

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Injury has long been regarded as a form of preventable disease. Since the late 1940's, efforts have been made to promote better public health management of injury, with epidemiologic data used to assess both the magnitude and long-term outcomes of various injuries and along with the potential benefits of injury prevention.12 The Global Burden of Diseases (GBD) team reported that the total burden of injury worldwide was estimated at 259,714,500 disability-adjusted life years (DALYs) (3,457.3 per 100,000) in 2016.3 This accounted for 10.61% of the global burden of all diseases.3 The 2016 total injury DALYs were 3,369 higher than in 2015.4 As the above research suggests, injury remains an important public health problem worldwide, despite it being preventable.
In Korea, the burden of disease from injury was 1,581,072 DALYs (3,170 per 100,000 people) in 2010.5 In the GBD 2010 country profile, the total injury burden of Korea was 1,286,733 DALYs,6 an estimated 18.6% lower than that seen in the Korea Burden of Disease (KDB) study. However, because the GBD used a prevalence-based approach to calculate years lived with disability (YLD), whereas the Korea National Burden of Disease (KNBD) study calculated YLD using an incidence-based approach, the extent to which these studies can be directly compared is limited.
DALY is calculated as the sum of years of life lost (YLL) and YLD.7 The difference in the YLL calculation between the two methods is that incidence-based approach adjusts outcomes based on age weighting and discount rate, while a prevalence-based approach does not.89 The prevalence-based approach estimates all health-related losses over the course of a year, whereas the incidence-based approach captures the burden of disease in new diagnostic cases.10 Traditionally, the burden of disease has been estimated by an incidence-based method for forward-looking or cohort-based approaches; however, since the first GBD study in 2010, the prevalence-based approach has become far more widespread as a means of estimating GBD,6 although no prevalence-based studies have been performed in Korea.
The goal of this study was to understand the differences in national burden of injury outcomes when calculated using either an incidence-based or prevalence-based approach. Outcomes were assessed in terms of injury mechanism and demographic characteristics, with the implications of these findings considered in the context of public health interventions.
METHODS
Study design
This cross-sectional study analyzed morbidity and mortality data related to injuries that occurred in Korea in 2014. We used injury-related deaths and hospital admissions data for 2014, because that was the most up-to-date hospital admission data at the time of analysis. We also used the 2014 mortality data to calculate the life expectancies, in turn used to evaluate the YLL. Ultimately, the burden of injuries was estimated for 2014 in terms of DALY.
Participants
The study population consists of all patients who were admitted to hospital due to an injury or died from external causes in 2014. The mortality and hospital admission data sources for this study include diagnostic codes of the 5th Korean Classification of Diseases (KCD-6) based on the 10th revision of the International Classification of Disease (ICD-10). The participants were categorized according to the mechanism of injury, based on the classifications in the KNDB 2015 study, as follows.11 Transportation injury: road injuries (ICD-10 V01-V04, V06, V09, V10-V19, V20–V29, Y85.0, V30–V79, V87.2-V87.3, V80, V82) and injuries caused by an agricultural vehicle (V05, V81, V83-V86, V88.2, V88.3, V91, V93-V98); unintentional injuries other than transport injuries: falls (W00-W19), drowning (V90, V92, W65-W74), fire, heat and hot substances (X00-X19), poisoning (X46-X47, X48, X40, X43-X44), exposure to mechanical forces (W32-W34, W24-W31, W45-W46), adverse effects of medical treatment (Y40-Y84, Y88), and animal contact-related (X20-X29, W53-W64); overexertion and strenuous movements (W21, W39, W44, W49-W52, W75-W99, X50-X58); self-harm and interpersonal violence: self-harm (X70, X76-X77, X72-X74, X68, X71, X75, X78-X83, X60-X67, X69) and interpersonal violence (X93-X95, X99, X85-X92, X96-X98, Y00-Y08); forces of nature, war and legal intervention: exposure to forces of nature (X30-X39), and collective violence and legal intervention (Y36, Y89.1, Y35, Y89.0). The cause disability weight (DW) for estimating incidence-based YLDs and health status DW for estimating prevalence-based YLDs were based on previously reported values.1213 Regarding morbidity data, we excluded cases that occurred during the preceding year from the incidence analysis.
