

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Glucocorticoids remain a useful therapeutic option in the management of persistent asthma.1 However, glucocorticoids decrease the function and number of osteoblasts and cause an increase in osteoblast and osteocyte apoptosis, and prolong the lifespan of the osteoclast.2 Unsurprisingly, glucocorticoid therapy is the most common cause of secondary osteoporosis, and fragility fractures occur in 30% to 50% of patients receiving long-term glucocorticoid therapy.3 Among fragility fractures, vertebral fractures are the most common, and are associated with chronic back pain, shorter height, kyphosis, reduced pulmonary function, abdominal discomfort, disability and death.45
Bone mineral density (BMD) accounts for approximately 70% of an individual's bone strength, which encompasses both bone density and bone quality.6 Occasionally, BMD measurement alone fails to predict overall fracture risk. Indeed, vertebral fractures have been found to occur at higher BMD values in patients receiving glucocorticoids than in untreated patients.7 Therefore, bone quality may contribute more to the increased risk of fractures in individuals treated with glucocorticoids than BMD.
Trabecular bone score (TBS) is a new texture parameter obtained from the analysis of dual-energy X-ray absorptiometry (DXA) images. TBS reflects gray-level pixel variations in the spine on DXA images and is related to trabecular microarchitecture, thereby providing information independent of BMD.8910 Higher TBS values reflect stronger, more fracture-resistant microarchitecture. Some evidence suggests that TBS may play a role in identifying secondary causes of increased fracture risk, such as excessive use of glucocorticoid, hyperparathyroidism, and type 2 diabetes.11 Glucocorticoid is known to affect regions of the skeleton that have abundant trabecular bone such as the lumbar spine and proximal femur.3 The increased risk of fracture associated with glucocorticoid-induced osteoporosis cannot be fully explained by changes in BMD. Interestingly, TBS has been found to provide additional information on glucocorticoid-associated alterations in bone quality.12 In a previous study, the presence of subclinical hypercortisolism was shown to be associated with a significantly higher number of fractures and a considerably lower TBS. Despite these changes in TBS, BMD at the spine and femur remained normal. These results indicate that subtle, albeit excessive, endogenous cortisol exposure can have a significant impact on bone microarchitecture without any change in BMD.13 Nevertheless, although several studies have reported associations between the use of an inhaled corticosteroid (ICS) and systemic corticosteroid (SCS) and a decline in BMD in patients with asthma,141516 no study has investigated TBS in asthmatic patients according to the use of corticosteroids.
This study aimed to evaluate TBS according to asthma severity and to identify correlations between TBS and ICS dose, cumulative doses of SCS, and asthma severity in patients with asthma.
MATERIALS AND METHODS
Study design
The present study was conducted as a retrospective cross-sectional study using electronic medical data. A study scheme is provided in Fig. 1. From April 2005 to March 2017, BMD values were collected at a single university hospital in Korea. The index date was defined as the most recent date of BMD measurement. A total of 10,122 subjects underwent BMD measurement during this period. Among them, 627 diagnosed as asthma based on their primary diagnosis code of J45 and prescribed anti-asthmatic medication at least once were included. Patients with non-active asthma (group 3, n = 333) were defined as those who have been prescribed asthma medication (ICS, ICS + long-acting beta-adrenoceptor agonist [LABA], leukotriene receptor antagonist [LTRA] for less than 90 days and no short-acting beta-agonists [SABA]) over a period of 1 year prior to the index date. Severe asthma was defined operationally in the present study as asthma which required high intensity treatment (high ICS + LABA/LTRA or systemic steroid) and required rescue medicines even though maintaining medium ICS + LABA/LTRA based on international guidelines of ERS/ATS.17 Severe asthma (group 1, n = 138) was defined as the presence of one of the the following over a period of 1 year prior to the index date in individuals diagnosed with asthma: 1) high ICS + LABA or high ICS + LTRA ≥ 180 days, 2) medium ICS + LABA or medium ICS + LTRA ≥ 300 days and SABA use, or 3) use of SCS ≥ 180 days. Among the patients with active asthma, 156 were categorized with non-severe asthma (group 2). Oral corticosteroid (OCS) burst was defined as systemic steroid use at a dose equivalent to at least 15 mg of prednisolone per day for 3 days or longer to control asthma exacerbation. Asthma exacerbation was defined as 1) OCS burst ≥ 2 events or 2) hospital admission (emergency department or wards) for the treatment of asthma attack ≥ 1 event. To select controls with which to compare asthmatics, propensity score matching was applied for age and sex using SPSS, version 23.0 (IBM cooperation, Armonk, NY, USA) (group 4, n = 627).
