

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Among females, cancer is the second leading cause of death worldwide [1]. Malignant diseases of the breast and genitals are the most common cancers in women with estimated 1.67 million and 1.09 million new cases diagnosed worldwide in 2012 [2]. Currently, breast cancer ranks first (25.5% of all incident cancers), and other gynecological cancers (corpus uteri, cervix uteri and ovary) rank second (16.5% of all incident cancers) [2]. Therefore, preventing the occurrence of gynecological cancers is essential. A combination of multiple environmental and genetic factors has been considered to contribute to the occurrence of gynecological cancers, and particular interest has focused on dietary intake.
Diet is a major source of bioactive components that may potentially contribute to the interaction with chronic inflammation [34], which might trigger the promotion of cellular proliferation, mutagenesis, inhibition of apoptosis, and secretion of mediators that may promote malignant transformation of cells and carcinogenesis [56]. A literature-derived, population-based dietary inflammatory index (DII) was recently developed to assess the inflammatory potential of an individual's diet [7]. The DII reflects a robust literature base, large number of articles that explored the effect of dietary parameters on the 6 inflammatory markers (interleukin [IL]-1β, IL-4, IL-6, IL-10, tumor necrosis factor [TNF]-α and C-reactive protein [CRP]) were screened for inclusion in the DII scoring algorithm [7]. Food frequency questionnaire (FFQ)-derived DII has also been significantly predicted higher blood concentrations of inflammatory markers such as CRP, IL-6, or TNFα-R2 among US postmenopausal women [8], Iranian women [9], German [10], Australians [11], Chinese [12], Italians [13], Swiss [14], and French [15]. Hence, based on global nutritional surveillance data sets, the DII can be applied to quantitative comparisons of dietary inflammatory status and health outcomes in diverse populations [7].
Recently, many studies have assessed the relationship between the DII and gynecologic cancers [16171819]. However, the results remain inconsistent and controversial. Elevated DII has been shown to be associated with high gynecologic cancer risk in some [1617], but not all [1819] studies. These conflicting findings might be due to different study design, sample size of study, and menopausal status of included participants. Therefore, we conducted this meta-analysis to systematically assess the association between DII and the risk of gynecologic cancers.
MATERIALS AND METHODS
1. Data sources and search strategies
We conducted this meta-analysis under the guidance of PRISMA. Two authors (LZY and GXP) independently searched the electronic databases, including PubMed, EMBASE and Web of Science, from inception to October 20, 2018. Search terms included: ((breast OR ovary OR ovarian OR endometrial OR endometrium OR “gynecological neoplasms, female”[mesh]) AND (cancer* OR carcinoma* OR neoplasm* OR malignan* OR tumour* OR tumor*)) AND (dietary inflammatory index OR inflammatory potential of diet OR inflammatory diet OR anti-inflammatory diet OR dietary score OR pro-inflammatory diet OR inflammatory potential intake). What's more, we also had a manual search of the references lists of the retrieved studies in case any additional study was missed. Related articles generated by PubMed and Google Scholar (https://scholar.google.com/) were also searched.
2. Study selection
Studies met all of the following inclusion criteria were considered: 1) the study design was a case-control or cohort study; 2) the DII was assessed, and the risk estimates were reported according to at least three DII category; 3) the outcome should include at least one of the following gynecological cancers: breast cancer, ovarian cancer, cervical cancer, or endometrial cancer; 4) the study reported outcome measures with adjusted odds ratios (ORs), relative risks (RRs), or hazard ratios (HRs) and 95% confidence intervals (CIs), or gave enough information to estimate these measurements. The exclusion criteria were listed as follows: 1) repeated survey population; 2) experimental laboratory studies, nonhuman animal research, letters, or review articles; and 3) studies that observed less than 30 participants. If data were duplicated or shared in more than one study, the study with the largest dataset was included.
3. Data extraction
Two authors (LZY and GXP) independently extracted data, and disagreements between investigators were resolved by discussion. The following variables were extracted from each study: study characteristics (the name of the first author, year of publication, journal name, country in which the study was conducted, study design, study period, duration of follow-up for cohort study, source of control for case-control study, type of cancer studied), participant characteristics (sample size and mean age of cases and controls or population at risk), DII characteristics (dietary assessment methods and number of food parameters to calculate DII), maximally adjusted ORs, RRs or HRs with 95% CIs and adjusted confounders, and the results of subgroup analysis, if any.