Data source and measurement
For this study, we used the 2014 Korean national database of mortality- and morbidity-related injuries. The 10th Korean National Hospital Discharge Survey (KNHDS) data from the Korea Centers for Disease Control and Prevention (KCDC) were used to calculate both incidence- and prevalence-based YLD. Cause of death statistics from Statistics Korea were used to estimate YLLs.
The KNHDS has been conducted every year since 2004. The survey sampling is based on clusters of hospitals stratified by geographic location and number of beds. The KNHDS data included approximately 9% of all discharged patients, who were sampled randomly from among 170 sample hospitals with more than 100 beds. These medical records data contained clinical information such as patient age, gender, area of residence (zip code), type of insurance cover, and diagnostic code(s). A physician collected additional data on injury mechanisms. Details of the survey sampling design have been reported.14 Weighting of the sample survey was applied when estimating the incidence and prevalence of injury in the years lost to disability (YLD) calculations
Mortality data from January 1 to December 31, 2014 were obtained from the mortality records of the Korea National Statistical Office. We estimated the incidence- and prevalence-based YLL from the mortality data. The incidence- and prevalence-based YLD were calculated from morbidity data. As the final index of injury burden, the incidence- and prevalence-based DALY was calculated as the sum of YLL and YLD.
Statistical analysis
Incidence-based YLLs were calculated based on the 2014 mortality and standard life-expectancy data using the same methodology as that used in the 2012 KNBD study.11 In the prevalence-based YLLs, age correction and discount rate were not applied. Incidence-based YLDs were calculated by multiplying the injury incidences by their mean duration and cause DW using Dismod II. We computed prevalence-based YLDs by multiplying the prevalence sequela and health status, calculated as the average of the various DW of health status. DALYs were calculated as the sum of YLLs and YLDs and presented as a number and rate per 100,000 in the registered population. Data analyses were performed using SAS version 9.4 (SAS institutes, Cary, NC, USA) and Dismod II version 1.04 (World Health Organization [WHO], Geneva, Switzerland).
RESULTS
Table 1 presents the demographic characteristics of the study subjects. The weighted frequency for morbidity was 1,026,000 persons. There were 24,288 deaths from injury in 2014. The injury morbidity rate was about 10% higher in males (55.7%) than in females (44.3%); the death rate was more than twice as high in males. Injuries were most frequent in the 40–50-year age group in both genders. Regarding injury mechanisms, unintentional injuries other than traffic injuries had the highest morbidity rate (61.4%). Regarding the mortality data, self-harm and interpersonal violence were the most common causes of death (58.8%).
Table 1
Demographic characteristics of injured persons according to Korean morbidity and mortality

![]()
Table 2 shows the injury burden of Korea in 2014. Prevalence-based YLLs were almost 2 times higher than that of incidence-based YLLs; however, incidence-based YLDs (1,003,981) were substantially higher than that of prevalence-based YLDs (655,138). The total incidence-based injury burden was estimated at 1,544,467 DALYs, compared with 1,670,229 DALYs using the prevalence-based method. The prevalence-based DALY rate was higher than that of the DALY incidence-based rate by 248 per 100,000. For all indicators, the injury burden of males was higher than that of females.
Table 2
Estimated burden of injuries by gender and age in Korea
Rate for DALYs: per 100,000 persons.
YLL = years of life lost, YLD = years lived with disability, DALY = disability-adjusted life year.
![]()
Next, injury burden was subdivided based on mechanism of injury into three levels (higher, middle and lower levels) using the criteria for injury classification set forth by Lee et al.5 (Table 3). Injuries were classified into 4 major categories: transport injuries; unintentional injuries other than transport injuries; self-harm and interpersonal violence; and forces of nature, war, and legal intervention. Each of the higher classifications was further divided into sub levels.
Table 3
Estimated burden of injuries by mechanisms in Korea

Rate for DALYs: per 100,000 persons.
YLL = years of life lost, YLD = years lived with disability, DALY = disability-adjusted life year.