 | Fig. 1Scheme of study subject selection.ICD, International Classification of Diseases; ICS, inhaled corticosteroid; LABA, long-acting beta-adrenoceptor agonist; LTRA, leukotriene receptor antagonist; BMD, bone mineral density; SABA, short-acting beta agonists; ER, emergency room; PSM, propensity score matching.
|
Prescription history of anti-asthmatics, steroids, and osteoporosis agents was collected for 1 year prior to the index date. Personal cumulative steroid use from the initial visit to the index date was also collected. The use of SCS was investigated from the patients' prescriptions related to asthma. The medical records of all subjects were reviewed retrospectively to obtain data on demographics (age, height and weight), asthma-related clinical information (disease duration, forced expiratory volume in 1 second [FEV1], FEV1/forced vital capacity [FVC], the provocative concentration of methacholine that causes a 20% decrease in FEV1 from baseline [methacholine PC20], and detailed prescription data on asthma medications and glucocorticoids), comorbidities of chronic obstructive pulmonary disease (COPD), rheumatoid arthritis (RA) or systemic lupus erythematosus (SLE) and International Classification of Diseases-10 codes related to osteoporotic fracture (osteoporosis with current pathological fracture [M80]). Systemic steroid and ICS doses were calculated as prednisolone equivalent doses (g) and fluticasone propionate equivalent doses (mg), respectively. This study was approved by the Institutional Review Board of Ajou University Hospital, and informed consent was waived.
Measurement of BMD and TBS
Densitometric examinations were performed with a Lunar iDXA apparatus (enCORE version 15.0; GE Healthcare, Madison, WI, USA). The coefficients of variations for BMD were 0.339% (L1-L4), 0.679% (femur neck), and 0.794% (total hip). TBS was measured using TBS iNsight® software, version 2.1 (Med-Imaps, Pessac, France) with anonymized spine DXA files from the database. The investigator encharged with assessing TBS was blinded to all clinical parameters and outcomes. The average short-term reproducibility for TBS was 1.408%. Diagnosis of osteoporosis was made using the World Health Organization T-score criteria (T-score ≤ −2.5) calculated from Korean reference data.
Statistical analysis
Comparisons of clinical characteristics, BMD, TBS, lung function results, and cumulative steroid doses among the four study groups were conducted with analysis of variance and Pearson's χ2 test for continuous and categorical parameters, respectively. Pairwise comparisons were corrected by Tukey and Bonferroni, for continuous and categorical parameters, respectively. The t-test was used to compare lung function and OCS burst between groups of severe and non-severe asthmatic patients. In analysis of TBS and BMD levels according to age, asthma severity, cumulative steroid dose 1 year prior to the index date, and active treatment for asthma, a generalized linear model with identity link function was used. We classified groups 1 and 2 into 4 subgroups based on the presence of exacerbation and compare TBS levels according to asthma severity and the presence of asthma exacerbation using generalized linear models. To identify predictors for TBS levels, age, sex, comorbidities, body mass index (BMI), prescription of anti-osteoporosis medications, severe asthma, ICS and SCS doses for the previous year, the frequency of OCS burst, and cumulative dose of SCS over all visitation days were evaluated by generalized linear models, presenting odds ratios (ORs) with 95% confidence intervals (CIs). Pearson's correlation was examined for correlations between BMD data and cumulative ICS and SCS doses for the previous year. Partial correlation analyses were applied to understand whether there are linear relationships between BMD data and asthma-related clinical parameters, whilst controlling for ICS and SCS doses. All analyses were conducted using SPSS ver. 23.0 (IBM cooperation). A P value of < 0.05 was considered statistically significant.
