

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic Obstructive Pulmonary Disease (COPD) was a preventable and treatable disease with some significant extra pulmonary effects that may contribute to the severity in individual patients. Its pulmonary component was characterized by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases.1 Recently, 2012 Global Burden of Disease study revisited most previous worldwide estimates on respiratory diseases, for example, COPD, asthma, sleep related disorders, lower respiratory infections, lung cancer and tuberculosis. The estimate number of 328 million people had COPD worldwide(men, 180 million; women, 150 million).1 COPD was also estimated to be the seventh and tenth leading cause of disability in countries of high income and in those of low or middle income, respectively.2
As we had known, though with decreasing tobacco use,3 the prevalence of COPD should also be decreasing. In Spain, the prevalence of airflow obstruction was 50% decreased in 10 years, that is from 9.1% in 1997 to 4.5% in 2007.4 The prevalence of self-reported diagnosed COPD was analyzed by comparing data from the 1988–1994 and 2007–2010 National Health and Nutrition Examination Survey (NHANES). Age-standardized estimated prevalence of doctor-diagnosed chronic bronchitis and emphysema decreased significantly in 2007–2010 overall and specifically among certain age groups and races.5 Another study in Finland, from the population surveys repeated every 5 years between 1982 and 2007, found that the prevalence of chronic bronchitis decreased from 19% in 1982 to 13% in 2007 in men, and from 13% to 11% in women.6 Overall, the prevalence of COPD and associated symptoms seems to be decreasing over the last decades.
In spite of decreasing prevalence, the economic burden of COPD kept growing. In Korea, medical costs per person were USD 2,803 ± 3,865 in 2009 according to the Korean Health Insurance Review and Assessment Service data.7 In addition, the numbers of patients with severe COPD increased rapidly in Korea and showed a high prevalence of comorbid disease. The total medical costs were over three times higher in patients with high-grade COPD compared with those without it (USD 3,744 vs. USD 1,183; P < 0.001). Medication costs comprised the largest portion of medical cost, but most impact came from hospitalization and exacerbation in both groups of patients.8
COPD was an age-related condition, and several evidences suggested a relationship with a rapidly increasing aging.9 COPD morbidity and mortality were stiffly increasing, especially in countries with aging society. Indeed, there was evidence that aging can serve as an underlying mechanism of COPD.10 Also, smoking, which was the most common cause of COPD, was also responsible for the systemic manifestations of the disease, independently from the lung function alterations.101112 Clinically, smoking was attributed as an age-accelerating factor.13 Various COPD associated symptoms (air-flow limitation and loss of parenchymal tissue) were also part of aging of lung.14 Relative risks for COPD patients with smoking according to gender and age varied from 2–32 compared with non-smokers.12 And almost COPD patients (80%–90%) had been smoked and 90% of care cost of COPD of men is due to smoking.15
The purpose of this study was to analyze the effect of aging on the occurrence of cigarette smoking induced COPD. For this analysis, we evaluated smoking status by a lifestyle intervention program and measured the occurrence of COPD by the Korea National Health and Nutrition Examination Survey (KNHANES) from 2005 to 2015.
METHODS
Study population
In this study, we used data from the 3–6th KNHANES from 2005 to 2015. We targeted 17,398 COPD patients who got lung function test. And According to Global Initiative for Chronic Obstructive Lung Disease (GOLD), we selected 1,427 patients who could get information regarding severity and smoking behavior.
COPD was defined by the International Classification of Diseases, 10th Revision classifications.8 J44 code of COPD included COPD with acute lower respiratory infection (J44.0), COPD with (acute) exacerbation (J44.1) and unspecified COPD (J44.9). For classification of COPD severity, we applied GOLD criteria.16 For calculating GOLD, we needed forced expiratory volume in one second (FEV1) and forced vital capacity (FVC). According to the KNHANES, we could get the information. Using restrictive spirometry, we calculated the FEV1/FVC ratio. GOLD 1 was mild status with FEV1/FVC was under 0.7 and FEV1 is over 80% predicted. GOLD 2 was moderate status with FEV1/FVC was under 0.7 and FEV1 was between 50% and 80% predicted. GOLD 3 was severe status with FEV1/FVC was under 0.7 and FEV1 was between 30% and 50% predicted. GOLD 4 was very severe status. The FEV1/FVC was under 0.7 and FEV1 was under 30% or under 50% predicted with chronic respiratory failure.