![]()
Among the higher-level classifications, the DALY for unintentional injuries other than transport injury was most common, accounting for 37.7% of the total injury burden, followed by self-harm and interpersonal violence (34.7%), transport injuries (27.1%), and forces of nature, war and legal intervention (0.5%) using the prevalence-based approach. Using the incidence-based approach, the top five middle-level classification groups were road injuries (477,984 DALYs), falls (431,999), self-harm (271,463), overexertion and strenuous movements (98,690), and exposure to mechanical forces (89,013). The most common prevalence-based DALYs were self-harm (DALYs, 473,628), road injuries (433,274), falls (316,894), overexertion and strenuous movements (146,299), and interpersonal violence (106,248). Among high-level classification groups, the mortality index (YLL) was highest in the self-harm and interpersonal violence group, accounting for more than double the YLL of the second highest ranking, unintentional injuries other than transport injuries, as determined using both the incidence-based and prevalence-based approaches. For YLD, unintentional injuries other than transport injuries ranked highest in both methods. For the majority of injury mechanisms, the incidence-based YLD was higher than that observed using the prevalence-based method, with the exception of pedal cycle vehicles and adverse effects of medical treatment, which were higher in prevalence-based results.
The gender difference between male and female injury burden is shown in Fig. 1. The top 5 DALY rankings were all higher for males compared with females. Self-harm was the highest DALY group for both males and females in prevalence-based results, compared with incidence-based results, which identified road injury as the most significant injury classification for both genders. For males, falls and self-harm were the second and third ranking groups, respectively, in incidence-based results, while road injury was second and falls third in the prevalence-based results. For females, falls were the second and road injury the third most common causes of injury in the prevalence-based results, compared with falls and self-harm in the incidence-based results. Interpersonal violence and drowning were seven times higher for males compared with females according to the prevalence-based method.

Fig. 2 presents the distribution of injury burden by mechanism and age group. Incidence- and prevalence-based total injury burden by age distribution produced an “inverse-v-shape” (Fig. 2A). By contrast, DALY rates showed a noticeably different pattern when examined on a per capita basis. Incidence-based DALY rates were flat above among citizens > 20 years of age, while the prevalence-based DALY rate increased steadily with age, with the steepest increases seen in those > 60 years of age (Fig. 2B). In particular, the prevalence-based DALY rate was very high at 7,540 per 100,000 populations in the 80+ and over age group. Among the 80+ group, falls was estimated to account for 52.1% of the total DALY rate.
 | Fig. 2DALYs for injuries by age and mechanism in Korea. (A) The incidence and prevalence-based total injury burden by age group. (B) Incidence and prevalence-based injury burden per person after adjusting for the age-matched number in the general population.DALY = disability-adjusted life year.
|
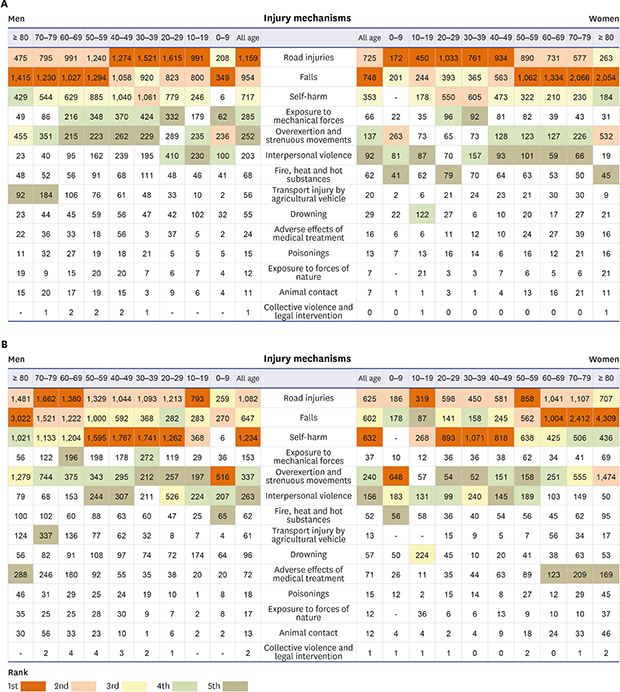
Next, we visualized the injury burden per person by gender and age group (Fig. 3). Road injuries were the highest ranked category for males and falls the highest ranked category for women using an incidence-based approach. By contrast, self-harm was the highest ranked category for both men and women when calculated using the prevalence-based approach. Fall and self-harm were the second and third ranking categories in men using an incidence-based approach, compared with road injuries and self-harm for women. Road injury and falls were the second and third most common causes for both men and women using the prevalence-based results. Mechanical forces and overexertion/strenuous movements were ranked fourth or below in the 30–70 age group, which corresponds to the physically and economically active period in the male incidence-based results. In women, overexertion/strenuous movement and interpersonal violence were ranked higher than that of men. Age-specific differences found transport injury by agricultural vehicle as the most common cause of transportation injury in men over 70 years of age in incidence-based results. Adverse effects of medical treatment were ranked fifth highest in women aged 60 years and over using the prevalence-based method.