The methodological quality of potential studies was assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS) [20]. This measurement judges a study quality based on the selection, comparability, exposure (for case-control studies), or outcome (for cohort studies). The score ranges from 0 to 9 points, with a higher score ≥7 indicating higher study quality.
4. Statistical analysis
We investigated the associations between the DII (highest versus lowest categories) and the risk of gynecological cancers as the main analyses. Because the incidence of gynecological cancers was relatively low, ORs were considered as good approximations of RR and combined with RRs, resulting in a common estimate of RR [21]. The pooled RR with 95% CIs was calculated using the random-effect models based on the DerSimonian and Laird method [22]. The random-effects model was chosen a priori because of the anticipated clinical heterogeneity and because it was considered as more conservative than the fixed-effects model, as it accounted for both within- and between-study heterogeneity [23]. We examined the heterogeneity of the results across studies using the I2 statistic (higher values denoting greater heterogeneity) [24]. An I2 value >50% was considered to indicate significant heterogeneity [25].
We further analyzed the trend between DII and the risk of gynecological cancers using parametric method, therefore a dose-response meta-analysis was performed by using the method proposed by Greenland and Longnecker [26]. The method required the numbers of gynecological cancers' cases and population at risk (or controls) for at least three categories of DII and the mean or median values for each category provided. For those studies that did not provide the median or mean DII for each category, we assigned the midpoint of the upper and lower boundaries in each category as the average level. If the highest or the lowest category was open-ended, we assumed the width of the interval to be the same as that of the closest category.
To explore the source of heterogeneity among studies, we conducted subgroup analyses based on study design (case-control or cohort study), cancer type (breast, ovarian, or endometrial cancer), age (<55 or ≥55 years), body mass index (BMI) (<25 or ≥25 kg/m2), family history of hormone-related cancers (yes or no), menopausal status (pre- or post-menopause), and parity (0 or ≥1), respectively. We also conducted influence analysis to assess the effect of each individual study on the summary risk estimates. Moreover, meta-regression was performed by using study design, publication year, cancer type, age, family history of cancer, menopausal status, and parity as covariates.
Publication bias was evaluated using Egger's and Begg's tests with visual inspection of funnel plots [2728]. The number of missing studies and the effect that these studies might have had on the outcome was explored by using nonparametric rank-based data augmentation techniques (trim-and-fill procedure) developed by Duval and Tweedie [29]. The p value <0.05 was considered statistically significant in all analyses, except for the Egger test (p<0.10) because of the low power of the test. All analyses were conduct with Stata software package version 11.0 (StataCorp, College Station, TX, USA).
RESULTS
1. Study search and characteristics
A total of 548 articles were identified by searching electronic databases from inception to October (Fig. 1). There were 405 articles left after duplicates removed. Through title and abstract scanning, 309 articles were considered unrelated and excluded. We reviewed the full texts of the remaining articles and 68 articles were excluded because of the following reasons: same cohort of patients (n=5) and no sufficient data (n=63). Three additional eligible articles were included after updated searching. Finally, 18 eligible studies were included in this meta-analysis.

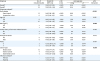
The main characteristics of included studies are shown in Table 1. These 18 studies included 12 case-control studies (10,774 cases and 15,958 controls) and 6 prospective cohort studies (330,363 participants and 23,133 incident cases). Studies were published between 2015 and 2018. Diet intake was estimated by through validated FFQs with items ranged from 78 to 260 and 24-h dietary recall, and all of the studies followed the method developed by Shivappa et al. [7] to calculate the DII (using 25-36 dietary components). Among these studies, 7 of them were carried out in Europe, 6 in the United State, 2 in Iran, 1 in Argentina, Australia, and China. Mover, adjustments for potential confounders in each study were listed in the Supplementary Table 1. The NOS scores of most included studies (17/18) were over 7 (Supplementary Tables 2 and 3).
