

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Radical hysterectomy or definitive chemoradiation (CRT) are treatment options used for International Federation of Gynecology and Obstetrics (FIGO) stages IA2–IIA cervical cancer. Given that over half of patients who undergo radical hysterectomy for stage IB–IIA will need adjuvant radiation, definitive CRT is the preferred treatment for FIGO IB2 and IIA2 bulky tumors [1].
The use of “adjuvant” or completion hysterectomy is another treatment strategy used outside of the United States [23]. Despite some studies showing potentially favorable outcomes for adjuvant hysterectomy after radiation or CRT, the magnitude of benefit from completion hysterectomy has not been established with larger series of patients [4567]. Previous studies exploring the benefit of adjuvant hysterectomy either did not use concurrent chemotherapy or were not powered to detect a difference in survival. The Gynecologic Oncology Group (GOG) 71-Radiation Therapy Oncology Group (RTOG) 84-22 trial randomized patients with IB2 tumors to external beam radiation therapy (EBRT) and brachytherapy (80 Gy to point A) vs. EBRT and brachytherapy (75 Gy to point A) followed by adjuvant hysterectomy [8]. This trial showed no difference in overall survival (OS) but a trend towards higher local recurrence in the arm without hysterectomy. The GYNECO 02 trial from France randomized 61 patients to CRT or CRT followed by hysterectomy [2]. This trial showed no therapeutic impact of adjuvant hysterectomy but was closed early due to lack of accrual.
Additionally, more recent minimally-invasive surgical techniques may make hysterectomy after preoperative treatment more feasible with less post-operative morbidity [9101112]. However, a recent meta-analysis investigating the use of adjuvant hysterectomy after concurrent CRT for locally-advanced cervical cancer found the pooled incidence of grade 3 and higher post-operative adverse events to be 26.5% [13]. The degree to which more modern surgical techniques have influenced the use of adjuvant hysterectomy for early-stage cervical cancer is not fully know thus we sought to identify patterns of care involving this treatment strategy.
Given the limited data regarding this clinical question in the modern era which includes the use of concurrent chemotherapy and more minimally invasive surgical techniques, we sought to identify treatment patterns and survival outcomes for cervical cancer based the use of adjuvant hysterectomy using a large, national cohort from the National Cancer Database (NCDB).
MATERIALS AND METHODS
The NCDB is a nationwide, hospital-based registry that consists of patients who received care at cancer centers accredited by the American College of Surgeons Commission on Cancer (CoC) and currently captures approximately 70% of all patients newly diagnosed with cancer [1415]. The CoC's NCDB and the accredited facilities participating in the NCDB are the source of the de-identified data used in this study. However, they have not verified and are not responsible for the statistical validity or conclusions derived by the authors of this study. This project did not meet the definition of human subjects research and therefore Intuitional Review Board approval was not required.
The NCDB was queried for patients with cervical cancer diagnosed from 2010–2014 who underwent preoperative concurrent chemoradiation followed by hysterectomy (CRT+S group) or concurrent chemoradiation alone (CRT group). Patients in the CRT+S arm were those that had CRT followed by hysterectomy in their first course of treatment as captured by the NCDB. Patients diagnosed prior to 2010 were excluded as FIGO staging was not recorded. FIGO stage IB2 through IIA2 were included. Concurrent chemotherapy was defined as starting within 2 weeks of the start of radiation. Patients receiving CRT+S had to receive at least a total dose of 60 Gy. Patients receiving CRT alone had to receive a total dose of at least 80 Gy. A lower dose cutoff was used for the CRT+S group than for the CRT group since those patients that undergo adjuvant hysterectomy typically are prescribed a lower dose of radiation as compared to those undergoing definitive CRT [28]. Both of these cutoffs are slightly lower than the typically doses prescribed in each of these clinical scenarios to account for potential lack of conversion of brachytherapy doses into 2-Gy equivalent based on commonly used fractionation schemes as cited by the American Brachytherapy Society (ABS) [16]. Those receiving nonstandard doses were excluded (Fig. 1). Additionally, to account for immortal time bias, patients living less than 6 months from the time of diagnosis were excluded.