DISCUSSION
Overall, calculations measuring the burden of injury using the prevalence-based approach were consistently higher than those determined using the incidence-based method. This observation is most pronounced when calculating DALY rate in individuals > 60 years of age using the prevalence-based method, compared with that seen for the incidence-based approach. By mechanism, falls and road injury had the highest YLD as calculated using the incidence-based and prevalence-based approaches, respectively. In the case of DALYs, road injury was the most significant category in incidence-based results, compared with self-harm in the prevalence-based results. While the overall burden of injury was 1.5 times higher in men, the same categories of road injuries, falls, and self-harm exhibited the greatest burden of injury for both men and women, although the ranking of these categories did differ between incidence-based and prevalence-based results.
Despite significant advances, injury burden continues to be a significant health problem worldwide.1516 Beginning in the late 19th century, many developed countries, including Sweden, the United States, Australia, and some European countries, began promoting injury prevention as a cornerstone of their political agenda.17 The Korean government is also spearheading a high-priority injury-prevention health project as part of the national health plan.18 Evidence regarding the effectiveness of these campaigns can be seen in global age-standardized total injury burden, which declined significantly between 1990 and 2013, with the DALY rate dropping 30.9% (95% uncertainty interval, −34.7 to −26.1) during this interval.19 However, injuries remain a leading causes of global DALYs, as they did back in 1990,4 making injury prevention an important public health issue even today.
As a standard indicator, DALY provides a more comprehensive measure of the relative size of different health problems, calculated as the sum of premature mortality in YLL in addition to non-fatal health outcomes coupled with disability.20 The incidence-based YLD estimation methodology has been updated since DALYs were first calculated as part of the GBD 1990 study21; however, since the incidence-based YLD is calculated as the sum of future health loss related to disease incidence in the reference year, it will not reflect the prevalence of all YLDs, nor does it accurately capture the time between which a disease occurs and the age at which health loss begins.10 Considering the characteristics of this incidence-based approach, GBD 2010 and the WHO have since decided to estimate YLD using a prevalence-based approach as the preferred method for calculating the total health loss in the current year.10 In Korea, the prevalence-based approach for calculating DALYs was first performed in the 2012 KNBD, with this study representing the first effort to expand such an analysis across all fields of injury.22
In 2008, The WHO reported the age distribution of global injury YLDs for 2004 as estimated using a combination of approaches, including classic YLDs, incidence-based YLDs, and prevalence-based YLDs.10 In this report, the incidence-based YLD was higher in younger individuals; however, this trend switched after 37.5 years of age, after which the prevalence-based YLD was higher. In our analysis, incidence-based YLD was higher in individuals < 60 years of age, but similar in the 60-year-old group and the prevalence-based YLD was higher in individuals > 70 years of age. Overall, Korean patients showed similar trends reported by the GBD team, except for the shift to the older age groups, which is likely due to differences in health care utilization between nations.23 Thus, the prevalence-based approach has a significant influence on the age distribution of YLD by estimating cases with high prevalence for each combination of injuries. These results could be applied to the distribution and management of appropriate medical expenditures by understanding the nature of the injury.
