

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Several methods12345678910 have been suggested as more esthetic alternatives to orthodontic brackets. A nickeltitanium (NiTi) archwire can be bonded directly to the lingual side of the anterior teeth with composite resin, in order to correct minor crowding.2 NiTi wires can also be used with or without simple tubes to resolve crowding.23 A simple tube is a generic term for various tubes without bonding bases that can be bonded to the tooth by covering the tube with flowable resin. A mini-tube appliance10 is the first simple tube manufactured for alignment of the anterior teeth. Alternatively, a small crimpable mini stop, which is used for holding a NiTi archwire, can also be used as a simple tube when crimping is not applied. The most important potential benefit of this approach is increased ease of oral hygiene care, due to the reduction of undercut areas underneath the simple tubes.11 Furthermore, patient comfort may be increased due to the small size and low profile of the simple tube.
However, simple tubes are used mainly with unbent superelastic NiTi archwires,10 because a bent wire cannot be inserted through the openings of the tube. Therefore, adjustments of tooth position are typically performed through repositioning of simple tubes, rather than wire bending. To reduce the repositioning of simple tubes, customized composite resin covering that holds the simple tube can be made by injecting flowable resin into the mold formed inside of the customized transfer tray, then applying light curing. This case report illustrates the method of fabricating customized resin coverings using a virtual setup, computer-aided design (CAD), three-dimensional (3D) printing, and fabrication of transfer tray.
DIAGNOSIS AND ETIOLOGY
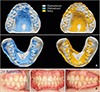
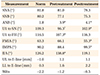
A 17-year-old male presented with the chief complaint of crooked anterior teeth. He exhibited a convex profile, and intraoral examination revealed palatal eruption of the maxillary left lateral incisor without transverse shift of the maxillary dental midline. The mandibular right lateral incisor had erupted lingually, and the dental midline was shifted 2.5 mm to the right. Crossbite was present in the areas of the maxillary left lateral incisor and mandibular right canine. The right and left molars exhibited Class I relationships. Pretreatment panoramic radiographs showed a favorable tooth axis and normal root length. Cephalometric analysis revealed a mild Class II skeletal pattern with retrognathic mandible. The maxillary incisors were tipped lingually, and there was a normal relationship between the esthetic line and the lip (Figure 1, Table 1). The suspected etiology of crowding was typical tooth size-arch length discrepancy.
TREATMENT OBJECTIVES
The treatment objectives were as follows: decrowding without severe proclination of incisors, and establishment of normal overbite and overjet while maintaining Class I canine and molar relationships.
TREATMENT ALTERNATIVES
Because the facial profile was favorable and the molar relationships were Class I, there was no consideration of orthognathic surgery to improve the retrognathic mandible, or premolar extraction treatment to improve the convex profile. Therefore, nonextraction treatment was chosen; interproximal reduction was also planned to avoid severe flaring of the incisors during the alignment process. Because posterior occlusion was good, anteroposterior movement of the posterior teeth was not needed. Therefore, fixed appliance using simple tubes was chosen, with the potential benefit of reducing the possibility of decalcification during orthodontic treatment.11
TREATMENT PROGRESS
Silver tubes with 2- or 3-mm widths (Hubit Co., Ltd, Uiwang, Korea) were used as simple tubes. These tubes have an inner diameter of 0.46 mm (0.018 inches [in]) and an outer diameter of 0.71 mm.1 A pretreatment model was scanned to fabricate a digital model; then, digital setup was performed using setup software (Maestro 3D Ortho Studio; AGE Solutions, Pontedera, Italy). Stereolithography files of the setup model were imported into 3D CAD software. In the maxillary arch, double simple tubes consisting of a 3-mm wide occlusal tube and a 2-mm wide gingival tube were designed to control tooth positions in three dimensions. In the mandibular arch, only occlusal simple tubes were designed because torque control was not required. Occlusal and gingival simple tubes and customized resin coverings holding the central portions of occlusal tubes were designed on the setup models. For the gingival simple tubes, only recesses in which the gingival simple tubes would be placed were modeled during the design of customized resin covering, in order to allow freedom for adding gingival simple tubes later when necessary (Figure 2). These recesses were modeled by