

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Transcatheter device closure of a secundum atrial septal defect (ASD) is advised as the principal treatment choice because of its proven efficacy and reliability, resulting in fewer complications and reduced hospitalization periods, as compared to surgical ASD closure.1)2)3) Percutaneous ASD closure has been established as a trustworthy procedure with minimal risk as a byproduct of the evolution of reliable device properties, as well as the accumulation of informed experience in and technological advancement of the procedure.
The optimal device should be readily positionable, facilitate complete closure with minimal risk of embolization, and use a delivery technique with safe retrieving and redeploying qualities.4) Additionally, it must be patient-friendly, facilitate rapid re-endothelialization, and be biocompatible and suitable for treating a wide range of defect characteristics. Globally, various kinds of nitinol-wire-mesh devices are mostly used nowadays, but there are only a few approved devices in Korea. The Amplatzer® septal occluder (ASO; St. Jude Medical Inc., Plymouth, MN, USA) has been used most prevalently with favorable follow-up results, including unique structural features to recapture and redeploy the device before release, i.e., a self-centering mechanism.2) The Occlutech Figulla® Flex II device (FSO; Occlutech GmbH, Jena, Germany) is a relatively novel nitinol double-disk occluder with similar construction and implantation procedures to those of the ASO. Although the first generation Occlutech Figulla® septal occluder received Conformité Européenne (CE) approval during the mid-to-late 2000s and has been implemented worldwide, there are no existing data in the literature about the use of this device in Korea.5)6)7)8)9) The Gore® Cardioform septal occluder (GSO; W.L. Gore & Associates, Flagstaff, AZ, USA) is a non self-centering device that replaced the Helex device made by the same company and received CE approval in June 2011. Because it is acknowledged for its flexibility with minimum metal content and soft disk with less frictional forces against erosion, the GSO was introduced to the Korean domestic market in May 2015.
The aims of this retrospective study were to describe our early to mid-term experience with transcatheter ASD closure using the FSO and GSO, and to compare three kinds of ASD closure devices: the ASO, FSO, and GSO in a single tertiary center.
METHODS
From September 2014 to August 2016, 267 patients underwent transcatheter ASD closure with an ASO (n=98, 36.7%), FSO (n=152, 56.9%), or GSO (n=17, 6.4%). We performed a retrospective comparative review of these patients' data.
Indications
Indications for transcatheter ASD closure include single or multiple ASDs with symptoms, a hemodynamically significant defect (right atrial and right ventricular enlargement in addition to calculated pulmonary blood flow-to-systemic blood flow [Qp/Qs] ratio >1.5) obtained from catheterization data, or suspicion of a paradoxical embolism (excluding other causes such as stroke or recurrent transient ischemic attack).10) In general, a sufficient septal rim should surround an ASD >5 mm in all directions. Although rim deficiency may potentially increase the risk of complications such as device embolization, erosion and encroachment of device onto nearby cardiac structures, most ASDs with deficient rims were closed successfully and included in this study.11)12) The exclusion criteria were as follows: any associated complex congenital heart disease or other types of ASDs (e.g., sinus venosus and ostium primum defects), bleeding disorders, and any contraindication to antiplatelet therapy, active systemic infection, and intracardiac thrombus.
The devices
The ASO (Figure 1A), constructed from nitinol wire, is braided into a cylindrical mesh, and it is a self-expanding, double-disk device with a self-centering mechanism that is repositionable and recapturable. As this device has been extensively tested over the years, all conceivable strengths and potential limitations have been thoroughly discussed in detail; thus, the solutions for arising issues have been fully refined. Among all issues to consider, cardiac erosion has become a significant one, as it can be fatal and sometimes have a delayed onset in patients.13)
 | Figure 1Devices used for atrial septal defect closure. (A) Amplatzer® septal occluder; (B) Occlutech Figulla® Flex II; (C) Gore® septal occluder.
|
The FSO (Figure 1B) is the third-generation Occlutech device for ASD closure with a flexible titanium oxide-coated nitinol mesh and a double-disk system similar to that of the ASO, but with distinct structural modifications that make it a more desirable option. This device features minimal material, no hub on the left atrial disk, and a small clamping hub on the right atrial disk. Additionally, this contraption has an adjustable delivery system and soft braiding with a biocompatible titanium oxide surface.6)14) The disk is available in different sizes, ranging from 4 to 40 mm, with 1–1.5-mm increments between 4 and 21 mm and 3-mm increments between 21 and 39 mm and 40 mm. Unfortunately, it requires a slightly heavier delivery sheath than do conventional ASO devices and has relatively limited size options (FSO vs. ASO: 20 sizes vs. 27 sizes).