The GBD team reported that the global DALY rate of injury in 2015 was 3,376 per 100,000, which is similar to Korea's 3,290 per 100,000 reported in 2014.4 In the GBD analysis, divided into four upper categories, unintentional injury was the most significant cause based on DALY, accounting for 1,481 per 100,000, compared with 1,241 per 100,000 in the Korean study. Unintentional injury was the most common category in both studies, suggesting similar trends between studies. Transport injury, intentional injury, and war and disaster accounted for rates of 971, 741, and 183 DALYs, compared with 891, 1,142, and 16, respectively, in the Korean study4 (Table 3). Overall, Korea's DALY rate was slightly lower than the global levels except for intentional injuries. This result validates the prevalence-based approach used in this study. We also found that prevalence-based YLD for pedal cycle vehicles and adverse effect of medical treatment were higher than those calculated using an incidence-based approach, suggesting that people did not die from the injury but survived with a severe disability. Therefore, an appropriate injury prevention policy should be established with regards to the potential long-term future of each injury mechanism.
We compared the estimated number of injury-associated DALY and rates per 100,000 populations by age based on both the incidence- and prevalence-based approaches (Fig. 2). The DALY was highest in the 30–50 age groups but decreased steadily after age 60. The overall injury DALY showed higher rates for the prevalence-based analysis compared with the incidence-based approach. However, DALY rate adjusted for the population structure showed a different pattern to the absolute DALY. Incidence-based DALY rates were flat across all groups > 20 years of age, compared with the prevalence-based DALY rate, which increased in all groups aged 20 and above. These data provide evidence regarding the long-term trends in the prevalence of non-fatal disability due to injury. In addition, it provides insight into health care utilization behavior of an aging Korean population when compared with the gradual decline of prevalence-based YLD after 52.5 years in the global data.1024
Increases in total DALY rate by mechanism was largely attributed to increased falls in the elderly population, with our data showing a > 50% increase in the total prevalence-based DALY rate in patients 80 years of age and above. This suggests that despite the continued efforts, the expenditure of health care due to falls is still high in the elderly population. Considering the nature of fall mechanisms, once a fall occurs, the sequela remains intensely prevalent and may have long-term effects on quality of life.24 Therefore, it is necessary to develop and implement an appropriate fall-prevention program that addresses the multi-factorial causes of falls. Indeed, several studies have reported significant public health effects following implementation of such a program.2526
Fig. 3 shows the injury ranking by mechanism according to gender and ages. Overall, the men DALY rate was higher in both incidence and prevalence-based results, consistent with that seen in 2012.5 Self-harm was the highest ranking for both men and women economically active age groups in prevalence-based results, indicating the importance of self-harm prevention management in Korea.
Even though the burden of injury has shown tremendous improvement worldwide, the portion of injury to overall health problems is still high.34 Considering that major health problems may change over time, injury-management policies should be conducted with vigilance and flexibility. This can be accomplished by performing continuous monitoring using well-proven, high-quality methods to assess public health priorities. In addition, considering the epidemiological nature of some injuries, a tight network of management policy for environmental levels throughout society will be needed. For this purpose, it will be important to work closely with health professionals, policymakers, politicians, and experts in various fields of society to fully meet the needs of the population.
As mentioned in the previous section, the GBD study team has reported global burden of injury data calculated using a prevalence-based approach since 2010. Comparing injury rate estimations derived by analysis of data obtained using a prevalence-based approach in Korea with international estimates is meaningful. In addition, the incidence-based approach captures only the burden of new injuries, while the prevalence-based approach has the advantage of estimating the overall health burden of injury during the year. The prevalence-based approach can also account for comorbidities more directly than the incidence-based approach. However, in Korea, the burden of all-cause disease is currently estimated using the incidence-based approach, which is useful for making comparisons among diseases and injury mechanism.
This study has several limitations. Because the burden of minor injuries in patients treated in hospitals under 100 beds was excluded from the data resources, it is possible that the burden of injury was underestimated. In addition, in household and web-based surveys for the DW calculation of the health status used to estimate the prevalence YLD, no information was obtained on those who refused or dropped out of the survey.13 This may restrict the result of the study by making it impossible to exclude non-responders when estimating the DW of health states. However, this study is meaningful in that this is the first report on the disease burden of injury estimated based on a prevalence approach in Korea. We also provided estimates that could more precisely predict the injury burden. In addition, using the same classification and methodology as the GBD study, the findings were comparable to the GBD study and were reliable when compared with global data.
 XML Download
XML Download