

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Summary measures of population health (SMPH) are a combination of a fatal health condition that can lead to death and a health condition of a non-fatal health condition.1 SMPH, also referred to as a composite indicator, is distinguished by indicators of health gap or life year and indicators of life expectancy.23 The indictors of health gap are again divided into the disability adjusted life year (DALY) which is utilized in the global burden of disease (GBD) study4 and the quality adjusted life year (QALY) which is mainly used as the outcome index of the cost-utility analysis.5 Furthermore, indicators of life expectancy are also classified into the healthy life expectancy (HALE) which is utilized in the GBD study4 and the quality adjusted life expectancy (QALE) using health-related quality of life.6
Among the SMPH, DALY and HALE are used to estimate the GBD, but there have been also many studies on DALY and HALE in Korea.78910 In order to calculate DALY and HALE, disability weight is an essential factor. The disability weight is a measure of the level of disability of particular health state and diseases, and its value lies between 0 (full health, no disability) and 1 (disability level in a state such as death).11 That is, the disability weight plays a bridging role between mortality and morbidity when estimating DALY and HALE. Therefore, it is necessary to be able to estimate the disability weight appropriately and reliably.12 If the disability weight of a specific disease is overestimated, the burden of the disease may be overestimated. Conversely, if the disability weight is underestimated, there is a possibility of underestimating the burden of disease.
Since 1996, many studies have been conducted to estimate disability weights in many countries.11131415 Most recently, disability weights for the GBD 2013 study was performed using paired comparison as a main valuation method and disability weights for 235 health states were estimated adding the results of European disability weight study.1314 In the case of Korea, two disability weights studies for the Korean Burden of Disease (KBD) 2012 were conducted most recently.1115 In the first study, a total of 496 physician and medical students participated in self-administered web-based surveys and a total of 228 disability weights of disease causes for calculating the incidence-based DALY were estimated.11 In the second study, a total of 2,728 and 3,188 general public participated in the household and web-based survey, respectively, and a total of 258 disability weights of health states for calculating the prevalence-based DALY were estimated.15
However, disability weights calculated in the past may not be valid at this time because of the emergence of new diseases or health states, changes in disease characteristics, development of treatment methods, and changes in social perspectives on disability.12 Therefore, it is necessary to continually evaluate the validity of disability weights and to revise disability weights. In particular, there is an increasing need to calculate the more valid burden of diseases reflecting the severity level of diseases and attempts are being made to calculate the disability weight reflecting the severity level of health states.915 However, there was no attempt to calculate the disability weights for disease causes reflecting the severity level of diseases.
For the KBD 2015 study, we have amended disability weights for causes of disease adapting the methodology of the KBD disability weight 2012 study. In particular, we attempted to further refine the severity level of diseases, such as cancer and diabetes, and to determine their disability weights.
METHODS
Study design and participants
We conducted a self-administered web-based survey in Korea, adapting the methodology of a preceding disability weights measurement study.11 The survey was conducted from November 2016 to March 2017. In this study, we recruited study participants who could be expected to have enough knowledge about causes of disease. Specifically, physicians and medical students who were attending in the third or fourth grade of a regular course participated in the survey. We recruited participants through promotion of the survey in the lectures of medical colleges and an announcement at medical conferences, seminars and meetings.
Valuation method and causes of disease
Each participant responded to his or her age, gender, specialty, and position at the beginning of the survey. Next, the participant evaluated the causes of diseases using a ranking method. That is, the participants ranked causes of disease in order of good health in the ranking method, considering mental and physical problems. Because the survey was conducted for the medical professionals, the descriptions of causes of disease were not developed and the response was obtained by presenting the causes of disease itself to the survey participants. We used a method ranking five causes of disease, which proved to be effective in previous study.16
The five causes of disease were randomly selected among the 289 causes of disease. Among the 289 causes of disease, 211 causes of disease were taken from the previous disability weights measurement study without subdividing severity level.11 For 60 causes of disease, the degree of severity was further subdivided. For example, gastric cancer was classified into four stages: gastric cancer stage I, gastric cancer stage II, gastric cancer stage III, gastric cancer IV. Osteoarthritis was subdivided into three stages: osteoarthritis (mild), osteoarthritis (moderate), osteoarthritis (severe). Diabetes mellitus was classified into two stages: diabetes mellitus without complications and diabetes mellitus with complications. Furthermore, 16 causes of disease were included in the list for the verification of the disability weight model of multimorbidity. For example, two or more causes of disease, such as patients with diabetes mellitus and osteoarthritis, were included in the list. The remaining two causes of disease were ‘full health’ and ‘being dead.’ These were included for use as an anchor points in the analysis.