subtracting the gingival simple tubes from the customized resin covering. Customized resin coverings and simple tubes that had been designed from the ideal setup were transferred to the pretreatment digital model. These were then merged with the pretreatment digital model and produced using a 3D printer (D35; Prodways, Les Mureaux, France). By thermoforming the transfer tray on this printed model, the negative forms of simple tubes and customized resin domes were made in the transfer tray. In the left half of the maxillary model, Vaseline® was applied to the recesses designed for the gingival tubes; gingival simple tubes were then placed on these recesses and fixed with flowable resin (Filtek Z350 XT; 3M ESPE, St. Paul, MN, USA) before thermoforming (Figure 2). A transfer tray was then thermoformed with 1.0-mm Bioplast® (Scheu Dental, Iserlohn, Germany). Gingival simple tubes fixed with flowable resin were automatically transferred into the transfer tray through the process of thermoforming. The occlusal simple tubes were manually inserted into the holes for the mesiodistal ends of tubes formed on the transfer tray (Figure 2). The resin used to fix the gingival simple tubes was sandblasted, cleaned, and then treated with plastic conditioner (Reliance Orthodontic Products, Inc., Itasca, IL, USA).
After preparing the tooth for indirect bonding (i.e., oral prophylaxis, etching, washing, drying, and application of bonding agent), flowable resin (Filtek Z350 XT) was injected into the recesses for the resin coverings in the transfer tray. Flowable resin was also applied on the tooth side surfaces of resin coverings for gingival simple tubes, after application of the bonding agent. Then, the tray was securely positioned over the arch and cured using a light curing unit. Because crossbite was present on the maxillary left lateral incisor, the 0.013-in copper NiTi archwire (Ormco, Brea, CA, USA) that was inserted into the occlusal simple tubes bypassed the maxillary left lateral incisor. Instead, a 0.013-in copper NiTi wire segment was inserted on the gingival simple tubes of the maxillary left central incisor, lateral incisor, and canine (Figure 3).
When applying simple tubes to the whole arch, an archwire can be inserted between the canine and first premolar, where there is a large inter-tube distance; both anterior and posterior teeth are approachable from this area. Alternatively, a NiTi archwire can be inserted from the distal opening of a molar tube, while holding the opposite end with a mosquito to prevent poking soft tissues.
After 2 months of alignment, interproximal reduction was performed between the maxillary right lateral incisor and canine, and the mesial and distal sides of the maxillary left first premolar. An occlusal simple tube was also bonded onto the maxillary left lateral incisor (Figure 3). In the maxillary arch, 0.016-in NiTi (Sentalloy; Dentsply sirona, York, PA, USA) was used for the main archwire; a 0.013-in copper NiTi wire segment was maintained for the gingival simple tubes. In the mandibular arch, 0.013-in copper NiTi was used first, followed 3 months later by 0.016-in NiTi. During bite jumping of the maxillary left lateral incisor, blue bite-raising resin (Bisfil™ Core; Bisco, Schaumburg, IL, USA) was bonded onto the maxillary molars, in order to reduce occlusal interference on the maxillary left lateral incisor (Figure 3). After 5 months of treatment, the crossbite of the maxillary left lateral incisor was nearly resolved. Because the torque control of the maxillary lateral incisor (using the main occlusal archwire and the gingival wire segment) was unsuccessful due to the short distance between the two wires, and because the wires exhibited an unaesthetic appearance, gingival simple tubes were debonded and lingual simple tubes were bonded directly onto the maxillary left central incisor, lateral incisor, and canine. For this bonding procedure, simple tubes were inserted on a 0.013-in copper NiTi wire segment before bonding. Lingual simple tubes were bonded passively on the maxillary left central incisor and canine; the simple tube for the maxillary left lateral incisor was then positioned more occlusally, in order to exert labial root torque on the lateral incisor (Figure 3). This bonding procedure is known as “deflection-based bonding,”12 because a wire is deflected as needed during this bonding procedure; this differs from the conventional bracket bonding procedure, in which brackets are bonded in their ideal positions in contact with tooth surfaces. Lingual simple tubes on the lateral incisor were positioned along a circle established with the labial simple tube as its center; its radius comprised the distance between labial and lingual simple tubes (Figure 3). After 8 months of treatment, orthodontic appliances were removed, and maxillary and mandibular fixed retainers were bonded (Figure 4).
