

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Nitric oxide (NO) is an endogenous mediator produced from arginine and oxygen by NO synthase (NOS). There are 3 NOS isoforms in the human airway mucosa: the neuronal-type NOS (nNOS), the endothelial-type NOS (eNOS) and the inducible-type NOS (iNOS).12 The first 2 are constitutively expressed and generate relatively low levels of NO, while iNOS is primarily expressed in response to external stimuli such as certain cytokines and bacterial products.3 NO exhaled air of humans was first demonstrated in 1991 by Gustafsson et al.,4 and then in 1993 an increased exhaled NO (eNO) level was found in asthmatic patients.5 Since then, the measurements of eNO as the non-invasive methods for exploration of respiratory tract became attractive. The role of NO in the airway is complex. It was first described as a vasodilator in 1987,6 then other functions were subsequently interpreted as a neurotransmitter and an inflammatory mediator.7 So far, it has been reported to play a role in the regulation of blood flow and ciliary beat frequency, and may also have potential antibacterial effects.
The measurements of NO can be divided into 2 main categories according to clinical purposes. One gathers exhaled air through the nostrils to gain nasal NO (nNO) generated from the upper airway, and the other measures fractional eNO (FeNO) through the mouth to detect the concentration of NO in the lower airway. The recommendations for standardized FeNO measurement have been published by the American Thoracic Society & European Respiratory Society (ERS) for years, which made the measurement of FeNO an essential objective support to the diagnosis and monitoring of lung disease,8 especially asthma.910 The nNO, mainly generated from the sinuses and partially from the nasal mucosa,11 was much higher in the upper respiratory tract than in the lower respiratory tract. It was not so stable as FeNO and can be influenced by many internal and external factors. There is also a significant degree of inter-individual variation over time, which means that changes of 20%-25% or less may account for by normal variation rather than changes in disease status.12 Thus, to some degree, the clinical use of nNO was limited. For some diseases, such as primary ciliary dyskinesia and cystic fibrosis, in which the nNO level is extremely low, the measurement of nNO is recommended as a useful screening tool for diagnosis.1314 Other achievements have also been gained in studies of other rhinal diseases such as chronic rhinosinusitis with or without nasal polyps,1516 and allergic rhinitis (AR).17 However, although the ERS has made an effort to standardize the detection of nNO for the last 20 years,14 there is still no widely recognized normal reference range of the nNO level. The normal range of nNO in Chinese adults based on large-sample, large-age span and multi-external factor control studies is also not available.
AR is one of the most common nasal diseases. The prevalence of AR worldwide is 23%-30% in Europe,18 12%-30% in the United States19 and 11.1%-17.6% in China.2021 Furthermore, it is highly associated with asthma. Rochat et al.22 reported a 41.5% of all new cases of asthma with preceding AR. According to the ‘one airway one disease’ theory, the nNO level may increase in AR patients, as the FeNO level in asthmatic patients. However, the results of previous studies are controversial. We designed a large sample-size study with the attempt to reveal the normal range of the nNO level in Chinese adults and the difference between AR patients, non-AR (NAR) patients and normal people. We also included asymptomatic atopic adults and first analyzed the nNO level in this cohort. The possibility of nNO as a useful diagnostic tool of AR was also taken into account in the current study. Additionally, we strictly controlled the known external factors to investigate the correlation between the nNO level and other internal factors.
MATERIALS AND METHODS
Study design
The study was conducted from November 2011 to December 2011. Participants were recruited from the general public in North China (Huairou region, Beijing) through public announcements. Finally, 1,000 adults were invited to this study. They were asked to complete 2 questionnaires. One questionnaire comprised 24 questions, including demographic information and history of upper airway diseases, lower airway diseases and allergen-related diseases; the other comprised the visual analogue scale (VAS) of clinical symptoms (nasal obstruction, rhinorrhea, sneezing, nasal itching and ocular itching). Seven of the participants did not complete both questionnaires. Of the remaining 993 participants (aged 18-68 years), 345 (34.7%) were males and 648 (65.3%) were females.