Fig. 1
Cohort selection diagram.
CRT, chemoradiation; CRT+S, preoperative chemoradiation + hysterectomy; FIGO, International Federation of Gynecology and Obstetrics; NCDB, National Cancer Database.

The primary goal of this analysis was to study the patterns of care regarding preoperative CRT followed by hysterectomy. The secondary goal of this analysis was to analyze survival. Vital status was available but not cause of death. Demographic, clinical, and treatment details were obtained and compared via the Pearson's χ2 test between those patients treated with CRT+S and CRT alone. Patient demographic details included age, gender, and race. Clinical and treatment details included tumor stage, tumor size, Charlson-Deyo score, histology, pelvic and para-aortic lymph node status, number of chemotherapy agents, the categorization of academic or non-academic cancer center, U.S. region, insurance type, and year of diagnosis.
Univariable logistic regression was performed to assess for predictors of CRT+S. The variables included in were age, FIGO stage (stage IB2, stage IIA not otherwise specified [NOS], stage IIA1, and stage IIA2), tumor size (≤4 cm, 4–8 cm, and >8 cm), modified Charlson-Deyo comorbidity score (0, 1, and ≥2), race (White, Black, and Other), histology (squamous cell carcinoma, adenocarcinoma, adenosquamous, and NOS), pelvic and para-arotic lymph nodes (positive, negative, and not assessed), chemotherapy (single-agent, multiagent), facility type (academic, non-academic), U.S. regions (Northeast, Midwest, South, and West), insurance status (none, private insurance, Medicare, Medicaid, Other Government, and Unknown), and year of diagnosis (2010, 2011, 2012, 2013, and 2014). Variables with a p-value <0.10 on univariable analysis were planned to be included in the multivariable analysis.
OS curves comparing those who received CRT+S to those who received CRT alone were generated using the Kaplan-Meier method and compared via the log-rank test. Univariable and multivariable Cox regression was used to determine covariables associated with differences in OS. Factors associated with a p-value <0.10 on univariable analysis were included in the multivariable analysis. The variables included in these analyses were age, FIGO stage (stage IB2, stage IIA NOS, stage IIA1, and stage IIA2), tumor size (≤4 cm, 4–8 cm, and >8 cm), modified Charlson-Deyo comorbidity score (0, 1, and ≥2), race (White, Black, and Other), histology (squamous cell carcinoma, adenocarcinoma, adenosquamous, and NOS), pelvic and para-arotic lymph nodes (positive, negative, and not assessed), chemotherapy (single-agent, multiagent), facility type (academic, non-academic), U.S. regions (Northeast, Midwest, South, and West), insurance status (none, private insurance, Medicare, Medicaid, Other Government, and Unknown), and year of diagnosis (2010, 2011, 2012, 2013, and 2014). All analysis was performed using SPSS version 20 (IBM Corp., Armonk, NY, USA).
RESULTS
1. Patient characteristics and patterns of care
There were 1,546 patients who met the study criteria, of which 1,407 (91.0%) received concurrent CRT alone and 139 (9.0%) received CRT+S. The median follow-up time was 33.3 months. Table 1 provides a summary of the patient demographic and clinical characteristics. Patients over the age of 65 made up a larger percentage of the CRT group, 16.2% vs. 9.4% in the CRT+S group (p=0.034). Additionally, more patients had stage IIA2 disease in the CRT group as compared to the CRT+S group, 12.5% vs. 7.9%, respectively (p=0.056). Adenocarcinoma histology comprised 18.0% of the CRT+S group and 12.7% of the CRT group and adenosquamous histology made up 5.8% of the CRT+S group and 3.1% of the CRT group (p<0.001). Positive pelvic nodes were present in 16.7% of patients treated with CRT compared to 7.9% in patients who were treated with CRT+S (p=0.024). More patients in the CRT+S arm had private insurance as compared to the CRT, 51.1% vs. 43.2%, respectively (p=0.014).
Table 1
Demographic and clinical characteristics of patients

Values are presented as number (%).
CRT, chemoradiation; CRT+S, preoperative chemoradiation+hysterectomy; FIGO, International Federation of Gynecology and Obstetrics; NOS, not otherwise specified.
