

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Mycoplasma hominis (MH) and Ureaplasma urealyticum (UU) are facultative anaerobic pathogens that usually colonize the lower genitourinary tract [12]. Although most colonized women remain asymptomatic, vaginal colonization with MH, UU, or both are associated with an increased risk of developing certain pathogenic conditions and pregnancy complications, such as pelvic inflammatory disease, postpartum infection, infertility, premature rupture of membranes (PROM), preterm labor, preterm birth, and systemic neonatal infections [345]. Doxycycline and quinolones are drugs of choice [678]. However, obstetricians empirically use macrolides for treatment of pregnant women in many cases due to fear of fetal abnormalities [910]. Antimicrobial susceptibility of MH, UU, and both has changed with times. It varies with geographic region too [1112131415]. Therefore, it is essential to know the latest antibiotic sensitivity in a particular region to ensure successful treatment. Such study regarding antimicrobial susceptibilities of MH, UU, and both in pregnant and non-pregnant women has not been reported in Korea yet. Therefore, the objective of this study was to investigate culture rates and the antimicrobial susceptibilities of MH, UU, and both MH and UU in pregnant and non-pregnant women residing in Cheonan city, a western area in South Korea.
Materials and methods
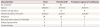
Non-pregnant women had undergone MH and UU culture and antimicrobial susceptibility test for abnormal vaginal discharge at our center from January 2017 to April 2018 were enrolled. In the non-pregnant group, tests were performed only for abnormal vaginal discharge, regardless of age, fertility, body mass index, underlying disease, or gynecologic disease. Abnormal vaginal discharge was considered present when the patient described having abnormal and bothersome discharge with respect to color, appearance, and odor as well as itching and burning sensations, necessitating examination and treatment (Table 1). In our study, we analyzed both UU and Ureaplasma parvum (UP) for ureaplasma infection. In the case of pregnant women, culture and antibiotic sensitivity tests were conducted only in the presence of a positive polymerase chain reaction test after admission for preterm labor or PROM. The patients-age ranged from 21 to 34 years, and culture was performed in women at more than 32 weeks of pregnancy. There were 30 cases of hospitalization because of preterm labor and 4 cases of hospitalization because of PROM. Women with multiple pregnancies were excluded from the study (Table 2).
Table 1
Clinical profiles of non-pregnant women (n=166)
![]()
Table 2
Clinical profiles of pregnant women (n=34)
![]()
Vaginal swabs were obtained from 200 women with a mean age of 37.7 years (range, 10–87 years) who were tested for the presence of MH and UU at Soonchunhyang University Cheonan Hospital between January 1, 2017, and April 30, 2018. Identification and antimicrobial susceptibilities of MU and UU were determined with a commercially available MYCOFAST Mycoplasma IST2 kit (bioMerieux, Macrcy-l'Etoile, France), as indicated by the manufacturer. Most hospitals in recent years use the same method despite using kits from different manufacturers. Briefly, the cotton swab included in the kit was inoculated in R1 transport medium, which could inhibit most gram-negative and gram-positive bacteria. The inoculated R1 medium was vortexed rapidly and 3 mL was added to R2 growth medium containing 1 mL lyophilized urea/arginine broth. After reconstitution and shaking, 55 μL was dispensed into each of 22 test wells on the strip. Two drops of mineral oil were added to each well. The remainder of the R2 medium and the inoculated strip were then incubated at 37°C and observed for color changes at 24 and 48 hours. Antimicrobial susceptibility testing included doxycycline, josamycin, ofloxacin, erythromycin, tetracycline, ciprofloxacin, azithromycin, clarithromycin, and pristinamycin.
The development or absence of red color at relevant part of the strip provided an index of resistance or susceptibility to each antimicrobial agent according to guidelines of the Clinical & Laboratory Standards Institute. The breakpoints for the antimicrobials tested are as follows: tetracycline susceptible S≤4, resistant R ≥8; doxycycline S≤4, R≥8; azithromycin S≤0.12, R≥4; clarithromycin S≤1, R≥4; erythromycin S≤1, R≥4; josamycin S≤ 2, R≥ 8; ciprofloxacin S≤1, R≥ 2; ofloxacin S≤1, R≥4; pristinamycin S≤1, R≥2. Per study protocol, these patients had not received any previous treatment with antibiotics for at least 6 weeks. Statistical analyses were performed using SPSS Statistics ver. 21 (SPSS, Chicago, IL, USA). Correlation was analyzed using χ2 test and Fisher's exact test. P-values <0.05 were considered statistically significant.
Results
The condition was assessed in 200 patients, including 34 (17%) pregnant women and 166 (83%) non-pregnant women. Of a total of 200 patients, positive culture results are as follows: MH only, n=10 (5%); UU only, n=58 (29%); and both MH and UU, n=36 (18%). The susceptibilities of MH only to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 100%, 10%, 40%, and 0%, respectively. The susceptibilities of UU only to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 94.8%, 87.9%, 5.2%, and 81%, respectively. The susceptibilities of both MH and UU to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 97.2%, 5.6%, 11.1%, and 11.1%, respectively (Table 3).
Table 3
Antimicrobial susceptibilities (%) of Mycoplasma hominis and Ureaplasma urealyticum for all patients (n=200)