Table 1
Main characteristics of the eligible studies

| Author (year) | Countries | Sample size* (n1/n2) | Follow-up duration (yr) | Source of controls | Age† (yr) | Dietary assessment | No. of food parameters to calculate DII | Cancer type | NOS score | |
|---|---|---|---|---|---|---|---|---|---|---|
| Case-control study | ||||||||||
| Ge et al. (2015) [49] | Germany | 2,887/5,512 | - | Population | 62 | FFQ (176-item) | 25 | Breast cancer | 8 | |
| Shivappa et al. (2016) [17] | Italy | 454/908 | - | Hospital | 60.67 | FFQ (78-item) | 31 | Endometrial cancer | 8 | |
| Shivappa et al. (2016) [18] | Italy | 1,031/ 2,411 | - | Hospital | 56.7 | FFQ (78-item) | 31 | Ovarian cancer | 8 | |
| Huang et al. (2017) [47] | China | 867/824 | - | Hospital | 47.5 | FFQ (81-item) | 33 | Breast cancer | 7 | |
| Niclis et al. (2017) [36] | Argentina | 317/526 | - | NA | NA | FFQ | NA | Breast cancer | 6 | |
| Peres et al. (2017) [19] | USA | 493/662 | - | Population | 49.5 | FFQ (110-item) | 27 | Epithelial Ovarian cancer | 7 | |
| Ricceri et al. (2017) [37] | Italy | 297/307 | - | Hospital and population | 60.94 | FFQ (260-item) | 27 | Endometrial cancer | 9 | |
| Shivappa et al. (2017) [50] | Italy | 2,569/2,588 | - | Population | 55 | FFQ (78-item) | 31 | Breast cancer | 8 | |
| Jalali et al. (2018) [38] | Iran | 134/267 | - | Hospital | 47.90 | FFQ (168-item) | 34 | Breast cancer | 8 | |
| Nagle et al. (2018) [51] | Australian | 1,375/1,415 | - | Population | 56.99 | FFQ (139-item) | 31 | Ovarian cancer | 8 | |
| Shivappa et al. (2018) [16] | USA | 205/390 | - | Hospital and population | NA | FFQ (110-item) | 29 | Ovarian cancer | 8 | |
| Vahid et al. (2018) [34] | Iran | 145/148 | - | Hospital | 49.17 | FFQ (168-item) | 31 | Breast cancer | 8 | |
| Prospective cohort study | ||||||||||
| Shivappa et al. (2015) [52] | Sweden | 49,258/6,944 | 20 | NA | 40.3 | FFQ (80-item) | 29 | Breast cancer | 9 | |
| Graffouillere et al. (2016) [53] | France | 3,771/158 | 12.6 | NA | 49.2 | 24-h dietary record | 36 | Breast cancer | 9 | |
| Tabung et al. (2016) [48] | USA | 122,788/7,495 | 16.02 | NA | 64.5 | FFQ (122-item) | 32 | Breast cancer | 8 | |
| Tabung et al. (2016) [54] | USA | 70,998/3,471 | 16.05 | NA | 64.5 | FFQ (122-item) | 32 | Breast cancer | 9 | |
| Park et al. (2017) [35] | USA | 49,731/2,155 | 7.6 | NA | 54.5 | FFQ (146-item) | NA | Breast cancer | 7 | |
| Shivappa et al. (2017) [55] | USA | 33,817/2,910 | 25 | NA | 62 | FFQ (121-item) | 29 | Breast cancer | 9 | |
DII, dietary inflammatory index; FFQ, food frequency questionnaire; NA, not available; NOS, Newcastle-Ottawa Quality Assessment Scale.
*n1 was number of cases and n2 was number of controls for case-control study; n1 was number of participants/ and n2 was number of cases incident during follow-up for cohort study; †mean or median years of age.
2. DII and risk of gynecological cancers
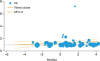
As shown in Table 2 and Fig. 2, in the meta-analysis of all 18 studies, using the random-effects model and ORs calculated by supplements included DII, women in the highest category had an increased risk of gynecological cancers than those in the referent category (pooled RR [95% CIs], 1.38 [1.21–1.56]; p<0.001), with a significantly between-study heterogeneity (I2=85.8%), and there was no significant difference when choosing another group of outcome in study by Peres et al. [19]. that calculated the DII without supplement (pooled RR [95% CIs], 1.36 [1.20–1.54]; p<0.001; I2=85.4%) (Supplementary Fig. 1).