Demographic, clinical, and treatment details were obtained and compared via the Pearson's χ2 test between those patients treated with CRT+S and CRT alone.
2. Predictors of completion hysterectomy
On multivariable analysis, adenocarcinoma (odds ratio [OR]=2.26; 95% confidence interval [CI]=1.29–3.95; p=0.004) and adenosquamous cell carcinoma histologies (OR=3.72; 95% CI=1.52–9.10; p=0.004) were associated with increased likelihood of undergoing CRT+S compared to squamous cell carcinoma. Stage IIA2 disease was associated with decreased likelihood of being treated with CRT+S (OR=0.43; 95% CI=0.43–0.19; p=0.046). Patients living in the Midwest (OR=2.47; 95% CI=1.18–5.17; p=0.02), the South (OR=2.72; 95% CI=1.34–5.55; p=0.006), and the West (OR=2.85; 95% CI=1.27–6.41) were more likely than patients living in the Northeast to receive CRT+S. Facility type (non-academic or academic) and insurance type were not predictive for treatment group. The results of the analysis of patterns of care for CRT+S receipt are summarized in Table 2.
Table 2
Univariable and multivariable logistic regression for the receipt of CRT+S over CRT

CI, confidence interval; CRT, chemoradiation; CRT+S, preoperative chemoradiation + hysterectomy; FIGO, International Federation of Gynecology and Obstetrics; NOS, not otherwise specified; OR, odds ratio.
*Univariable logistic regression was performed to assess for predictors of CRT+S. Variables with a p-value <0.10 on univariable analysis were included in the multivariable analysis.
3. OS
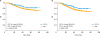
Kaplan-Meier curves depicting survival in patients grouped by receipt of CRT+S vs. CRT are shown in Fig. 2A. Four-year OS for the CRT+S group was 82.2% and 74.9% for the CRT group (p=0.036). On subgroup analysis by lymph node status, the 4-year OS for patients without positive pelvic or para-aortic lymph nodes was 84.9% in the CRT+S group vs. 77.8% in the CRT group (p=0.072) (Fig. 2B). On subgroup analysis by histologic subtype, there were no differences in OS between the CRT+S group vs. the CRT group. Likewise, there were no differences in OS on subgroup analysis by stage between the CRT+S group vs. the CRT group.
Fig. 2
(A) Kaplan-Meier OS curve for entire cohort. (B) Kaplan-Meier OS curve for patients without positive lymph nodes. (A) are shown below the data: CRT+S, 4-year OS 82.2%; CRT, 4-year OS 74.9%; p-value=0.036. (B) are shown below the data: CRT+S, 4-year OS 84.9%; CRT, 4-year OS 77.8%; p-value=0.072.
CRT, chemoradiation; CRT+S, preoperative chemoradiation + hysterectomy; OS, overall survival.
On multivariable Cox regression, Charlson-Deyo comorbidity score of 1 (hazard ratio [HR]=1.56; 95% CI=1.10–2.21; p=0.012) and 2 (HR=2.97; 95% CI=1.83–4.84; p<0.001) were associated with decreased OS. Positive pelvic lymph nodes (HR=2.03; 95% CI=1.46–2.84; p<0.001) and positive para-aortic lymph nodes (HR=2.78; 95% CI=1.76–4.38; p<0.001) were also associated with decreased OS. There was no difference in survival based on treatment group (HR=0.64; 95% CI=0.40–1.04; p=0.069). A summary of the findings of the univariable and multivariable Cox regression for OS are found in Table 3.
Table 3
Univariable and multivariable Cox regression for OS

CI, confidence interval; CRT, chemoradiation; CRT+S, preoperative chemoradiation + hysterectomy; FIGO, International Federation of Gynecology and Obstetrics; HR, hazard ratio; NOS, not otherwise specified; OS, overall survival.
*Univariable and multivariable Cox regression was used to determine covariables associated with differences in OS. Factors associated with a p-value <0.10 on univariable analysis were included in the multivariable analysis.