The GSO (Figure 1C) is a non-self-centering double-disc device that has a platinum-filled nitinol wire frame, which is enclosed in expanded polytetrafluoroethylene that can malleably align with atrial septum.3) The GSO is available in device sizes from 15 to 30 mm in 5-mm increments and delivered using a standard delivery system, which makes the device repositionable and retrievable. It is generally recommended that the device size should be more than twice the defect size and the GSO is not suitable for defects over 18 mm due to the non-self-centering feature.
Procedure
The implantation technique was similar for all devices and performed by one operator. First, hemodynamic study and assessment of morphologic characteristics of the defect were performed by cardiac catheterization. Femoral venous access was obtained, and a right heart study was performed to measure right heart pressures and calculate the Qp/Qs. Generally, the procedure is conducted under local anesthesia or deep sedation with spontaneous respiration with intracardiac echocardiography (ICE) guidance for device implantation. ICE evaluation includes the size and position of the defect and its anatomic relationship to the adjacent cardiac structures, including the vena cava, atrioventricular valves, coronary sinus, and all pulmonary veins.15)
Patients received intravenous heparin (60–100 IU/kg for children and 5,000 IU for adults) at the beginning of the procedure. The activated clotting time was maintained between 200 and 300 seconds to prevent thrombosis during the procedure.
The device was selected based primarily on the measurement of the defect's stretched diameter, which was determined using a compliant balloon catheter (sizing balloon catheter, St. Jude Medical or Nu MED, Inc., Nicholville, NY, USA) placed across the defect and controlled by color Doppler ICE, with the stop-flow technique. The stop-flow diameter (SFD) which is measured from a perspective view of both fluoroscopy and ICE is recommended as the standard measurement to avoid oversizing.16) In self-centering devices such as the ASO, the recommended device size is the same or slightly larger (<2 mm) than SFD. Nevertheless, the selection for device size was individualized considering deficiency of rims, spatial relationship with nearby cardiac structures and size of the heart. In cases of aortic rim deficiency, the usual recommendation is to avoid an “oversized” device because of the potential risk of erosion.16) Then, the appropriate delivery sheath was advanced into the left atrium over a guidewire previously placed in the left upper pulmonary vein. A loader for the FSO/ASO, first flushed in saline, assisted in positioning the occluder within the delivery sheath. The connection to the delivery sheath became attainable after de-airing the delivery sheath in water to eliminate the risk of air embolism. The device positioning techniques were similar with both devices, and the ICE and fluoroscopy devices were used to verify correct positioning. When the placement was judged as satisfactory, the occluder was released completely.
The patients were prescribed aspirin (5 mg/kg, maximum 100 mg) daily for 6 months, and transthoracic echocardiography was performed at 1 month, 3–6 months, and 12 months after implantation during follow-up. Residual shunting was defined on color Doppler imaging as trivial (<1 mm color width), small (about 1–2 mm color width), moderate (about 2–4 mm color width), or large (>4 mm color width).14)
Statistical analysis
All analyses were performed using SPSS 22.0 (IBM Corp., Armonk, NY, USA). The results are expressed as the mean±standard deviation (SD) and range. Differences between outcomes of the three devices were analyzed using the unpaired Student's t-test or by variance analysis as appropriate. A p value ≤0.05 was regarded as statistically significant.
Ethics statement
This study was approved by the Yonsei University College of Medicine Institutional Review Board and Research Ethics Committee of Severance Hospital (study approval number: 4-2017-0743). The requirement for individual consent was waived because of the retrospective nature of this study.
RESULTS
Patient characteristics
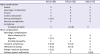
Patient characteristics and hemodynamic data are presented in Tables 1 and 2, respectively. Most of the patients had progressive and/or significant right heart enlargement when they had device closure. Patients with multiple ASDs accounted for 16.1% (43/267) of all patients. No significant differences were observed among the groups in the sex ratio, weight, and body surface area. Patients in the GSO group had the youngest average age of 20.0 years (SD 21.7 years, median 23.7 years, range 0.6–68.7 years). Twenty-eight (18.4%) patients in the FSO group and 5 (29.4%) in the GSO group weighed <15 kg.
Table 1
Patient characteristics in all three device groups

Data are presented as median (range) or mean±standard deviation, unless otherwise indicated. Bolded values indicate statistically significant differences.