Table 2
Overall and stratified analyses on the association between DII and the risk of gynecological carcinoma
BMI, body mass index; CI, confidence interval; DII, dietary inflammation index; RR, relative risk.
*Each foot-note is presented as for p value of Q-test for between study heterogeneity test; †for DII calculated with consideration of dietary supplements; RRs and 95% CIs were pooled by using the random effects model (the DerSimonian and Laird method); ‡for DII calculated without consideration of dietary supplements; RRs and 95% CIs were pooled by using the random effects model (the DerSimonian and Laird method); §for RRs and 95% CIs were pooled by using the fixed effects model; ‖Influence analysis was conducted by eliminating one study at a time; for overall, the excluded study was the study by Huang et al. [47] for minimal pooled RRs, and the study by Tabung et al. [48] for the maximal pooled RRs.
Fig. 2
Forest plots of associations between DII and the risk of gynecological cancers. Error bars indicate 95% confidence intervals.
DII, dietary inflammatory index.

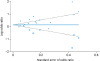
Dose-response analyses were explored with linear, three knots, four knots, and five knots, and goodness-of-fit χ2 were 142.02, 140.59, 133.95, and 133.34, respectively. Thus, the linear model was chosen (plinearity=0.002) (Fig. 3) and the pooled dose-response RR was 1.07 (95% CIs, 1.03–1.12; p=0.002) when the DII score increased by 5 units.
Fig. 3
Dose–response relationship between DII and the risk of gynecological cancers. The dots represent the relative risks corresponding to DII in each individual study. The area of the dots is inversely proportional to the logarithm of the variance of the relative risk.
CI, confidence interval; DII, dietary inflammatory index; RR, relative risk.
3. Subgroup analysis and meta-regression
We conducted subgroup analysis to explore the potential source of heterogeneity among the included studies (Table 2). Stratified by study design indicated that, the pooled RRs was significantly higher for case-control studies than cohort studies (RR: 1.48 vs. 1.07; p for interaction<0.001), for studies conducted among participants with BMI ≥25 kg/m2 than participants with BMI <25 kg/m2 (RR: 1.52 vs. 1.23; p for interaction=0.026), among participants with ovarian cancer and endometrial cancer than participants with breast cancer (RR: 1.42; 1.49 vs. 1.19; p for interaction=0.038). Stratified analyses suggested that the association did not differ among age strata, family history of hormone-related cancers, menopausal status, and parity (p interaction range: 0.126–0.975) (Supplementary Figs. 2, 3, 4, 5, 6, 7, 8). Meta-regression analysis further confirmed that study design significantly contributed to inter-study heterogeneity (p≤0.001) (Supplementary Table 4).
4. Sensitivity analysis and publication bias
The sensitivity analysis indicated that the pooled RRs were not obviously influenced by any single study (Table 2).
Both Egger's and Begg's test revealed significant publication bias, and the p values were 0.019 and 0.037. The funnel plot also indicated evidence of publication bias. After imputing six missing studies by using the trim-and-fill method, the recalculated pooled RRs were attenuated, but not substantially changed from the initial estimates (imputed RR [95% CIs], 1.179 [1.030–1.350]; p=0.017) (Fig. 4).
DISCUSSION
The present meta-analysis had systematically reviewed published epidemiological studies on the association between DII and the risk of gynecological cancers. The pooled results find that women in the highest DII category had an increased risk of gynecological cancers, compared with those in the lowest DII category. The association was further confirmed in the sensitivity and dose-response analyses. Although a significant publication bias was observed, the association persisted after correction using the trim-and-fill method. Subgroup analyses indicated that the adverse effects of elevated DII turned out to be more prominent among case–control studies (vs. cohort study), participants with ovarian cancer and endometrial cancer (vs. breast cancer), and obese (vs. non-obese) participants.