The exclusion criteria were: history of lower airway diseases such as asthma, tracheitis or with symptoms like cough and dyspnea; history of upper airway diseases except rhinitis; history of nasal operation. The included subjects needed to undergo the skin prick test (SPT) to determine the atopic status. According to the above criteria, subjects were divided into 4 groups (the flowchart is shown in Fig. 1). The AR here was defined as having physician-diagnosed AR, having nasal symptoms during the screening period and having at least 1 SPT positive result. The NAR was defined as having nasal symptoms for at least 2 years but no positive history of SPT or serum-specific immunoglobulin E. The ‘asymptomatic atopic’ herein stands for the patients having no history of rhinitis and no symptoms during the screening period but being allergic to at least 1 of the screening antigens. Then the participants with no history of upper and lower airway disease, no airway symptoms and negative SPT results were considered normal. The nNO level, FeNO level and nasal airflow resistance of all participants were respectively measured by the same experienced technician.

The Ethics Review Board of Beijing Tongren Hospital and Beijing Institute of Otolaryngology, China (No. 2011013) approved the study, and prior to entry into the study, all participants provided written informed consent.
Assessment of atopic status
Atopic status was determined with SPTs by using a panel of 21 aeroallergens, including Dermatophagoides pteronyssinus, Dermatophagoides farinae, animal hair, Blattella germanica, giant ragweed, mugwort, lamb's quarters, Humulus, Chenopodium album, dandelion, grasses, pine, plantain, locust, trees, Aspergillus fumigatus, Penicillium notatum, Curvularia lunata, Alternaria tenuis and Candida albicans. The aeroallergens were standardized allergen extracts (ALK-Abelló, Hørsholm, Denmark); histamine was used as a positive control, and normal saline solution for a negative control. An allergen/histamine-induced wheal of ≥3 mm was regarded as positive. An experienced technician conducted all SPTs. Atopy was defined as the presence of positive SPT reaction to at least 1 of the 21 aeroallergens.23
Measurements of nNO and FeNO
NIOX MINO (Aerocrine AB, Solna, Sweden), an online NO testing instrument, was used to measure the levels of nNO and FeNO according to the manufacturer' instructions. The measurement unit was parts per billion (ppb). The measurement range of nNO was 5-1,700 ppb and that of FeNO was 5-300 ppb. To avoid the effects of other factors such as sport, diet, and time of the day, we fixed the operation between 9 am to 11 am. The participants needed to rest for at least 30 minutes before the measurement of nNO. A nasal olive with a central lumen was blocked firmly against the nostrils and connected to the NIOX MINO (Aerocrine AB). The transnasal airflow was at a fixed and constant flow rate of 0.25–3 L/min. Subjects were asked to breathe normally. Slow oral exhalation against the resistance of at least 10 cm H2O was performed to obtain velopharyngeal closure that can avoid the results of nNO being influenced by air from the lower airway.24 The measurements were carried out for the right and left nasal cavities separately, with the other nostril closed in turn. The mean value was determined after 3 exhalations. After the measurement of nNO, the subjects were asked to rest for 15 minutes. After that, they were asked to stand and exhale to residual volume. After the mouthpiece was placed, the subjects inhaled to total lung capacity, and then exhaled for 10 seconds at a constant flow rate of about 50 mL/s to gain the FeNO value.
Measurements of nasal airflow resistance
Nasal resistance was measured by heart rate recovery at 2 minutes 4-phase rhinomanometry (RhinoLab GmbH, Rendsburg, Germany), and nasal patency was measured by acoustic rhinometry (Ecco Vision; Hood Laboratories, Pembroke, MA, USA). All measurements were conducted in an examination room at a temperature of 22°C-24°C and 40%-70% humidity. Before the examination, participants were asked to sit quietly for 20 minutes and maintain upright posture throughout the measurements. For rhinomanometry, the total nasal resistance was measured at the pressure of 75 Pa (T75) and 150 Pa (T150). For acoustic rhinometry, nasal volume within 0–7 cm from the anterior nares (V0–7cm) was measured. To maintain a constant congestive state, these measurements were completed within 6 minutes.