ASO = Amplatzer® septal occluder; BSA, body surface area; FSO = Occlutech Figulla® Flex II; GSO = Gore® septal occluder.
*Small children defined as patients weighed <15 kg.
![]()
Table 2
Hemodynamic data and defect characteristics in all three groups

Data are presented as median (range) or mean±standard deviation, unless otherwise indicated. Bolded values indicate statistically significant differences.
ASO = Amplatzer® septal occluder; FSO = Occlutech Figulla® Flex II; G = grade; GSO = Gore® septal occluder; mPAP = mean pulmonary artery pressure; MR = mitral regurgitation; PAH = pulmonary arterial hypertension; Qp/Qs, pulmonary blood flow-to-systemic blood flow ratio; TR, tricuspid regurgitation.
*Pulmonary arterial hypertension was defined as ≥25 mmHg of mean pulmonary artery pressure.
![]()
The defect size of 11.9 mm (SD 8.8 mm, median 16.8 mm, range 5.0–16.0 mm) and Qp/Qs ratio were lower in the GSO group than in the other two groups (p=0.027). However, the ratio of ASD size to body surface area was not different between the three groups. The prevalence of defects with retro-aortic rim deficiency was the highest for FSO which was 83.6% (n=127), in ASO it was 58.9% (n=58) and in GSO it was 47.4% (n=8). Patients with pulmonary arterial hypertension, defined as ≥25 mmHg of the mean pulmonary artery pressure, comprised 13.1% (n=20), and this proportion was similar to those in the other two groups. Tricuspid regurgitation more than grade 2 and mitral regurgitation more than grade 1 were found in 19 (12.5%) and 8 (5.5%) patients in the FSO group, respectively.
Procedural data
The results of device implantation are presented in Table 3. The follow-up duration was a median of 2 years (range 13–37 months) in 267 patients. Among the three groups, the procedural success rate was 100%, and major complication rate was <1%. In the FSO group, 1 (0.9%) patient exhibited complicated complete atrioventricular (AV) block that occurred several hours post-procedurally. Despite adequate medical treatment, the complete AV block remained until the device was removed by percutaneous retrieval; the patient later underwent surgical ASD repair. In the ASO group, 1 (1.0%) case of device embolization occurred for a 40-mm large ASD after device placement in the cardiac catheterization laboratory. This device was retrieved percutaneously without any further complications, and the patient underwent surgical ASD repair.
Table 3
Procedural variables and follow-up outcomes in all three device groups

Data are presented as number (%), unless otherwise indicated.
ASO = Amplatzer® septal occluder; FSO = Occlutech Figulla® Flex II; GSO = Gore® septal occluder.
![]()
There were 2 (1.4%) cases of access site hematoma and 5 cases of minor complications in the FSO group, which were comparable to the findings of the other two devices (Table 4). Three (1.9%) patients had transient arrhythmia, 2 patients had atrial tachycardia, and 1 patient had paroxysmal supraventricular tachycardia. No patients required further treatment, and all patients were spontaneously converted to normal sinus rhythm. One (5.8%) case of delivery system malfunction was noted in the GSO group. Among all the devices, there was no case of mortality, significant neurologic complication, erosion, or late embolization.
Table 4
Complications during the follow-up in all three device groups
Data are presented as number (%).
ASO = Amplatzer® septal occluder; AV = atrioventricular; FSO = Occlutech Figulla® Flex II; GSO = Gore® septal occluder; TIA = transient ischemic attack.
![]()
DISCUSSION
Currently, transcatheter device closure of ASDs is widely accepted as the standard method of treatment for suitable ASDs.17) The ASO is one of the most predominantly used devices for closing ASDs, and it has been proven highly auspicious with minimal risk in the long term for the past two decades. Despite many of the ASO's undeniable advantages, cardiac erosion, a rare but serious complication, has been reported to occur in 0.043% to 0.3% of patients, which is why it should be considered an increasingly important concern.18) The likelihood for erosion to occur has been conclusively identified to be associated with oversized devices and deficiency of any rim; however, the specific mechanisms for device erosion remain obscure.16)18) This issue has far-reaching consequences under a rare complication rate; hence, pursuing the ideal device while considering all safety precautions has become a task of utmost priority in order to counteract the limitations of current devices.
