

 PDF
PDF ePub
ePub Citation
Citation Print
Print


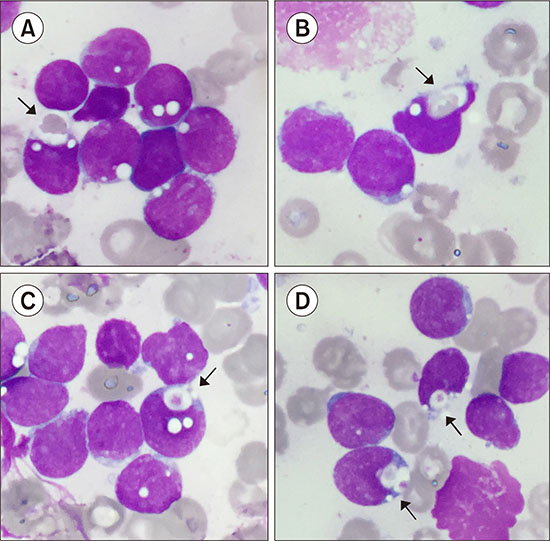
A 4-year-old boy presented with spontaneous hematomas, lower limb pain, fever, and hepatosplenomegaly. A complete blood count revealed pancytopenia (white blood cells, 7.6×109/L; neutrophils, 0.46×109/L; hemoglobin, 6.7 g/dL; platelets, 85×109/L). The peripheral blood smear examination showed 54% medium-sized blasts, with a high nucleus-to-cytoplasm ratio, round or oval nuclei, fine chromatin, and basophilic cytoplasm containing many vacuoles. The bone marrow (BM) was infiltrated by 98% of blasts of the same morphology. Interestingly, we frequently observed thrombophagocytosis and erythrophagocytosis by blasts in the BM (composite image of BM smear, May-Grunwald-Giemsa staining, ×1,000; A, B: erythrophagocytosis. C, D: thrombophagocytosis). Immunophenotyping analysis showed positivity for cluster of differentiation (CD) 34, CD19, cCD79a, and CD10; aberrant positivity for CD33; and negativity for CD20, c-µ, and sIgM. These confirmed the diagnosis of B-cell precursor acute lymphoblastic leukemia (ALL), B-II type common, according to the European Group for the immunological classification of leukemias. A normal 46,XY[20] karyotype was observed, but fluorescence in situ hybridization analysis revealed a cryptic translocation t(12;21)(p13;q22) with ETV6-RUNX1 fusion. Hemophagocytosis by blasts has been reported mainly in acute myeloid leukemia, especially associated with t(8;16)(p11;p13); KAT6A-CREBBP. In ALL, this phenomenon is very rare and is not associated with specific cytogenetic or molecular anomalies.
 XML Download
XML Download