RESULTS
Superimposition of the pretreatment and posttreatment cephalometric radiographs revealed mild labioversion of both maxillary and mandibular incisors (Figure 4). A posttreatment panoramic radiograph showed no significant root resorption. Superimposition of pretreatment and posttreatment digital models13 revealed that the alignment was completed with mild arch expansion (Figure 5). Superimposition of the digital setup model and posttreatment model showed a high degree of similarity between the models, except that the intercanine width was wider in the posttreatment model (Figure 5).
The treatment results were stable after 2 years of retention. However, gingival recession was evident on the maxillary left lateral incisor (Figure 5). This could have been caused by the rapid movement of the root into the buccal cortical bone. Slower movement of the maxillary left lateral incisor might have reduced gingival recession.
DISCUSSION
The limitations of bracketless or bracket-free12345678910 orthodontic treatments are similar to those of treatment using two-dimensional (2D) brackets.1415 These methods use only round wires. Unlike 2D brackets, simple tubes can receive only superelastic NiTi wire without any sharp bends, which limits the indications for treatment using simple tubes, compared with those for treatment using 2D brackets. Control of tipping and rotation of teeth is also difficult when using simple tubes with narrow width. Therefore, use of simple tubes of > 3 mm width is recommended, unless severe crowding is observed. Another limitation of this treatment method is that rectangular or heavy wires cannot be used; thus, space closure and key correction are impossible, and torque control is difficult. Therefore, only mild Class I or relapse cases can be treated with this appliance. Although the indications are limited, patients who prefer treatment using a clear aligner for aesthetic reasons frequently accept this alternative approach using simple tubes.
To overcome these limitations, double wires can be used. In the present case, labial archwire and lingual wire segments were used to apply labial root torque to the maxillary left lateral incisor (Figure 3). In this application, the maxillary left lateral incisor had been constrained with thicker and stiffer labial archwire. The occlusally-deflected lingual wire segment generated an intrusive force passing through the lingual side of the center of resistance of the maxillary left lateral incisor, thus producing a moment for labial root torque (Figure 3).
Decalcification occurs frequently in orthodontic patients with poor oral hygiene. Bracket wings and hooks can act as a trap or reservoir for food debris and dental plaque. In addition, orthodontic appliances disturb the salivary flow field on tooth surfaces and can lead to reduction in salivary velocity and increased bacterial numbers.8 Local vortexes that form in areas gingival to the bracket, together with the constraint of narrow space, contribute to a periodontal inflammatory response.8 When 0.71-mm-thick simple tubes are bonded with dome-shaped customized resin coverings, the self-cleansing action of the salivary flow is less affected than when using brackets. When poor oral hygiene is observed during fixed treatment using brackets, simple tubes can be used to replace the brackets after completion of the space closure or key correction. Rotation and extrusion are difficult to achieve with clear aligners.1617 Simple tubes can be used in combination with clear aligners to achieve tooth movements that are difficult to realize with aligners.16 Currently, the fabrication process for customized resin covering is technique-sensitive and time-consuming. Therefore, direct application of simple tubes may be more practical. However, as 3D CAD18 and 3D printing technologies continue to advance, the present approach may evolve and its indications are likely to broaden in the future with an additional use of auxiliary wires or aligners. Hopefully, this is helpful for patients who is reluctant to accept the fixed appliance treatment using brackets, thus broadening acceptance of orthodontic treatment.




 XML Download
XML Download