Each participant performed a total of 20 ranking methods. In order to obtain a sufficient number of comparisons between ‘full health’ or ‘being dead’ and other causes of disease, ‘full health’ should be included in question 1 and 11, whereas ‘being dead’ should be included in question 5, 10, 15, and 20.
Analysis
Initially, we conducted descriptive analyses for determining the characteristics of socio-demographic factors of the participants. Before the disability weight analyses, illogical response that ‘full health’ was not listed as the healthiest condition were excluded from the results. Then, we converted the ranked data into paired comparison data.16 For example, if the orders of causes of disease were “C1 > C2 > C3 > C4 > C5,” they were converted as follows: “C1 > C2,” “C1 > C3,” “C1 > C4,” “C1 > C5,” “C2 > C3,” “C2 > C4,” “C2 > C5,” “C3 > C4,” “C3 > C5,” and “C4 > C5.” After conversion, we ran a probit regression according to the analytic methodology of previous studies.1115 The stated preference between the two causes of disease in the paired comparison data were regarded as the dependent variable. The 289 causes of disease were treated as independent variables and created as dummy variables with ‘being dead’ as the reference. The predicted probabilities for each cause of disease were calculated from the coefficient estimates of the probit regression. ‘Being dead (1)’ and ‘Full health (0)’ were utilized as anchor points to rescale the predicted probability of each cause of disease on a scale from 0 to 1. Using the 95% confidence interval (CI) of the predicted probabilities, the 95% CIs of disability weight for causes of disease were estimated.
The calculated disability weights from this study were compared to those calculated in a preceding disability weights measurement study.11 Stata 13.1 software (StataCorp, College Station, TX, USA) was used for all statistical analyses. P values less than 0.05 were regarded statistically significant in this study.
RESULTS
A total of 605 participants performed the survey. Table 1 shows the details of the participants' socio-demographic characteristics. The participants in the 30s were predominant and the men participants outnumbered women participants in the survey. The specialists accounted for about 60% of the total survey participants, and the medical part specialists were more than the surgical part specialists.
Table 1
Characteristics of the study participants by type of survey

![]()
Of the 1,210 questions that included ‘full health,’ eight (0.7%) were illogical responses for which the ‘full health’ was not listed as the best health status. All of these illogical responses occurred in question 11. Table 2 shows the disability weights and their 95% CIs for 289 causes of disease. The cause of disease with highest disability weight was ‘trachea, bronchus and lung cancers (stage 4) (0.906),’ followed by ‘kidney cancer (stage 4) (0.902)’ and ‘brain and nervous system cancers (0.888).’ The cause of disease with lowest disability weight was ‘acne vulgaris (0.049),’ followed by ‘dental caries (0.065)’ and ‘allergic rhinitis (0.087).’ More than half of the causes of disease (n = 166, 57.4%) had disability weight values of less than 0.5 (Fig. 1). Furthermore, disability weights for about 70% of causes of disease (n = 201, 69.6%) were located between 0.2 and 0.7.