Statistical analysis
The 1-sample Kolmogorov-Smirnov test was performed to analyze the distribution of baseline variables. Both nNO and FeNO values of the study participants were non-normally distributed and were expressed as median, interquartile range (IQR), 95% confidence interval (95% CI) and range. The comparisons between groups were conducted by the Mann-Whitney U test and the Kruskal-Wallis test. Correlation was examined using Spearman correlation analysis. A P value of < 0.05 was considered significant. All statistical analyses were performed using SPSS software, version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic characteristics of the study subjects
Based on the medical history and VAS symptom scores, 100 subjects were excluded; 60 with chronic rhinosinusitis, 14 with nasal polyps, 40 with asthma and 1 with tracheitis (the numbers were not mutually exclusive). The others were divided into 4 groups according to the medical history, VAS symptom scores and SPT results. The measurement of nNO showed higher effective detection rate than the measurement of FeNO in all groups. The details of the demographic characteristics of the subjects and the nasal resistance data are shown in Table 1.
Table 1
General characteristics of the study population

Values are presented as number (%), median (IQR) or mean ± standard deviation.
AR, allergic rhinitis; NAR, non-allergic rhinitis; IQR, interquartile range; BMI, body mass index; BSA, body surface area; T75, total nasal resistance measured at the pressure of 75 Pa; T150, total nasal resistance measured at the pressure of 150 Pa; V0–7cm, nasal volume within 0–7 cm from the anterior nares; nNO, nasal nitric oxide; FeNO, fractional exhaled nitric oxide.
*Atopy subjects with positive SPT results but absence of respiratory diseases or symptoms.
†Efficiency represents the proportion of successful measurements of valid values.
![]()
The nNO and FeNO in healthy subjects
The below detection missing values were expressed as half-detection-limit and the final calculation results were all integers. The levels of nNO and FeNO were both non-normally distributed. The median of nNO in the healthy group was 91 ppb (IQR, 51-143 ppb; 95% CI, 3-269 ppb); the median FeNO level in healthy group was 9 ppb (IQR, 6-13 ppb; 95% CI, 3-24 ppb). The nNO levels were significantly higher in females than in males (P = 0.002), while the FeNO levels were significantly lower in females than in males (P = 0.012). There was no difference in nNO and FeNO levels between smokers and nonsmokers. Details are shown in Table 2.
Table 2
The nNO and FeNO levels of healthy Chinese adults

nNO, nasal nitric oxide; FeNO, fractional exhaled nitric oxide; IQR, interquartile range; CI, confidence interval.
*The comparison between sexes used the Mann-Whitney U test, significant with P < 0.05.
†The comparison between smokers and nonsmokers used the Kruskal-Wallis test, significant with P < 0.05.
![]()
Comparison between the study groups
The comparisons of nNO and FeNO levels between groups are shown in Figs. 2 and 3. As in Fig. 2, the nNO levels were significantly higher in AR patients than in the normal subjects (P = 0.033) and asymptomatic atopic subjects (P = 0.001). The nNO levels were significantly higher in the NAR patients (P = 0.002) and normal subjects (P = 0.039) than in the asymptomatic atopic patients. There was no difference in the other 2 pairs of comparisons, AR patients versus NAR and the normal subjects versus NAR patients. For FeNO levels, the AR and NAR groups showed higher values than the normal subjects (P = 0.001 and P = 0.002, respectively) and the asymptomatic atopic patients (P = 0.009 and P = 0.022, respectively) as shown in Fig. 3. No difference was shown between the comparisons of the other 2 pairs.
 | Fig. 2The comparisons of nNO values between different subgroups. The NO values are represented by box diagram.nNO, nasal nitric oxide; NO, nitric oxide; AR, allergic rhinitis; NAR, non-allergic rhinitis.
*The significance of the difference between groups is indicated by the asterisk on the lines above the 2 sets of box plots. The more asterisks, the more significant is the difference.
|
 | Fig. 3The comparisons of nasal FeNO values between different subgroups. The NO values are represented by box diagram.FeNO, fractional exhaled nitric oxide; NO, nitric oxide; AR, allergic rhinitis; NAR, non-allergic rhinitis.
