

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The population of refugees is increasing globally. Mass media as well as researchers have termed this upsurge the contemporary refugee crisis. The numbers of refugees worldwide are at record highs. In the 2017 review of refugees' status,1 the office of the United Nations High Commissioner for Refugees (UNHCR) reported that about 68.5 million peoples were forcibly displaced worldwide. Of these 25.4 million people were international refugees and another 3.1 million were asylum-seekers. UNHCR estimated there were 44,400 new displacements every day during 2017. The majority of refugees came from Syria, Afghanistan, and South Sudan. In many countries, the constant influx of refugees has been the source of many political controversies.
The Republic of Korea (South Korea) is no exception to this global phenomenon. Korea became a signatory to the multilateral UN Convention relating to the Status of Refugees in 1993, and started receiving refugees in 1994. In 2013, Korea became the first Asian country to enact legislation regarding refugees. Though the legislation is regarded as reflecting the spirit of the UN convention well, the process of approving refugee status has been criticized as being too rigid and complex. Since 2010, the numbers of refugees and foreign nationals seeking asylum have increased sharply in Korea. There were 1,011 applications for refugee status in 2011, and 9,942 new applications in 2017. Of these, only 121 applicants were granted full refugee status, with another 318 granted humanitarian residence permits, a semi-refugee status, in 2017. From 2009 to 2017, there have been a total of 30,566 refugee applications, out of which only 692 people were granted full refugee status.2 With full refugee status, one can receive the same level of basic social protection as received by Korean nationals. On the other hand, with the annually renewable humanitarian residence permits, a semi-refugee status, one can work in Korea, but without the legal and social protection afforded by refugee status. The majority of refugee applicants at this time are undergoing the refugee approval process, and are regarded as asylum seekers. Having applied for refugee status, these people are approved to remain in Korea until the conclusion of the process, which can be as long as three or four years, with complex steps including appeals and possible trials. Most of these refugees and asylum seekers reside in urban communities, in this protracted situation involving their refugee applications and waiting. Such protracted situations are not uncommon worldwide.
There have been various studies of refugees' mental health worldwide. Most of which report higher levels of depression, anxiety, and post-traumatic stress disorder (PTSD).345678 One recent review estimates the prevalence of depression as between 5% to 44%, and from 9% to 36% for PTSD.9 In Korea, there is a great deal of literature regarding the mental health of North Korean Refugees (NKRs). A recent 10-year review reported 33%–51% prevalence of depression and 4%–52% of PTSD. Although there has been little attention paid to, or conventional research studies conducted on mental health of refugees so far, a study based on a survey of 72 refugees in Korea reported high anxiety, paranoia and depression. According to this study one third of the participants scored above the cut-off point on the screening of mental health problems.10
This study aimed to determine the current prevalence of possible depression and PTSD in a community of refugees (including applicants for refugee status and humanitarian residency permittees) and compare them with migrant workers not of refugee origin and Korean nationals surveyed in the 2016 Korean National Health and Nutrition Examination Survey (KNHANES).11
METHODS
Study subjects
The primary target population was a group of refugees residing around the Seoul and Gyeonggi province. We contacted major refugee communities, Non-Government Organizations (NGOs) and government facilities supporting refugees to recruit 129 refugees — including approved refugees, asylum seekers (refugee applicants), and humanitarian residential permittees. To compare their health and mental status, we set up two control groups. The first group comprised migrant workers, and shares many characteristics with the target group in terms of legal status and socio-economic conditions faced as unstable aliens in Korean society. We recruited 121 migrant workers, with no history of exile, from the charity NGOs providing medical and welfare support for them. The second comparison group comprised age and gender matched Korean nationals drawn from the KNHANES, with a ratio of 10 nationals per one refugee subject.
Survey method
We used the KNHANES 2016 questionnaire plus some additional demographic questions regarding refugee status and mental health questions regarding experience of trauma. We translated the questionnaire into 3 different languages — English, French, and Arabic, except where there already existed individual scales with multiple language versions. For those scales, we used standardized versions for each language. Those scales were EuroQol12 (EQ-5D), Patient Health Questionnaire-913 (PHQ-9) and Impact Event Scale-Revised (IES-R).1415 Trained interviewers who could speak the relevant languages interviewed the refugees and migrant workers using the questionnaire in the subjects' own neighborhoods, with support from NGO activists and community workers who were familiar with the subjects.
We also conducted focus group interviews with governmental officials and NGO/Non-Profit Organization (NPO) activists, social workers, and a priest engaged with refugees at various stages of their life in Korea. The results are summarized in Table 1. We focused on depression rather than PTSD in this study.
Table 1
Summary of focus group interviews with various governmental and NGO/NPO personnel engaged with refugee populations in Korea (n = 8)