DISCUSSION
We found in this large hospital-based analysis that completion hysterectomy was utilized after CRT 9.0% of the time. While there was a survival benefit for the whole cohort, with a 4-year OS for CRT+S, 82.2% compared to 74.9% for CRT (p=0.036), this was no longer significant on multivariable analysis.
The addition of adjuvant hysterectomy following radiation was used more frequently in previous years in the United States but later fell out of favor as the exact benefit compared to radiation alone was not clearly defined [817181920]. However, the use of completion hysterectomy is sometimes used as a treatment strategy abroad [2]. A recent French national survey found completion hysterectomy was still being performed in one of third of academic centers after complete response to preoperative treatment and negative para-aortic nodes [3]. Data regarding pathologic response after preoperative treatment suggests completion hysterectomy may provide a benefit in the setting of residual disease [2122]. For example, in a series with 143 patients with stages IB2–IVA disease, completion hysterectomy for residual disease >2 cm after CRT resulted in survival rates at 3 and 5 years of 80% [23]. However, despite the theorized benefits a convincing argument for the advantage of completion hysterectomy in the form of a large, randomized trial has yet to be made.
The GOG 71-RTOG 84-22 randomized patients with IB2 tumors to EBRT and brachytherapy vs. EBRT and brachytherapy followed by hysterectomy and showed no difference in OS but a trend towards increase in progression-free survival (PFS) (62% vs. 53% at 5 years, p=0.09) [8]. This trial did not use concurrent chemotherapy. The GYNECO 02 trial randomized 61 patients with IB2–IIB disease to definitive CRT or CRT followed by hysterectomy and also failed to show a therapeutic impact of hysterectomy. However, this trial was closed early due to lack of accrual. Three-year disease-free survival rates were 72% and 89% in the CRT+S and CRT arms, respectively (p=0.15). The 3-year OS rates were 86% and 97%, respectively (p=0.17). The authors postulate the lack of accrual was partly due to reluctance on the part of treating physicians to enroll patients on a trial in which they may not have a completion hysterectomy [2]. A more recent randomized study by Cetina et al. [9] failed to show a benefit of hysterectomy after EBRT only in patients with IB2–IIB cervical cancer as compared to definitive CRT and brachytherapy. PFS rates were 74.8% and 71.7% in the CRT and CRT+S arms respectively (p=0.186). OS rates were 76.3% in the CRT arm vs. 74.5% in the CRT+S arm (p=0.236). While none of the previously described studies showed an OS benefit with the addition of completion hysterectomy, each had its own respective shortcoming thus not sufficiently answering the question.
Whereas previously the use of multimodality treatment resulted in increased morbidity as compared to CRT alone, more recent data show that complications after hysterectomy following EBRT are comparable to hysterectomy as the primary treatment [19]. Additionally, the use of minimally invasive laparoscopic hysterectomy may result in less post-operative morbidity [101112]. As such, hysterectomy could possibly be more easily be incorporated into the treatment strategy in the present era if a benefit could be established.
In the present analysis, 4-year OS for the CRT+S group was 82.2% and 74.9% for the CRT group (p=0.036). While our study showed increased survival in patients receiving CRT+S, this benefit lost significance on multivariable analysis. As such, the survival benefit observed may be in part due to differences between the patients selected for CRT+S vs. CRT. For example, more patients in the CRT arm had positive pelvic lymph nodes as compared to the CRT+S group. On subgroup analysis by lymph node status, the 4-year OS for patients without positive pelvic or para-aortic lymph nodes was 84.9% in the CRT+S group vs. 77.8% in the CRT group (p=0.072). The fact that this finding was not statistically significant may be in part because this portion of the analysis was underpowered to detect a statistical difference given the small number of patients in this subgroup. Although this finding was not statistically significant, it is plausible that a difference could be detected in a larger group of patients and even that a clinically significant difference in local control resulted from the use of adjuvant hysterectomy. However, this information cannot currently be ascertained from the NCDB. Furthermore, there may be cofounding factors even among the patients with node-negative disease similar to the entire cohort of patients that may have resulted in selection bias. For example, patients with less advanced tumor staging and less medical comorbidities may have been more likely to be selected for adjuvant hysterectomy and the difference in survival among those groups could be partially due to differences in patient factors.