Some important structural innovations have caused the increased use of the FSO, primarily its unparalleled adaptability and minimization of implanted material quantity.19) In contrast to the ASO, the FSO has a minimal amount of material with no hub on the left disk, so it has greater flexibility and reduces the trauma risk and clot formation in patients.5) Additionally, this device has a unique release mechanism resembling that of a bioptome with flexible angulation (from a range of 45° to full circular motion between the device and delivery cable). Because of these convenient features and its exceptional design, the device has softer braiding than the original Amplatzer® device; therefore, it can conform to the defect anatomy and reduce the risk of erosion.4)
There are several reports on the universal use of the FSO for ASD closure that show comparable and encouraging results in favor of its use. Roymanee et al.20) published a comparison between the FSO and ASO in 149 patients: there was a slightly higher success rate with the FSO (97.4% vs. 94.4%), and the median fluoroscopic time in the FSO group was shorter (ASO 13.7 minutes vs. FSO 9.0 minutes), even despite the larger ASDs in this group. Godart et al.14) compared the second and third generations of the Figulla® ASD occluder (n=31) with the ASO (n=100) in 131 patients, and concluded that the ability of the FSO to effectively and thoroughly resolve transcatheter ASD is commendable. According to current studies, including a registry report of Occlutech device use in 1,315 patients by Haas et al.,19) there was no case of erosion, which is similar to the results shown herein. Most reported erosions with the ASO are due to the use of oversized devices in rim-deficient patients, which is why the FSO may be preferred to the ASO because of its flexibility and reduced shear force.
Regarding device embolization, 1.1% of cases occurred during implantation and 0.4% occurred during the follow-up.19) The majority of the defects showed no rim, and they demonstrated an increased risk for device embolization when balloon sizing was not performed. There is still a prevailing necessity for further discussion regarding the differentiating factors of the devices and the risk for embolization. However, during deployment, the left atrial portion has a round, ball-like shape unlike the flat profile of devices with a double-sided hub. This prevents prolapse of the left disk during implantation, particularly in large ASDs, those without a rim, or those with a minimal aortic rim.21) In our study, a deficient retroaortic rim was also highly prevalent but not associated with an increased risk of technical failure or early adverse events.22)
Our study is innovative since it is the first to report the early to mid-term outcomes of using the FSO to close secundum ASDs in Korean patients, even including small children. The device handles very well and can be recaptured after deployment of both disks; thus, it can be repositioned easily. The third generation of the FSO has a lower profile than the previous generation, which proved itself indispensable in expanding its indications in smaller children. Our rate of 18.4% (28/152) of small children (<15 kg), patient and ASD characteristics, and rate of complications were comparable to findings of a multicenter series performed by Haas et al.,19) who reported a rate of small children of 7.1% (94/1315). In our study, technical success was achieved in 100% of cases, and complications occurred in a mere 3.5% (1/28) of all small children.
The GSO has been continuously available for interventional ASD closure in the European market since 2011, and it has achieved feasible, effective implantation in patients with ASD.3) This device is preloaded as a package device with the whole delivery system that has been modified for improved ease in delivery and positioning.23) The GSO has a soft patch-like double disk with fewer frictional forces, which is a preventive feature against erosion. Initial studies suggested that the GSO has potential benefits in safety, efficacy, repositionability, and the ability to recapture the viewpoint. The overall closure rate of ASD closure by the GSO was reported as 95.4% in 206 patients over a 20-month follow-up period. No erosion or perforation event was noted.3) Because of these advantages, the GSO device was expected to perform well in smaller defects especially with deficient retro-aortic rims, those in small children, or multi-fenestrated defects, when covering most of the atrial septum is necessary.11) In our study, although there were few patients in GSO group (n=17), the small children under 15 kg were highest (29.4%) in that group, and there was also no significant difference of defect size to BSA ratio among the 3 groups. Scientific studies have repeatedly confirmed that the GSO, through its specific device properties, is a reliable device for successfully treating ASD with various morphologies such as aortic rim deficiency, septal aneurysm and multiple defects.3)24)25)
This study has some limitations that must be pointed out, especially because of its retrospective nature. In addition, the selection of the device was based on the standard treatment guideline, rather than on randomization. Nevertheless, our study was conducted in a large cohort of patients by an experienced interventionist, who had the trained capacity to exclude procedural failure related with the learning curve. Although immediate procedural results and early to mid-term results were excellent in our cohort, longer follow-up is warranted because of increasing potential concerns.
In conclusion, the FSO and GSO were found to be reliable, safe and effective as well as ASO in transcatheter ASD closure according to our mid-term follow-up. These recent generation devices offer great practical clinical value, and we confirmed them to be therapeutic alternatives by verifying their efficacy and safety with various morphologies in selected patients with feasible anatomy.
 XML Download
XML Download