Statistics
We compared the demographic information, quality of life, and mental health status between: refugees and age-gender matched Korean nationals, and refugees and migrant workers, mainly using χ2 tests. We defined the presence of possible depression as a score of 10 points or greater on the PHQ-9, and the presence of possible PTSD as having more than 33 points in IES-R. In addition, we made provisional diagnoses for major depressive disorder according to diagnostic algorithm in the PHQ.16 We conducted multivariate logistic regression to determine the odds ratio for depression with various social and health related factors. The IBM SPSS software platform (version 25; IBM Corp., Armonk, NY, USA) was used to conduct all statistical tests.
Ethics statement
The study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital, with IRB No. 1805-152-948. Informed consent was acquired from all study participants, in the language most familiar with them (English, French or Arabic). The process of receiving informed consents was assisted by trained interpreters and where possible, NGO community activists supporting them.
RESULTS
We interviewed 129 refugees in various stages in the refugee approval process, and 121 migrant workers residing in Korea. We also compared the refugee group with 1,290 age and gender matched Korean controls drawn from KHNANES 2016. Of the 129 refugees, 100 subjects were asylum seekers (applicants for refugee status), and 22 subjects were approved refugees. A further 7 subjects were classified as humanitarian residency permittees. Among asylum seekers, 9 subjects were in undocumented status (illegal stay). The 51.2% of the refugees group came from sub-Saharan Africa, and another 34.1% from the Middle East, whereas 74.4% of migrant workers were from Asia (Table 2). Of migrant workers, 51 subjects were undocumented foreign nationals.
Table 2
Countries of origin of study subjects

Of the refugee group, 72.1% were men, and 72.9% were younger adults below 40 years of age. About two-thirds of the refugees had more than 12 years of education, in contrast to 55.4% of the migrant workers. Only 17.8% of the refugees were in any kind of employment, compared to 49.7% of the migrant workers. In terms of formal health coverage, 93% of the refugees were outside any kind of the health coverage system, in contrast to 72.7% of the migrant workers. None of the refugees or migrant workers were eligible for any other social protection in Korea. More than 60% of the refugees had been in Korea over 1 year, and 54.6% had been in exile for 1–5 years (Table 3).
Table 3
Demographic profile of study subjects

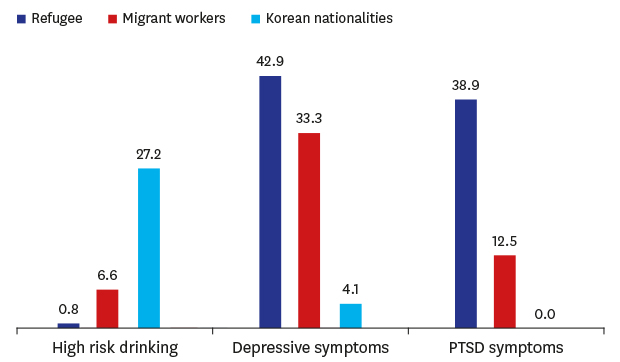
Table 4 shows selected mental health indicators of the study subjects. The refugees group showed more frequent suicidal planning during the past year than both migrant workers and Korean controls, but the only statistically significant comparison was between the refugee group and the Korean control group (3.1% refugees vs. 0.9% of Korean controls). Suicidal attempts during past year were also significantly more frequent among refugees than the Korean controls (0.8% vs. 0.2% of Korean controls). Interestingly, suicidal attempts in the refugee group were less frequent than in the migrant workers group (though this result also failed to achieve statistical significance). High risk drinking was much less frequent in the refugee group (0.8%) than in Korean nationals (27.2%) and the migrant workers group (6.6%). Possible depression was present in 42.9% of refugee subjects. This was significantly higher than in the Korean control group, but not significant when compared to the migrant workers group. Comparing the depressive status according to the severity category of PHQ-9, the refugee group more often exhibited severe symptoms than Korean nationals and the migrant workers group. Using the PHQ-9, we made provisional, syndromal diagnoses of major depressive diagnosis. For the refugee group, prevalence of possible major depressive disorder was about 16.7%, compared to 14.2% of the migrant workers group and 1.6% of the Korean control group. Differences between refugees and Korean control group were statistically significant (χ2 = 73.997; df = 1; P < 0.01, data not shown on table).
Table 4
Comparison of mental health indicators among refugees, migrant workers and the age and gender-matched general population in Korea