Target population were divided into four categories: young age and short smoking duration, young age and long smoking duration; old age short duration; old age long duration. For grouping four categories, sample age and duration were considered 2 categories (aged less than 50 and aged more 60, smoking duration less than 5 years and more than 20 years) in order to contrast maximize (Table 1). The reason why we used 60 years old as a cut-off for old is that almost all public policies used the 60 as a standard age for the old. In case of smoking duration, over 20 years smoking duration is significantly risky to COPD patients compare to under 10 years duration.1 Finally, total study population is 627 COPD patients who can be included four categories.
Table 1
Definition of the categories (n = 627)

| Smoking duration, yr | Age, yr | |
|---|---|---|
| < 50, No. (%) | > 60, No. (%) | |
| < 5 | 138 (22.0) | 198 (31.6) |
| > 20 | 85 (13.6) | 206 (32.9) |
![]()
For control variables, body weight and height were assessed to calculate body mass index (BMI). The number of pack-years smoked (the number of cigarettes per day divided by 20 multiplied by the number of years smoked) and smoking status (current and ex-smoker) were recorded.
Statistical analysis
The purpose of this study was to find the independent and combined effects of aging and smoking behavior on COPD patients. Especially, this study used multivariate model that specified that age, smoking duration and interaction of them and level of COPD severity. Multiple logistic regression analyses were used to test the models including interaction effect in which the independent variables were age, gender, smoking habits. Odds ratio (OR) are reported with 95% confidence intervals (CIs). A backwards stepwise approach was undertaken with the criteria for variables to be considered significance. SPSS version 18.0 (IBM Corp., Armonk, NY, USA) was used for the data analysis and a P value < 0.05 was considered significantly different.
RESULTS
Descriptive statistics for the sample are provided in Table 2. The social and clinical characteristics of these 627 subjects are described in Table 2. The mean age was 61.9 and standard deviation was 11.91. The youngest patient's age was 41 and the oldest was 87 years old. Men COPD patients (488 patients) were 3.5 times of women (139 patients). In case of BMI, averaged BMI was 27.4 (± 4.1) and the range of BMI was from 21.1 to 30.9. According to GOLD levels, middle level's severity patients (level II and III) were more than severe patients (level IV). In smoking habits, the current smokers was 298 persons, less than ex-smokers (n = 329). The length of smoking duration is about 13 years average (12.9 years) and the range was 0.8 to 42.7 years.
Table 2
Descriptive statistics (n = 627)
SD = standard deviation, BMI = body mass index, GOLD = global initiative for chronic obstructive lung disease, FEV1 = forced expiratory volume in one second, FEV1/FVC = forced expiratory volume in one second/forced vital capacity (Tiffeneau indexa).
aTiffeneau index, calculated ratio which represents the proportion of a patient vital capacity that they are able to expire in the first second of forced expiration.
![]()
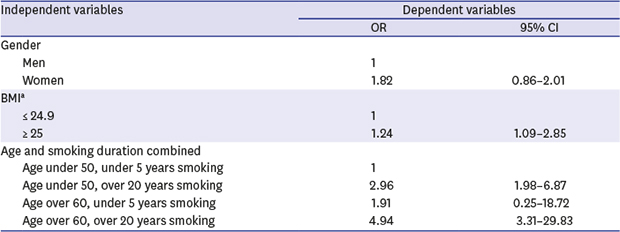
We examined weather the aging, smoking duration and their interaction displayed relations to COPD severity or not by multiple logistic regression analysis. Control variables included in multivariate model were gender and BMI. Gender was not significantly associated COPD severity, while BMI was significantly related with COPD severity. In comparison with under 50 years with under 5 years smoking, the same age group with over 20 years smoking group yielded an OR of 2.96 significantly. But the aging effect was stronger among longer smoking duration group, and the OR for COPD was 2.96 (95% CI, 1.98–6.87) vs. 4.94 (95% CI, 3.31–29.83). The age was found to have a significant positive main effects. Thus, with increasing age, the severity of COPD was increased. Duration of smoking was also positively related to COPD severity. As patients smoked 20 years more, they experienced malfunction of lung and severe COPD. The combined effect of smoking duration and age were found highly significant among subjects over 20 years aged smoking group for COPD severity (Table 3).