Table 2
Disability weights for 289 causes of disease

![]()

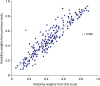
Fig. 2 shows the correlation of disability weights between the disability weights for the overlapping causes of disease from this study and a previous study.11 The Pearson correlation coefficient was 0.930. Among 211 overlapping causes of disease, the disability weights for 47 causes of disease from this study, such as ‘tuberculosis’ and ‘decubitus ulcer,’ were determined to be higher than that from the previous study; whereas, the disability weights for 163 causes of disease from this study, such as ‘schizophrenia’ and ‘epilepsy,’ were estimated to be lower than that from the previous study. The cause of disease with largest difference in disability weight between the two studies was ‘falls (0.448)’, followed by ‘down's syndrome (0.318)’ and ‘asperger's syndrome (0.277).’ Supplementary Table 1 shows comparisons between the disability weights for overlapping causes of disease from this study and the previous study.11
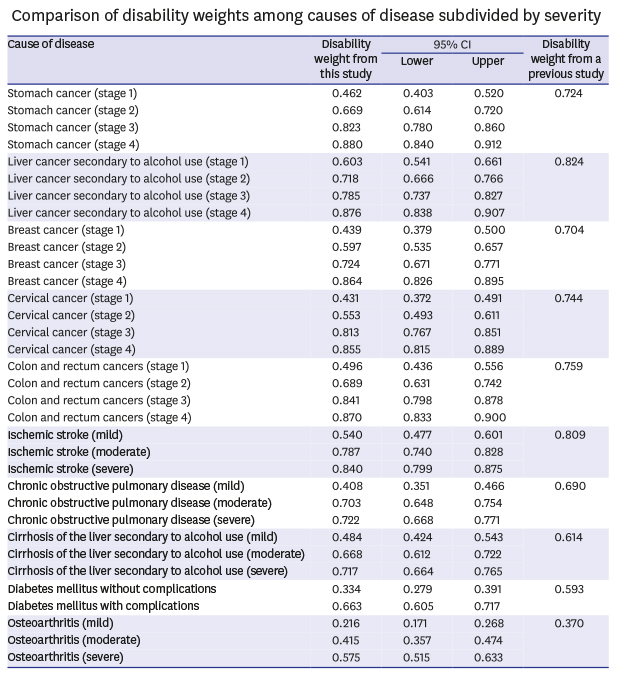
The results of comparing the disability weights of 60 causes of disease that are more subdivided into severity are shown in the Table 3. In the case of ‘liver cancer secondary to alcohol use,’ the disability weights by stage were 0.603 (stage 1), 0.718 (stage 2), 0.785 (stage 3), and 0.876 (stage 4). The disability weight of ‘liver cancer secondary to alcohol use’ in the previous study was 0.824, located between the stage 3 and 4. On the other hand, in the case of ‘thyroid cancer,’ the disability weights by stage were 0.301 (stage 1), 0.484 (stage 2), 0.639 (stage 3), and 0.779 (stage 4). The disability weight of ‘thyroid cancer’ in the previous study was 0.466, located between the stage 1 and 2. Furthermore, the disability weight of ‘diabetes mellitus without complications’ was 0.334, but the disability weight of ‘diabetes mellitus with complications’ was 0.663, with a difference of 0.329.
Table 3
Comparison of disability weights among causes of disease subdivided by severity

![]()
DISCUSSION
In this study, we have amended 289 disability weights for causes of disease adapting the methodology of the KBD disability weight 2012 study.11 In particular, we divided the severity of major causes of diseases unlike KBD disability weight 2012 study and estimated their disability weights. A significant number of physicians and medical students participated in the disability weight survey to collect professional and objective opinions on the preferences of the causes of diseases. Furthermore, we maximized the efficiency of the collecting data by using a method ranking five causes of disease that has not yet been attempted in disability weight studies.
In the meantime, paired comparison has been used as a key value evaluation method in the latest international and domestic disability weight studies.11131415 In this study, however, the ranking method was used as a valuation method, and we determined that the ranking method could be used to calculate the disability weight. Paired comparison has a disadvantage in that the amount of information that can be obtained from a single question is limited, so that the number of items in the survey or the sample size must be increased, if the number of health states or causes of disease to be compared is large.1217 Although the utilization of the ranking method is still low, it can provide more information than the paired comparison. Based on the experience of this study, we expected that the use of the ranking method will increase gradually.