Korean controls are an age and gender matched subset from 2016 Korean National Health and Nutrition Survey, high risk drinking is defined by presence of an occasion, in which subject drink more than 7 drinks (5 if women) during last month.
PHQ-9 = Physical Health Questionnaire-9, IES-R= Impact Event Scale-Revised, PTSD = post-traumatic stress disorder, SE = standard error.
aP < 0.05 by χ2 test.
Presence of possible PTSD (measured by the IES-R) were also more frequent in the refugees group than in the migrant workers group (38.9% vs. 12.5%; χ2 = 22.237; df = 1; P < 0.01). Since no data regarding PTSD were collected through the KHNANES, we were unable to compare our results with the Korean control group. To observe the effect of staying in Korea on depression and trauma-related symptoms, we used Kruskal-Wallis H tests for mean scores of PHQ-9 and Impact Event Scale (IES) across the staying durations (Figs.1 and 2). There was no significant difference across the staying durations in PHQ-9 but the distribution of IES was significantly different, with highest mean scores in first 12 months of staying.
Fig. 1
Boxplot of PHQ-9 scores, according to duration of staying in Korea. No significant difference of distribution of PHQ-9 scores between groups by Kruskal-Wallis test (P = 0.08; df = 3; H = 6.698).
PHQ-9 = Patient Health Questionnaire-9.

Fig. 2
Boxplot of IES scores, according to duration of staying in Korea. Significant difference of distribution of IES scores between groups by Kruskal-Wallis test (P = 0.04; df = 3; H = 8.201). In pairwise comparison, Group I > Group II & Group I > Group IV.
IES = Impact Event Scale.

Half of the refugees reported their health status as good, significantly higher than both the Korean control group (32.3%) and the migrant workers group (34.7%). Nevertheless, the quality of life in the refugee group was generally worse than indicators of the Korean matched control group in all five domains of EuroQol. Domains that presented particularly greater frequency of problems were ‘Pain and Discomfort’ (54.3% vs. 14.3% for the Korean control group) and ‘Anxiety and Depression’ (54.3% vs. 4.7% for the Korean control group). When compared to the migrant workers group, the refugees group showed significant difference only in the anxiety and depression domain of EuroQol (54.3% vs. 36.4%). Refugee group also have significantly frequent non-health related activity restriction than migrant workers group (65.9% vs. 35.6%) (Table 5).
Table 5
Comparison of life quality and functional restrictions among refugees, migrant workers and the age and gender-matched Korean nationals

To determine the odds ratio for depression and PTSD among various risk factors, we conducted multivariate logistic regression analysis (Table 6). Only traumatic event before entering Korea was a significant risk both in possible depression and possible PTSD. All other socio-economic and health related factors were insignificant, except lower risk of possible depression in the 31–40 years age group (than 18–30 years group).
Table 6
Multivariate logistic regression analysis of risk factors of depression among refugee participants