RESULTS
Study populations
Table 1 summarizes the characteristics of the study subjects. The percentage of males was significantly higher in group 1 (severe asthma, 29.7%) than in group 2 (non-severe asthma, 12.8%, P = 0.002), group 3 (non-active asthma, 13.5%, P < 0.001), and group 4 (non-asthmatic controls, 16.7%, P = 0.003). Mean age was not significantly different among the study groups. Applying the definition of severe asthma in the present study, we identified 138 severe asthma patients: 49 (35.5%) used high ICS + LABA or high ICS + LTRA ≥ 180 days, 30 (21.7%) used SCS ≥ 180 days, and 78 used SABA under maintaing medium ICS + LABA or medium ICS + LTRA ≥ 300 days. The proportions of patients accompanied with COPD, RA or SLE, who are frequently treated with SCS, were different between the asthma and control groups. In groups 1, 2 and 3, the prevalence of COPD was significantly higher than in group 4. The percentage of patients taking anti-osteoporotic medications was significantly higher in groups 1 and 2 as compared with the controls. The cumulative SCS dose throughout all visit days (7.50 ± 9.3) and the cumulative SCS dose for 1 year prior to the index date (1.22 ± 2.0) were significantly higher in group 1 than in all other groups (3.10 ± 4.4 and 0.44 ± 1.1 for group 2, 4.22 ± 7.2 and 0.38 ± 0.8 for group 3, 1.66 ± 4.8 and 0.18 ± 0.5 for group 4). As the prevalence of RA and SLE was higher in group 3 than in the control group, the higher cumulative SCS dose and the longer days of SCS use were shown in group 3 as compared with group 4. FEV1 predicted % (72.33 ± 24.8 vs. 91.89 ± 22.5, P < 0.001) and FEV1/FVC (78.98% ± 13.4% vs. 86.58% ± 11.3%, P < 0.002) were significantly lower in group 1 than in group 2. The proportion of patients who had experienced severe asthma exacerbation for 1 year prior to the index date (78.3% vs. 46.8%, P < 0.001), including OCS burst at least twice (66.7% vs. 35.3%, P < 0.001) and admission for treatment of asthma attack (33.3% vs. 18.6%, P = 0.005), was significantly higher in group 1 than in group 2.
Table 1
Clinical characteristics of the study groups

Mean and standard deviation was presented for continuous variables. Group 1: severe asthma; Group 2: non-severe asthma; Group 3: non-active asthma; Group 4: non-asthma. Clinical characteristics were examined with trend test (P for trend).
BMI, body mass index; COPD, chronic obstructive lung disease; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; TBS, trabecular bone score; BMD, bone mineral density; ICS, inhaled corticosteroid; SCS, systemic corticosteroid; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; methacholine PC20, provocative concentration of methacholine that causes a 20% decrease in FEV1 from baseline; OCS, oral corticosteroid; ER, emergency room; severe asthma exacerbatin, oral corticosteroid burst ≥ 2/year or ER visit or admission for asthma over 1 year prior to the index date.
![]()
TBS and BMD in patients with asthma and controls
TBS was significantly lower in the severe asthma group (1.32 ± 0.1) than in the non-severe asthma group (1.36 ± 0.1, P = 0.001), the non-active asthma group (1.38 ± 0.1, P < 0.001) and the non-asthmatic controls (1.39 ± 0.1, P < 0.001, Table 1). However, we discovered no significant differences in BMD among the 4 study groups.