*The significance of the difference between groups is indicated by the asterisk on the lines above the 2 sets of box plots. The more asterisks, the more significant is the difference.
|
Correlation analysis
As shown in Table 3, the correlation analysis revealed that the nNO level was positively correlated with the VAS score (total P = 0.001, r = 0.111; nasal obstruction P = 0.012, r = 0.091; sneezing P = 0.007, r = 0.101), T75 (P = 0.010, r = 0.097) and FeNO (P = 0.000, r = 0.173); inversely correlated with nasal volumes of V0–7cm (P = 0.000, r = −0.188); independent of age, height, weight, body mass index (BMI) and body surface area (BSA). FeNO was positively correlated with age (P = 0.009, r = 0.162), height (P = 0.001, r = 0.200), weight (P = 0.032, r = 0.134), BSA (P = 0.008, r = 0.165) and VAS score (total P = 0.000, r = 0.197; nasal obstruction P = 0.000, r = 0.206; rhinorrhea P = 0.000, r = 0.163; sneezing P = 0.000, r = 0.180; nasal itching P = 0.000, r = 0.183; ocular itching P = 0.000, r = 0.136); inversely correlated with nasal volumes of V0–7cm (P = 0.000, r = −0.138); independent of BMI, T75 and T150. The correlations were significant according to P value; for all of them, the |r| < 0.3 revealed that the correlation was weak.
Table 3
Correlations among nNO, FeNO and other factors

nNO, nasal nitric oxide; FeNO, fractional exhaled nitric oxide; BMI, body mass index; BSA, body surface area; VAS, visual analogue scale; T75, total nasal resistance measured at the pressure of 75 Pa; T150, total nasal resistance measured at the pressure of 150 Pa; V0–7cm, nasal volume within 0–7 cm from the anterior nares; r, correlation coefficient.
*Significant with P < 0.05; †Significant with P < 0.01.
![]()
Cutoff values of nNO and FeNO for the diagnosis of AR
The results of the present study showed that in subjects with AR, the receiver-operator characteristic curve of nNO and FeNO were both with low area under the curve (AUC) values (nNO: AUC, 0.556; FeNO: AUC, 0.608) and the cutoff points according to the Youden index also showed low sensitivity and specificity (nNO: cutoff value, 117.5 ppb; sensitivity, 50.9%; specificity, 63.9%; FeNO: cutoff value, 10.5; sensitivity, 64.3%; specificity, 52.4%) (Fig. 4).
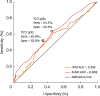 | Fig. 4The ROC curve and cutoff point of nNO and FeNO for predicting AR. The diagonal line is the reference line, which represents the AUC of 0.5. The ROC curve of nNO is shown in blue and the ROC curve of FeNO is shown in green. The cutoff values of nNO and FeNO from the Yoden index are marked on each curve with points of different shapes. The exact cutoff value is shown below the mark point on the nNO curve and above the mark point on the FeNO curve with their sensitivity and specificity behind.Sens, sensitivity; Spec, specificity; ROC, receiver-operator characteristic; nNO, nasal nitric oxide; FeNO, fractional exhaled nitric oxide; AR, allergic rhinitis; AUC, area under the curve.
