MLC.6 However, due the limitations of that modality, ultrasound examination with a carotid echo-Doppler is recommended for diagnosis and treatment planning in cases of CCAP.5 In our clinical practice, we usually refer patients for a medical examination when CCAPs are seen on imaging. Conversely, since MLCs are physiological, there are no associated risk factors or clinical implications.7 Panoramic radiography, which is used for many purposes in clinical practice, may be relevant for the early diagnosis of CCAP.
One may hypothesize that the more frequent detection of calcifications in group D may have been due to lifestyle changes among the population that would increase the prevalence of CCAPs. However, this explanation cannot be accepted, because the radiographs of group A were acquired only 1 to 3 years before those of group D, a period that is not sufficient for lifestyle changes to influence the prevalence of CCAPs. We therefore believe that the present results can be explained by a reduction in the energy parameters (mA and kVp) employed in digital systems. In addition, the possibility to adjust brightness and contrast in the images may enable the visualization of medium-density anatomical structures, such as cartilages. Therefore, it is possible that some of the radiopacities found on digital panoramic radiographs correspond to normal cartilages that appeared as radiopaque areas due to the reduction in energy parameters and image adjustment. We believe that medium- density tissues, which used to be burned out by the higher energy parameters applied to film-based radiographs and the low resistance offered by the cervical region, are now being seen in digital radiographs due to the factors mentioned above. Ultrasound studies are recommended to confirm this hypothesis, since ultrasonography is a noninvasive method that uses non-ionizing radiation.
The major limitations of this study are the different devices used and the small number of oral radiology centers included. It was difficult to gather a sample of film-based radiographs from centers that have recently switched to a digital system. The energy factors were also different, since they varied according to the patient's physical characteristics, but this represents actual clinical practice. However, we do not believe that the digitization of film-based panoramic radiographs influenced our results, since the opinions of the observers who evaluated the digitized images from the database were the same as those presented in the reports, which were issued by professionals that had analyzed the physical version of the film-based radiographs.
In conclusion, CCAPs and/or MLCs were more frequently detected on digital images than on film-based panoramic radiographs. Further studies are encouraged to determine whether such radiopacities do indeed correspond to mineralized structures, rather than medium-density anatomical structures such as cartilages.




 XML Download
XML Download