Fig. 2 shows interactions noted for TBS and BMD in relation to asthma severity and age groups. TBS and BMD were plotted against age groups and stratified by asthma severity. Old age was the main factor affecting TBS and BMD in asthmatics and controls. BMD levels were dependent primarily on age groups, not on asthma severity. Moreover, a significant interaction between age and disease status on TBS was also revealed by a generalized linear model (P < 0.001, Fig. 2A), after adjusting for cumulative SCS doses for 1 year prior to the index date as a covariate. However, for BMD values (P = 0.205, Fig. 2B), no significant interaction between age and disease status was indicated by the generalized linear model. Using TBS levels in patients aged over 65 years with severe asthma as a reference, TBS levels were significantly differentiated according to disease status among the 3 age groups. In the severe asthma group, no significant difference was noted in TBS levels between patients aged over 65 years and 50-64 years.
 | Fig. 2(A) TBS and (B) BMD according to age and study grouping. P values were evaluated by generalized linear models adjusting for cumulative systemic steroid dose (g) for 1 year prior to index date.TBS, trabecular bone score; BMD, bone mineral density.
*P < 0.05; †
P < 0.01 for comparing to TBS levels in patients with severe asthma aged over 65 years old.
|
Correlations between bone mineral densitometry results and clinical parameters in asthmatics
TBS showed a significant positive correlation with all other BMD indices (correlation coefficient 0.350, P < 0.001 for BMD; 0.356, P < 0.001 for T-score). We evaluated the association between TBS and asthma-related clinical makers in subjects with asthma (Table 2). Therein, TBS was significantly correlated with cumulative SCS (−0.163, P < 0.01) and ICS (−0.192, P < 0.01) doses during the previous year before the index date, while no significant correlation was observed between BMD and steroid doses. In contrary, regarding the lifetime SCS dose showed a significantly negative linear relationship with BMD, not with TBS (Table 2). In partial correlation analyses controlling for cumulative ICS and SCS doses, TBS was also significantly associated with lung function parameters, including FEV1 predicted % (correlation coefficients 0.289, P < 0.01), and methacholine PC20 (0.224, P < 0.05), asthma duration (−0.197, P < 0.05) and age (−0.524, P < 0.01) In contrast, BMD was only significantly correlated with BMI (0.207, P < 0.05), not with age, FEV1 predicted %, methacholine PC20 in patients with asthma.
Table 2
Correlations for bone mineral densitometry results with age and asthma-associated parameters in 627 asthmatics
Partial correlation coefficient adjusted for ICS and SCS dose.
TBS, trabecular bone score; BMD, bone mineral density; BMI, body mass index; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; methacholine PC20, provocative concentration of methacholine that causes a 20% decrease in FEV1 from baseline; ICS, inhaled corticosteroid; SCS, systemic corticosteroid.
*P < 0.05; †
P < 0.001.
![]()
To compare TBS levels according to asthma severity and the presence of asthma exacerbation, we classified severe and non-severe asthma groups into 4 subgroups based on the presence of asthma exacerbation. Compared with TBS levels in patients with non-severe asthma without exacerbation (1.38 ± 0.1, Fig. 3A), all mean levels of TBS in non-severe asthmatics who had experienced asthma exacerbation (1.34 ± 0.1, P = 0.011) and in severe asthmatics who had experienced exacerbation (1.32 ± 0.1, P < 0.001) were significantly less when both ICS and SCS doses were adjusted. However, BMD levels did not differ among the 4 subgroups (Fig. 3B).
 | Fig. 3TBS and BMD according to asthma severity and existence of exacerbation. P values were obtained by generalized linear models controlling with inhaled and systemic corticosteroid doses over the year prior to bone mineral densitometry measurement. Each level of TBS and BMD was compared to non-severe asthma without exacerbation as references.TBS, trabecular bone score; BMD, bone mineral density.
|
We investigated whether the cumulative ICS dose for 1 year prior to the BMD measurement affected TBS levels using a generalized linear model adjusting for age, sex, use of anti-osteoporotic medications, and cumulative SCS dose (Fig. 4). No significant difference in TBS levels between asthmatics without using ICS and those using less than a fluticasone propionate dose equivalent to 180 mg (1.38 ± 0.1 vs. 1.34 ± 0.1, P = 0.052). However, compared with no ICS users, asthmatics who had taken ICS at least 180 mg (1.33 ± 0.1, P = 0.002) for 1 year showed significantly lower levels of TBS. However, no significant difference in BMD levels was discovered between ICS users, regardless of ICS dose, and non-ICS users.