|
DISCUSSION
The nNO can be influenced by multiple external factors, such as season,25 time points of the day,26 physical exercise,27 breathing method and the analyzers.28 The mean normal value of nNO varied from 79 to 1,380 ppb according to the published studies29 Many of the published articles did not fully describe the aforementioned external factors or make any effort to control them. This may not only enlarge the variation in a single study, but also lead to a lack of comparability between different studies. To reduce the variation derived by these factors, the present study was conducted in the same season (winter), and a single experienced technician conducted all the measurements of nNO using the same analyzer during the same time points of the day after the participants sat quietly for 30 minutes. To eliminate race factors,30 we mainly compared the normal value (18-68 years; median, 91 ppb; IQR, 51-143 ppb; 95% CI, 3-269 ppb) to that of healthy Chinese people. We then found that our result was similar to that of the study by Leng et al.29 (n = 182; mean ± standard deviation [SD], 79 ± 35 ppb),29 but much lower than that of the study by You et al.31 (n = 120; mean ± SD, 273.5 ± 112.3 ppb). The equipment we used was the same (NIOX MINO; Aerocrine AB). The difference in results may relate to the different procedure. In the present study, the participants were asked to breathe normally, while in Shaohua You's study patients were asked to hold their breath for 45 seconds during the measurement. Although someone argued that all methods of NO measurement had excellent reliability according to their really limited sample size (normal, n = 10; AR, n = 23),32 the differences in operation should not be ignored. Besides the methods, normal breathing, breath holding and tidal-breathing, etc.,33 the differences in instruments can also bring a wide variation in results. Leigh et al.34 proposed a standardized method for testing primary ciliary dyskinesia to study online nNO across a number of 6 collaborating sites with different analyzers. However, another study highlighted the difference in the nNO levels between online and offline methods.35 To reduce the variation in nNO levels, controlling external factors is very important. Although the reference value of nNO is not currently used to diagnose diseases, it is very important to establish the normal range of nNO levels in different populations to compare relevant studies. The present study described the technique in a comprehensive and detailed way and the studied population has a large age span and a large sample size, which made the results of the normal range here more reliable.
In the current study, although nNO and FeNO showed a significant correlation (r = 0.173, P = 0.000), their sex differences were inconsistent. In females, nNO is higher than in males, while FeNO is lower in females than in males. The sex difference of nNO levels remains debatable: some studies reported results consistent with ours,21 others did not.3136 However, the sex difference in the current study can be reasonably explained. In our previous study of nasal resistance, the total nasal resistance is significantly higher in females than in males.37 In the current study, the nNO level is positively correlated with total nasal resistance, which could explain why females have higher nNO levels than males. The correlation analysis of the normal group revealed that the FeNO level was positively correlated with height, weight and BSA, which were higher in males than in females.
Besides the normal value, the current study also aimed to investigate the nNO of AR patients. The questionnaires and SPTs about sensitization to 21 different aeroallergens gave us the supporting materials to separate the sample into different groups. The comparisons between the groups showed that the nNO and FeNO levels were significantly higher in AR patients than in normal subjects, which corresponds to results of some other studies.383940 In NAR patients, the nNO levels were not different compared with the norms, while the FeNO levels were significantly higher than in the normal controls. No difference was found in the nNO levels between AR and NAR patients.
However, the results of the studies on nNO in rhinitis patients were not consistent. A Norwegian general population study showed that nNO was similar in subjects with allergic or perennial rhinitis compared with controls,41 and another one also found no relation between current rhinitis and nNO concentration.42 It has been known that airway allergic inflammation results from the activation of mast cells and antigen-specific type-2 T-helper cells, with the concomitant release of cytokines, including interleukin (IL)-4, IL-5 and IL-13. In the studies of asthma, the release of the mentioned inflammatory factors can regulate iNOS expression in epithelia and then lead to higher NO generation.43 Similar results were found in the studies of AR. Olthoff et al.44 found elevated nNOS immunoreactivity around glands in patients with AR. Likewise, Takeno et al.45 found that nasal epithelial cells of allergic patients overall produce higher levels of NO through concomitant expression of different isoforms (iNOS and eNOS). Some other studies revealed the increased expression of iNOS in epithelial cells of AR patients as well.114647 These findings regarding the elevated NOS explain well significant results here. According to the above results, nNO can objectively reflect inflammation in AR patients. For the insignificant results of the other studies, we should further look into the correlations between nNO, nasal resistance and sinus obstruction.48