Another difference from previous studies is that we estimated disability weights considering the severity of the causes of disease. We calculated the disability weights of 60 causes of disease considering severity level and compared them with the disability weights in the previous study.11 These results show that prejudice about the severity of cause of disease itself can affect the estimation of disability weight, when estimating the disability weight of cause disease without consideration of severity. For example, disability weight of ‘liver cancer secondary to alcohol use’ by stage were 0.603 (stage 1), 0.718 (stage 2), 0.785 (stage 3), and 0.876 (stage 4). The disability weight of ‘liver cancer secondary to alcohol use’ in the previous study was 0.824, located between the stage 3 and 4 (11). On the other hand, disability weight of ‘thyroid cancer’ by stage were 0.301 (stage 1), 0.484 (stage 2), 0.639 (stage 3), and 0.779 (stage 4). The disability weight of ‘thyroid cancer’ in the previous study was 0.466, located between the stage 1 and 2.11 These results suggest that it is necessary to calculate the disability weight of causes of disease by reflecting the severity in order to calculate the valid DALY in cases of the large severity difference in the cause of disease or the burden of disease is large. However, in this case, epidemiological data according to severity should be also collected to estimate valid DALY.1819
When conducting a disability weight study, we typically estimate disability weights for dozens to hundreds of health states or causes of disease, and the calculated disability weight has a value of a limited scale of 0 to 1. Thus, a disability weight for any health state or cause of disease may seem counterintuitive when compared to other health state or cause of disease's disability weight, and the absolute magnitude of the disability weight may not seem plausible. This will be the same in this study. However, since there is no golden standard for disability weights, it is not easy to assess the validity of disability weights.1217
In this study, the following indirect methods were used to evaluate and enhance the validity of the disability weights. First, we examined whether disability weights were reversed in diseases with different levels of severity. For example, when the severity of an ischemic stroke is classified as mild, moderate, or severe, the disability weight of the mild ischemic stroke should be the lowest, and the disability weight of the severe ischemic stroke should be the highest. No such reversal was found in this study. We also tried to compare the disability weights of the present study with the disability weights calculated in a previous study.11 As a result, it was confirmed that there was a fairly high correlation between disability weights from the two studies. Finally, we tried to increase the number of survey participants and to include various specialist among survey participants. Compared to the size of other studies' samples,17 a significant number of medical professionals have participated in this disability weights survey.
In the recent disability weighting study, the general public is used rather than the healthcare professionals as a participant in the questionnaire.131415 Considering that the reason for estimating the disability weight is to measure the burden of disease and one of the main reasons for measuring the burden of disease is to determine the priority of resource allocation, it is persuasive to calculate disability weights reflecting the preferences of the general public.122021 However, it is not easy to precisely get preferences for health states or causes of disease among the general public who do not have a lot of medical knowledge.1222 It is therefore still worthwhile to utilize healthcare professionals in disability weights studies who are expected to be able to objectively compare and evaluate causes of disease with a wealth of knowledge of various health states and causes of diseases.11 It is expected that comparing and integrating the results of the disability weights studies for healthcare professionals, patients, and the general public will become increasingly important.
One limitation of this study is that it could not perform the verification of the disability weight model of multimorbidity properly. We included 16 causes of disease, such as diabetes mellitus with osteoarthritis, in the list of causes of disease and tried to preliminarily evaluate the validity of multiplicative model, additive model, and maximum model for disability weights in multimorbidity.2223 However, it seems that the meaning of having a complex disease in the survey participants is not enough. As a result, there were some cases in which the disability weight did not increase despite the increased number of cause of disease. For example, the disability weights of ‘allergic rhinitis’ and ‘atopic dermatitis’ were 0.087 and 0.231, respectively, but the disability weight was estimated to be 0.166 for both of these causes of disease. In order to validate the disability weight model in multimorbidity, further studies are needed considering the level of understanding of participants.
Another limitation is that physicians and medical students participating in the survey may not represent the preference for disease among all medical professionals. However, we tried to increase the number of survey participants and to include various specialist among survey participants. Therefore, it is expected that the disability weight derived from this study will not be significantly different from the judgment of the degree of disability of all medical professionals. Future disability weight studies need to involve more medical professionals with various specialties in the survey.
In conclusion, we have estimated 289 disability weights for causes of disease adapting the methodology of the KBD disability weight 2012 study. The disability weights estimated based on the severity can be used to estimate the more accurate burden of diseases. Furthermore, the disability weights from this study can be utilized to estimate health life expectancy, especially HALE, in Korea.
 XML Download
XML Download