In the present study, patients with IIA2 disease were less likely to undergo completion hysterectomy as compared to earlier stages. Additionally, we found that patients with adenocarcinoma and adenosquamous histologies were also more likely to be treated with CRT+S. Previous randomized studies investigating the role of CRT+S did not analyze the interplay of histology and treatment modality however older data suggest CRT+S may be beneficial for adenocarcinoma as compared to CRT alone [24]. However, in the current study we did not find a survival difference on subgroup analysis based on histologic subtype. Additionally, patients in this series from the Midwest, South, and West were more likely to be treated with CRT+S as compared to the Northeast, where there is a higher density of academic centers. Patients diagnosed in 2014 were less likely to be treated with CRT+S as compared to 2010.
In summary, although there is a theoretical benefit to the use of completion hysterectomy after CRT, this has not been demonstrated with a large, randomized trial. The GOG 71-RTOG 84-22 study did not use concurrent chemotherapy and GYNECO 02 and the study by Cetina et al. [9] were not powered to detect a survival difference. In our analysis, CRT+S was used in only 9.0% of the patients with stage IB2–IIA cervical cancer from 2010–2014 and did not result in a survival benefit when accounting for other factors. Patients in the current analysis were more likely to receive CRT if they had node-positive disease and more advanced staged disease suggesting the difference in survival may have been related to differences in treatment groups. Even though a difference in survival was found between CRT and CRT+S in the patients with node-negative disease, this was not statistically significant and again may have been due to other differences between the treatment groups. Additionally, patients with residual disease after preoperative CRT may derive more benefit from completion hysterectomy as compared to those without however the amount of residual disease could not be completely assessed in the current analysis with the data available from the NCDB.
Our findings were similar to the studies exploring the use of adjuvant hysterectomy previously described in which a benefit of adjuvant hysterectomy could not be clearly established. This may have been in part due to lack of accrual in those prospective studies and in the case of our study, the fact that this strategy is infrequently used even among a national cohort. A large-randomized trial in which arms are more balanced in terms of stage, nodal status, and comorbidities could shed light on this clinical question however this is not likely to be undertaken due to issues with accrual in previous studies, concern for post-operative complications as seen in the adjuvant hysterectomy arm, and little concrete evidence supporting the use of this strategy. Therefore, despite the theoretical benefit of an adjuvant hysterectomy, there is not currently enough evidence to recommend the routine use of this strategy for stages IA2–IIA cervical cancer including those with node-negative disease.
There are challenges and limitations with hospital-based registries. While data reporting to the NCDB is highly standardized, there may still be variances with data abstraction resulting in inaccurate coding. Other limitations include lack of information regarding recurrence and salvage therapy, as well as the lack of information regarding the cause of death. Given that only data regarding the patient's first course of treatment is captured in the NCDB, it is plausible that surgery could have been performed as salvage therapy later in time in some patients in the CRT group which would confound the results. Additionally, information regarding the time interval between CRT and hysterectomy was not consistently available for all patients in the CRT+S group. Due to selection bias, patients treated with CRT+S may have had a better performance status than those selected for CRT and as well as less high-risk clinical features including node-positive disease. Accordingly, the group of patients treated in CRT+S arm may have been more likely to have better survival regardless of the use of hysterectomy. Additionally, a large percentage of patients in each group did not have pelvic and para-aortic lymph nodes assessed either by imaging or biopsy. Therefore, there could be even greater differences among clinical features between the treatment groups than can be accounted for with the variables that were used. Furthermore, the amount of residual disease after preoperative treatment and pathologic response could not be completely assessed using data from the NCDB. Finally, we were unable to assess specific postoperative complications that may occur after concurrent CRT such as the development of fistulas or infections in the CRT+S group of patients.
In conclusion, we found from this large hospital database that completion hysterectomy is used infrequently and did not result in a significant survival difference when accounting for other factors. We conclude that although a theoretical benefit for the use of adjuvant hysterectomy may exist, there is not substantial clinical evidence to support the use of this strategy for stages IA2–IIA cervical cancer including those with node-negative disease.
 XML Download
XML Download