In the current study, we found a positive correlation between nNO and T75 and an inverse correlation between nNO and V0–7 cm, revealing that the nNO concentration detected could be increased when the patency of nasal airway decreased. However, there also existed the controversial results. Takeno et al.49 found that nNO was independent of nasal airflow resistance. Three points here may account for different conclusions. First, they did not measure nasal volume, which in our study was significantly correlated with the nNO level. Secondly, they only measured nasal resistance at 100 Pa, which is not widely used. According to our study, nasal resistance only positively related to nNO concentration at 75 Pa, but not at 150 Pa. Besides the above results, the obstruction of the sinus ostia should also be taken into account. As previously reported, nNO was mainly generated from the paranasal sinus, and the nasal mucosa only generated a small amount of nNO. Sinus NO is found in the range of thousand ppb and decreased to approximately half in the nose.50 A study comparing nNO levels between the inferior turbinate surface and the middle meatus in AR patients found that the middle meatus area showed higher nNO than the inferior turbinate area in all subjects; the AR patients showed a significantly higher nNO level in the inferior turbinate area than the normal control, but no significant difference with the nNO in the middle meatus area; the ratio of nNO levels of the middle meatus area to the inferior turbinate area was significantly lower in the AR groups. These results suggested that the high background nNO output of the paranasal sinuses is still implicated in AR patients where the allergic inflammation of nasal mucosa did not change the NO level of the middle meatus area. The high background levels of NO from constitutive sources may blunt the smaller increases in nasal mucosal NO output. If inflammation further impairs the patency of the sinus, the entrance of high concentration NO into the nasal cavity is blocked, which resulted in a decrease in nNO51 levels. Thus, the increase tends to be obscured, whereas the decreases (as in primary ciliary dyskinesia and chronic sinusitis with nasal polyps) are apparent. This may also explain why the use of the nNO level for the diagnosis of AR is not ideal. Therefore, if the condition of the sinuses was not evaluated or the sample size was not big enough, a biased insignificant result could appear. Hence, we concluded that nNO can reflect allergic inflammation in AR patients and that sinus edema, congestion and mucus accumulation are all factors need to be considered in the diagnosis or treatment evaluation.
No previous studies have assessed the nNO level in asymptomatic atopic adults. Hence, the current study showed the useful data in this aspect. It first showed a significantly lower of nNO level in the asymptomatic atopic patients than in the normal subjects (P = 0.039). Obviously, the nNO levels were also significantly lower of the asymptomatic atopic patients than in the AR and NAR patients. There have been few studies reporting FeNO levels in asymptomatic atopic patients. A previous study was conducted in Korean children (6–23 years),52 with the result that asymptomatic atopic children had a higher mean FeNO level than non-atopic children. To some extent, this result was different from ours. However, Kharitonov et al.53 found that the nNO levels decreased 1 hour after the start of nasal measurement. There exists an inflammation reaction stage with a decreased nNO level before its increase and symptom attacks; otherwise, the lower nNO level was just the characteristic of asymptomatic atopic subjects to differentiate them from AR patients. Further exploration and long-term follow-up are needed to be to clarify the role of NO in the inflammatory process of AR patients.
FeNO showed a positive relationship with age (P < 0.01), which was reported in other studies in children,54 but seldom in adults. This may be due to the different age span of the study samples. In our study, the age of participants ranged from 18 to 68 years. This 50-year age span may have caused its correlation with NO. The correlation between the NO level and nasal symptoms has been evaluated in previous studies, both in adults and in children.55 However, the correlations were weak for all the typical symptoms of AR.
There are some limitations in the current study: the sex imbalance and the bias of smokers and nonsmokers. In the current study, the nNO levels was significantly higher in females than in males, while the FeNO levels were significantly lower in females than in males. Sex imbalance may have caused non-normal distribution. Smokers here only made up a small percentage of the study subjects. No relationship was found between NO and smoking. In another study, current smokers showed significantly lower levels of nNO compared with nonsmokers, in which the study subjects were adequately balanced.42
In conclusion, nNO is an objective indicator with a high effective detection rate in the general population. The non-standardized process of operation, differences in analyzers limited the comparability between the study groups. Although the reference value of nNO is not currently used for the diagnosis of diseases, it is very important to determine the normal range of nNO in the comparison of different studies. The nNO level has a significantly positive correlation with the nasal symptom VAS score and an inverse correlation with nasal patency. There was a significant difference in the nNO level between AR patients and healthy adults. By using our technique of nNO measurement, nNO can be used to diagnose AR. However, since many external and internal factors contribute to the difference in the nNO level, the controlling confounding factors should be considered in future study design.
 XML Download
XML Download