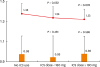 | Fig. 4TBS and BMD according to ICS dose. P values were obtained by generalized linear models adjusting for age, sex, use of anti-osteoporotic medications and systemic corticosteroid dose over the year prior to measurement of TBS (line) and BMD (bar). Patients without ICS treatment were used as references.TBS, trabecular bone score; BMD, bone mineral density; ICS, inhaled corticosteroid.
|
Predictors for TBS levels in patients with asthma
Old age (ORs, 0.997; 95% CI, 0.996-0.998; P < 0.001), patients with severe asthma (0.959; 0.929-0.991; P = 0.013), and cumulative SCS dose for the previous year (0.987; 0.978-0.997; P = 0.013) were significant and independent predictors for lower TBS levels, along with sex, comorbidities of COPD, RA or SLE, BMI, ICS dose for the previous year and cumulative SCS dose for the lifetime, number of OCS burst, and using anti-osteoporotic medications as covariates (Table 3).
Table 3
Multivariate analysis for detecting predictors of TBS levels
Generalized linear model for countinuous variables was used.
OR, odds ratio; CI, confidence interval; TBS, trabecular bone score; COPD, chronic obstructive pulmonary disease; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; BMI, body mass index; ICS, inhaled corticosteroid; OCS, oral corticosteroid; SCS, systemic corticosteroid.
![]()
When we applied a generalized linear model for identifying predictors for TBS levels in 138 patients with severe asthma, age (ORs, 0.997; 95% CI, 0.996-0.999; P < 0.001) and SCS dose for 1 year prior to the measurement (0.983; 0.970-0.997; P = 0.016) were significantly associated with lower TBS levels. However, severe asthmatics who had been prescribed ICS at least a fluticasone propionate dose equivalent to 180 mg over the previous year showed a significantly higher in TBS levels (1.057; 1.008-1.108; P = 0.021, Supplementary Table S1). Therefore, we compared clinical characteristics of severe asthmatics according to the ICS dose over the previous year between at least 180 mg and less than 180 mg. Significantly frequent OCS burst events were observed in severe asthmatics who used ICS less than 180 mg (5.56 ± 3.54 vs. 3.13 ± 4.10, P = 0.007), and both TBS (1.27 ± 0.15 vs. 1.32 ± 0.10, P = 0.038) and BMD (0.90 ± 0.15 vs. 0.98 ± 0.18, P = 0.041) levels were significantly decreased in those patients as compared with severe asthmatics used ICS ≥ 180 mg for the previous year. SCS doses for the lifetime (6.94 ± 9.48 vs. 10.04 ± 8.21, P = 0.132) and for 1 year prior to the index date (1.12 ± 2.11 vs. 1.65 ± 1.27, P = 0.231) tended to increase in patients who used ICS less than 180 mg over the previous year; however, no statistical significance was noted (Supplementary Table S2).
DISCUSSION
In this study, patients with severe asthma exhibited lower vertebral TBS values than those with either non-severe or non-active asthma or non-asthmatic subjects, whereas there were no significant differences in BMD among the study groups. As expected, TBS was significantly associated with exposure to higher SCS and ICS doses for 1 year prior to the measurement, even after controlling for age, sex, BMI and anti-osteoporotic medication use. TBS was also significantly correlated with FEV1 and methacholine PC20, suggesting that airway inflammation leading to airway obstruction and bronchial hyper-reactivity may impair bone quality in patients with active asthma. To our knowledge, this is the first study to demonstrate the potential utility of TBS to predict bone quality fragility in patients with asthma in comparison to BMD.