DISCUSSION
We found high rates for depression and PTSD among refugees seeking asylum in Korea. Prevalence of both diagnoses in our study are higher than findings from a systematic review of refugee studies of other nations from the previous decade,17 which reported 5% prevalence of depression and 9% prevalence of PTSD. But recent reviews have reported high prevalence estimates similar to our findings.918 There are some studies reporting higher prevalence of PTSD, as high as 84%, but one of these studies was conducted in a refugee camp,19 rather than in community, and another included only small numbers of subjects (n = 25).5 The rate of mood and anxiety problems are also similar with that of NKRs (or North Korean defectors) who have settled in Korea, whose prevalence estimates are 33%–51% for depressive symptoms and 43%–53% for anxiety symptoms.20 For PTSD, a study using IES scale reported 40% prevalence among NKRs,21 which is in line with our study, but another study using diagnostic interviews like Structured Clinical Interview reported 5% prevalence of PTSD among NKRs.22
The prevalence of mental health problems among refugees in Korea is much higher than that in the general population, as expected. This is in line with findings around the world. For the general adult population of Korea, a study using KNHANES data reported 6.7% prevalence of depression with the PHQ-9 score of more than 10,23 and a nation-wide psychiatric epidemiologic study conducted in 2011 reported 3.1% 12-month prevalence of major depressive disorder.24 Globally, data from World Mental Health Survey initiative indicated 5.5% 12-month prevalence of major depressive episodes in ten high income countries and 5.9% in eight low-to middle-income countries in 2011,25 and a systematic review report put the prevalence of major depression at 4.7% (4.4%–5.0%) in 2013.26 For PTSD, the 12-month prevalence among general adult Koreans was reported as 0.6% in 2011,24 and global 12-month prevalence from World Mental Health Survey Initiative was 1.1% (0.2%–3.8%).
The refugee population of Korea shares many similarities with the migrant workers, especially undocumented migrants, since they are filling the same low-income jobs available to foreign nationals and have many similar uncertainties and instabilities in their life circumstances. Still, the refugee group showed more serious mental health problems. Prevalence of possible depression determined by the PHQ-9 were not significantly higher in refugees, but when narrowed down to possible major depressive disorder, the difference was statistically significant. In quality of life measure, refugees have much greater problems with anxiety and depression than the migrant workers do, but we could not find any significant differences in the remaining four domains.
It is of note that although the refugees reported much greater frequency of suicidal planning during the past year, as well as higher frequency of depression, actual suicide attempts were less frequent among refugees than both the general population and the migrant workers, though this result was not statistically significant. It is also worth noting that high risk drinking was significantly less frequent in refugees than in both the general population and the migrant workers. We think that these results reflect the cultural and religious backgrounds of refugee subjects. The refugee group in our survey contained high number of Muslims among them, but the migrant workers group were mainly from East Asian countries with little Muslim representation. Religions in general are said to be protective against suicide, and there is some research that Islam is related to lower rates of suicide.27 Moreover, as Islam explicitly forbids consumption of alcohol, there are studies that report lower alcohol consumption in Muslims even in a county that does not forbid drinking.28
In our study, out of several demographic and health related factors, only the traumatic event before entering Korea was a significant risk factor for possible depression. This combined with the results that while possible PTSD decreases following the time staying in Korea, possible depression does not, indicates the traumatic experience before arriving in Korea is a very important mental health risk, not just for PTSD but also for depression, and indicates the management of trauma is important in treating depression among refugee population. This also explains the higher, although not statistically significant, prevalence of possible depression of refugees over migrant workers, who share many similar socio-economic characteristics regarding life in Korea.
Another interesting result of this study was the change of mental problems over time. In contrast with depressive symptoms that stay relatively stable regardless of the duration of stay, PTSD symptoms are the most severe in the first year and reduce afterwards. This implies that mental health service to refugees should be precisely designed to mitigate the distress from traumatic events in a timely manner.
It is of note that the result of our study does not include being women as a risk factor for both possible depression and PTSD. Especially studies from subjects of refugee camps indicate that being women is an important risk factor for both PTSD and depression.6819 This might be because our subjects are from the urban community, and not from refugee camps.
One major limitation of our study is that our sample consisted of subjects with heterogeneous ethnic and cultural backgrounds. So, for more accurate estimates of prevalence of mental health problems among the refugees in Korea, future studies should recruit more subjects from each ethnic background. And our study sample is a convenient sample, with subjects recruited from established refugee communities and governmental/NGO facilities. This might result in the failure to include the more vulnerable subjects who are not in touch with supporting groups or facilities. Indeed, the refugee communities we surveyed for this study consisted of stabilized refugees living in urban environments, but one NGO facility included in this study was a provider of emergency shelters for more vulnerable refugee population, so our sample can be regarded as balanced as possible, since the nature of a refugee population make it very difficult to conduct random samplings. But as the refugee populations are growing rapidly in Korea, we think a study with a more robust sampling method should be conducted hereafter.
Another limitation of this study is that we did not collect information about history of mental health issues and lacked information regarding the nature of trauma they experienced. A few studies regarding Syrian refugees reported that an important risk factor is a history of past mental health problems.1929 The intrinsic vulnerability of a person could interact with traumatic experiences and socioeconomic risk factors, and therefore, would explain much of the depression and other mental health issues seen in refugees. In addition, knowing what kind of traumatic experiences lead to mental health problems would enable more efficient intervention.
In spite of its limitations, this study shows the high burden of mental health problems among refugees and refugee applicants in Korea, even when compared with migrant workers. Mental health problems can interfere with adaption within the new environment in Korea, at least for those with syndromal level symptoms of major depression and high level of symptoms related to the PTSD. Without intervention, worsening, and chronicity of mental health issues could easily lead to greater disability, and worsen the already prevalent prejudice and stigma against refugees. Appropriate, early, mental-health screenings, with culturally acceptable and timely interventions for those at-risk would efficiently reduce the social cost related to the refugees.
 XML Download
XML Download