Table 3
Risk factors for COPD according to GOLD

COPD = chronic obstructive pulmonary disease, GOLD = global initiative for chronic obstructive lung disease, OR = odds ratio, CI = confidence interval, BMI = body mass index.
aBMI, calculated as the weight in kilograms divided by height in meters squared.
![]()
Interaction effects of age and smoking duration were detected in relation to the severity of COPD. A positive interaction effect was found significantly. Thus while subjects experienced severe COPD as they lived smoking longer, this effect was aggravated when aging was combined.
DISCUSSION
For more deepen knowledge of the COPD, we calculated risk combination of increasing age and smoking habit. On previous study, they reported the prevalence of COPD and its risk factor in the same aged general population.8 But there was not the interaction between risk factors. The trend among smokers with COPD, compared to non-smoker COPD patients, to develop COPD severity with time passed. Because they were more sensitive to air condition or environmental status. 116 So to grasp the actual effects of interaction between risk factors could be useful indicators for prevention COPD patients or slow down the COPD processing.
Our data show that COPD patients exhibit aging and smoking duration related severity. These two characteristics were significantly effected on the lung function of COPD patients. Especially, the smoking duration is exaggerated in the presence of old age for older COPD patients.
Regarding disease severity, the prevalence of mild COPD (GOLD I) for 10 years was about 30% (3% per year) and moderate and severe COPD (GOLD II and III vs. IV) was 6.0% and 0.8%, respectively. This numbers were similar to the 6.9% according to GOLD found in the US NHANES III survey.17
The interaction effect of aging and smoking is dominated determinant of COPD severity. The mild smoker with under 50 years old COPD patients were in less severe COPD status. The strong combined effect between smoking duration and COPD severity was consistent with several previous studies showing that aging and smoking habit are strongly associated with the COPD.9101112 Especially, age-related physiological and biological abnormalities happened in COPD patients with smoking.18 The 2013 World Health Assembly called on governments to reduce smoking by a third by 2025, which could avoid more than 200 million mortality during the remainder of the century.19 However few studies have assessed the severity of COPD according to interaction between aging and smoking behaviors. In particular, a study reported that life style intervention improved COPD risk factor status312 and aging related abnormalities in COPD patients were also found for identifying smokers at high risk for aging related systemic manifestation.20
General study reported that a higher prevalence of COPD among men.2122 But, in our study, the gender difference was not significant not only single gender effect but also by smoking and aging effect. Further study was needed to find out the gender effects regarding aging and smoking habits. In addition, KNHANES was self-reported questionnaires so subjects could answer with biased. So when we implemented the results, we needed more careful.
Globally, COPD has been established as significant contributors to the burden of disease.23 And cigarette smoke remains the most important cause of COPD. Especially, COPD mortality due to smoking in high-income countries was 73%.2 This relation is derived highly by gene, so not all smokers get COPD but high portion of smokers have been noted to develop COPD.2425 Lung function started to decrease in the third and fourth decade of life, naturally.26 But some researchers reported that the reason for the increasing prevalence of COPD recently is the population changing to aging society.27 Generally, aging is associated strongly with diseases and factors that allow patients to survive into old age, such as enhanced interventions for acute diseases will induced in higher COPD prevalence, morbidity and mortality. Although smoking is a powerful risk factor for COPD, the relation between changing smoking prevalence in a population and disease outcome is more complex.28 So the interaction between aging and smoking is hard to judge certainly. But the aging of the global population, COPD is major chronic disease which will keep becoming more frequently. So it will be best managed in a comprehensive way with attention to effectiveness intervention.29
COPD gets importance more and more internationally. To know the risk factor of COPD quantitatively and to find out the interaction between task factors could result in better preventive intervention for COPD patients.
 XML Download
XML Download