In addition to conventional risk factors for osteoporosis, inflammatory factors and treatment with corticosteroid may facilitate further bone loss in asthmatic patients.1819 Indeed, previous studies have shown that glucocorticoid therapy has deleterious effects on bone, resulting in an increased fracture risk.3 Although the detrimental effects on bone metabolism are assumed to be lower with ICSs, given their limited systemic absorption,20 evidence does suggest that patients with asthma undergoing ICS therapy are at risk for reduced BMD.16182122
The effect of ICSs on the BMD of patients with asthma has previously been investigated, although results are conflicting.141518212324 Many studies have identified significant reductions in BMD upon administration of ICS in patients with asthma.1416182122 Meanwhile, in other studies, ICS use for asthma was not associated with changes in BMD.152324 A recent meta-analysis revealed that ICS therapy in asthmatic patients was not associated with significant reductions in BMD in comparison to controls, and thus the authors concluded that ICS treatment for asthma can be considered safe.25 In the present study, we noted no significant differences in BMD among the study groups divided according to the severity or presence of asthma and severe asthma exacerbation, whereas TBS was significantly decreased in severe asthma patients and non-severe asthmatics with exacerbation. In other words, changes in TBS are more sensitive to asthma severity, experience of severe asthma exacerbation, and SCS and ICS doses compared to BMD.
In a recent cross-sectional study,26 a 14% higher prevalence of fractures was noted in asthmatic women than in non-asthmatic controls, despite no differences in the lumbar spine or the femoral neck BMD between cases and controls. Unlike postmenopausal osteoporosis, wherein both increases in bone formation and resorption occur, the increased risk of fracture associated with glucocorticoid treatment-induced osteoporosis cannot be fully explained by changes in BMD.12 Glucocorticoids cause decreased production of osteoblast precursors and increased apoptosis of mature osteoblasts.3 Histomorphometric studies have confirmed that decreased numbers of osteoblasts on trabecular bone in patients with glucocorticoid-induced osteoporosis are associated with thinning wall width.27 Altogether, these findings suggest that glucocorticoid treatment can significantly deteriorate bone quality, particularly in trabecular bone. In the same context, we found that patients with severe asthma and having taken higher dose of cumulative SCS over the previous year had a significantly lower TBS, whereas BMD levels were not associated with ICS use, SCS dose and number of OCS burst events in the present study. This suggests that TBS was more specific to detect an impaired bone quality by SCS or ICS treatment than BMD. Moreover, cumulative dose of SCS for the lifetime had no significant effect on the TBS levels. Deleterious effects of corticosteroids on bone metabolism were found to be observed soon after the start of steroid treatment with a rapid onset during the first 3 to 6 months and are dose-dependent.28
Low TBS values are perceived to be associated with poor microarchitectural bone quality, such as thinner trabeculae, low trabecular number, low connectivity density, low bone volume to tissue volume and high trabecular separation.29 A recent meta-analysis study demonstrated that TBS is a consistent and significant predictor of fracture risk, and provides information independent of the Fracture Risk Assessment tool in men and women from international cohorts of multiple ethnicities.30 Furthermore, previous studies have highlighted an association between TBS and the presence of fragility fractures in diseases with an altered bone structure, such as primary hyperparathyroidism, type 2 diabetes mellitus, and RA.1131 In a prior study,12 glucocorticoid-treated women had lower TBS values than glucocorticoid-naïve women, whereas their L-spine BMDs did not differ. In the present study, exposure to high SCS dose and severe asthma over the previous year were identified as independent predictors of a lower vertebral TBS in a generalized linear model even after controlling for age, SCS dose for the lifetime, comorbid diseases and anti-osteoporotic medication use. However, no significant correlation between BMD and ICS and SCS doses was found. Interestingly, TBS levels in controls and the other 3 groups of asthmatics, except severe asthma, differed significantly among age groups, although in severe asthmatics, no significant difference was noted in TBS levels between patients aged over 65 and 50-64 years. Therefore, clinicians should monitor TBS earlier to detect deterioration of bone quality and fracture risk in asthmatic patients, especially in severe asthmatics who had frequent OCS burst leading to increased risk of exposure SCS over the year. In analyses including all asthmatic patients, severe exacerbation and high dose ICS use were associated with reductions in TBS, but not in BMD. However, interestingly in severe asthmatics who had been maintaining ICS ≥ 180 mg (fluticasone propionate 0.5 mg/day for at least 12 months or 1 mg/day for more than 6 months) for the previous year, less OCS bursts and higher levels of TBS and BMD were found. Therewith, for severe asthmatics, using ICS ≥ 180 mg was suggested as a protective factor of TBS, while age and SCS dose for the previous year were also found to be risk factors of decreased TBS. Taken together, to increase adherence to ICS use for severe asthmatics, clinicians can reduce SCS exposure and lessen steroid effects on the bone quality. However, further studies to prove optimal ICS dose for achieving asthma control and for preventing from bone fragility in patients with asthma are still needed.