With 33,907 gynecological cancers cases, our results reinforced and complemented the findings in several previous studies [30313233], which indicated that the elevated DII certainly linked with higher risk of gynecological cancers. Compared with those previous meta analyses, our studies included 6 new eligible studies [163435363738], and more studies enable us to explore the potential source of heterogeneity such as stratified analyses according to study design, and different age and BMI strata.
An inflammatory index (DII) has recently been developed and refined to quantify the inflammatory potential of individual diets [7], and has been widely used in cancer screening among populations or in public health interventions. The DII was created based on the literature to assess each food having a positive or negative effect on inflammation, and the index score was calculated using the dietary intake data from the FFQ as described in Shivappa et al. [7]. Moreover, DII has been validated in a variety of longitudinal and cross-sectional studies with various systemic inflammatory markers that have been shown participate in both the initiation and progression of cancer, including CRP [39], IL-6 [839], and TNF-α [8]. Chronic inflammation makes adverse effects on body health, and some studies [640] suggested that systemic inflammation plays a vital role in cancer progression at nearly every process. Therefore, the diet-related inflammation may promote the occurrence of gynecological cancer through increasing estrogen production to disrupt the estrogen-progesterone balance [41], aggravating inflammatory reaction during ovulatory events, and promoting monocytes differentiate into tamoxifen that express numerous tumor-promoting characteristics [42].
Stratified by study design indicated that the estimates for case-control studies were significantly higher than for cohort study (p for interaction<0.001; pooled RR: 1.48 vs. 1.07). Among the 18 included studies, 12 were case-control studies and 6 were cohort studies. In case-control study, cases have the disease or outcome of interest, they may be more probing or thoughtful when examining past exposures or activities compared to controls, thus lead to recall bias [43]. Therefore, the recall bias associated with the case-control study design may have led to overestimated results. However, in our study, pooled RR of cohort studies still suggested a statistically significant estimate of a positive association, which indicated that, the recall bias contributed partly, but not all of the increased risk for the association between DII and risk of gynecological cancers.
Subgroup analysis for BMI revealed that the association between elevated DII and higher gynecological cancers risk varies among participants with different BMI strata (BMI: <25 vs. ≥25; p for interaction=0.026). High BMI or obesity has been shown to be associated with increased gynecological cancers risk [25]. The reason might be due to that the higher serum inflammatory mediators coursed by obesity [44], which can lead to chronic inflammation and trigger cellular events that can promote malignant transformation of cells and carcinogenesis.
In addition, we also found that elevated DII turned out to be more prominent among participants with ovarian cancer and endometrial cancer (vs. breast cancer). Compared with breast tissue, significant inflammatory components are involved in most of the key physiological processes of human reproductive tract, including follicle development, ovulation, implantation, pregnancy, labor, postpartum, remodeling and menstruation [45]. Therefore, as an influence factor of systemic inflammatory markers [839], dietary intake could more likely having effect on those physiological processes. Moreover, increased inflammatory components during physiological processes in the reproductive tracts [45] and dietary related chronic inflammation [46] could also contribute to the increased risk of ovarian cancer and endometrial cancer.
The present meta-analysis includes a large number of patients from both case-control and cohort studies allowing a relatively precise estimation of the strength of the association between DII and risk of gynecological cancers.
Nevertheless, there were also several limitations in this study. Firstly, the heterogeneity in the relation across studies was large. However, through subgroup and meta-regression analyses, we found that the heterogeneity could be mainly explained by study design, BMI status, and cancer type. Secondly, different covariates/confounders were adjusted for across the selected studies, which may contribute to the heterogeneity between studies. Thirdly, publication bias was observed in Begg's or Egger's tests, but using the trim-and-fill method to include supposedly missing negative studies, a significant positive association still persisted. Moreover, one study in this meta-analysis did not adjust for energy [36]; however, the result persisted after eliminating this study from overall analysis (RR, 1.33; 95% CI, 1.17–1.51). Finally, most study participants in this analysis were from Europe or the United States, thence, extrapolating these findings to multiple populations should be taken with caution.
Our meta-analysis indicated that, elevated DII independently was associated with a higher risk of gynecological cancers, especially in patients with ovarian cancer and endometrial cancer and among obese participants. More high-quality studies should be conducted to establish the evidence of the associations between the DII and risk of gynecological cancers among Asian populations.
 XML Download
XML Download