Currently, data on bone density in asthmatic patients are limited, and most studies have primarily focused on bone loss according to steroid treatment.16 Nevertheless, many factors indirectly related to asthma activity or its treatment, such as physical activity level and supplemental calcium and vitamin D intake in women, may differently affect bone metabolism.161932 Also, as airflow obstruction worsens, risk of osteoporosis increases because patients become more debilitated, less mobile, and nutritionally depleted.33 Systemic inflammation in asthma, including elevated levels of osteoclastogenic cytokines, such as TNF-α and IL-6, might have a detrimental effect on bone metabolism too.34 In the present study, TBS was also significantly correlated with FEV1 and methacholine PC20. Therefore, one could suggest that asthma itself might have an association with deterioration of bone quality.
There are some limitations in the current study. This retrospective cross-sectional study was performed only at a single university hospital. To overcome this limitation, we analyzed big data from electronic medical records, and enrolled a total of 627 asthmatics and the same numbers of age- and sex-matched controls. We applied operational definitions to classify severe and non-severe asthma primarily based on international guidelines.17 However, about half of asthmatic patients had been prescribed anti-asthmatic controllers less than 3 months during the study period. Therefore, we could not evaluate correctly the effects of ICSs on bone quality in these subjects defined as non-active asthma. In addition, as we collected data from patients who had taken BMD and TBS measurement, about 80% of patients were female and sex distribution among asthma groups are different from previous results. However, we adjusted sex as an important covariate for statistical analyses. We could not collect all subjects' data which could have possible effects on BMD or TBS such as smoking, alcohol drinking, daily activity and other chronic diseases. Even though patients in group 3 had been exposed to a higher dose of cumulative SCS for a longer period of time than those in group 4, no significant difference in TBS or BMD levels between these two groups was found. In addition, using anti-osteoporotic agents might have affected TBS of the subjects. Therefore, we adjusted the prescription of anti-osteoporotic agents as a covariate for statistical analyses to minimize its possible effects on the results. Moreover, the most common prescription of anti-osteoporotic agents were bisphosphonates in our study subjects (group 1: 72.4%, group 2: 73.7%, group 3: 55.4%, and group 4: 64.7%). Bisphosphonates are known to have a little effect on TBS. In the same context, TBS is not recommended for monitoring bisphosphonate treatment in postmenopausal women with osteoporosis by the International Society for Clinical Densitometry.35 Thus, we do not think that it affected the present results seriously to include the subjects on anti-osteoporotic agents. However, prospective studies are needed to determine TBS cutoff values with which to predict the exact fracture risk in asthmatics. Secondly, some laboratory parameters related to bone metabolism, such as bone turnover markers and serum vitamin D, could not be analyzed due to the lack of data. Thirdly, the existence of vertebral fractures was not evaluated due to the retrospective study design.
In conclusion, patients with severe asthma exhibited a lower vertebral TBS. Older asthmatics and patients with severe asthma and high SCS exposure for 1 year prior to BMD measurement were identified as significant and independent predictors of lower TBS in patients with asthma. In addition, TBS was also significantly correlated with airway obstruction and hyper-reactivity as well as ICS doses used over the previous year, which were not correlated with other BMD results. Physicians should pay additional attention to fracture risk in asthmatic patients being treated with high glucocorticoid doses, even if they have relatively normal BMD.
 XML Download
XML Download