Values are presented as number (%). The breakpoints (mg/L) according to Clinical & Laboratory Standards Institute were as follows: doxycycline S≤4, R≥8; erythromycin S≤1, R≥4; ciprofloxacin S≤1, R≥2.
S, susceptible; R, resistant; MH, Mycoplasma hominis; UU, Ureaplasma urealyticum.
![]()
In 166 non-pregnant women, the positive culture results were as follows: MH only, n=10 (6%); UU only, n=49 (29.5%); and both MH and UU, n=32 (19.3%). The susceptibilities of MH only to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 100%, 10%, 40%, and 0%, respectively. The susceptibilities of UU only to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 93.9%, 89.8%, 6.1%, and 79.6%, respectively. The susceptibilities of both MH and UU to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 96.9%, 6.3%, 12.5%, and 12.5%, respectively (Table 4).
Table 4
Antimicrobial susceptibilities (%) of Mycoplasma hominis and Ureaplasma urealyticum for non-pregnant women (n=166)

Values are presented as number (%). The breakpoints (mg/L) according to Clinical & Laboratory Standards Institute were as follows: doxycycline S≤4, R≥8; erythromycin S≤1, R≥4; ciprofloxacin S≤1, R≥2.
S, susceptible; R, resistant; MH, Mycoplasma hominis; UU, Ureaplasma urealyticum.
![]()
In 34 pregnant women, positive culture results were as follows: MH only, n=0 (0%); UU only, n=9 (26.5%); and both MH and UU, n=4 (11.8%). The susceptibilities of MH only to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 0%, 0%, 0%, and 0%, respectively. The susceptibilities of UU only to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 100%, 77.8%, 0%, and 88.9%, respectively. The susceptibilities of both MH and UU to doxycycline, erythromycin, ciprofloxacin, and azithromycin were 100%, 0%, 0%, and 0%, respectively (Table 5).
Table 5
Antimicrobial susceptibilities (%) of Mycoplasma hominis and Ureaplasma urealyticum for pregnant women (n=34)

Values are presented as number (%). The breakpoints (mg/L) according to Clinical & Laboratory Standards Institute were as follows: doxycycline S≤4, R≥8; erythromycin S≤1, R≥4; ciprofloxacin S≤1, R≥2.
S, susceptible; R, resistant; MH, Mycoplasma hominis; UU, Ureaplasma urealyticum.
![]()
Discussion
MH only infection accounted for about one-sixth of UU infections in this study. The study population seemed to be mainly infected with UU. Doxycycline was still the best antibiotic because those with positive culture results for UU only, MH only, and both MH and UU showed susceptibilities. More than 80% of UU infections alone were sensitive to erythromycin and azithromycin, whereas less than 12% of MH and both MH and UU infections were sensitive to erythromycin and azithromycin. The susceptibility of UU only and both MH and UU to ciprofloxacin was only less than 12%.
In this study, the incidence of MH, UU, both MH and UU infection and antimicrobial susceptibilities were similar between pregnant and non-pregnant women.
Organisms other than Chlamydia trachomatis and Neisseria gonorrhea, particularly UU, may be detected more frequently in patients with pelvic inflammatory disease in a Korean study. In addition, identification of MH may be important in female health problems such as Fitz-Hugh-Curtis syndrome [16]. MH and UU infection can cause urethritis and increase the risk of vaginitis, abnormal vaginal bleeding, and foul vaginal odor. MH, like UU, is commonly found in the urinary and genital tracts. In most cases, people with MH or UU infection do not have any symptoms. If there are any symptoms, they include difficulty and pain during urination, and discharge of fluid from the urethra. In women, the symptoms are vaginal discharge and dysuria. In men, the symptoms are urethritis, dysuria, and discharge. Besides symptoms, an indication for a laboratory test is a high-risk sexual behavior. All sexual contacts within the preceding 6 months of the onset of symptoms or diagnosis should ideally be evaluated, tested, and treated. Test-of-cure samples should be collected no earlier than 3 weeks after the start of treatment [17].
The major problem is that pregnant women infected with both MH and UU are not sensitive to erythromycin or azithromycin at all. The role of MH and UU in premature births may be related to their ability to induce inflammatory cytokines, thereby triggering pathways leading to preterm labor. The role of MH and UU in adverse pregnancy outcomes is increasingly accepted. However, the sole presence of these microorganisms in the vaginal flora might be insufficient to cause pathological issues. Other factors such as bacterial vaginosis or cervical incompetence may be additionally needed to induce preterm birth [18]. According to a Russian study, josamycin was inferior to azithromycin in terms of a number of pharmacologic parameters, compliance, and safety. Therefore, josamycin should not be used in pregnant women [19]. Doxycycline became immediately popular after its Food and Drug Administration approval in 1967 because of its simplified once (or twice)-a-day dosage regimen rather than the 4 times daily dosing scheme for tetracycline. Doxycycline was developed after tetracyclines had been labeled as potentially harmful because of severe adverse effects, including teratogenicity, permanent yellowish-brown teeth discoloration after in utero exposure and in children under 8 years of age, and, very rarely, fatal hepatotoxicity in pregnant women [20]. There is no evidence in the current literature of any human teratogenicity following the use of doxycycline during pregnancy [21]. Cumulative evidence suggests that the use of doxycycline during the first trimester is not associated with increased risk in the growing fetus [22]. Although many studies have reported that the use of doxycycline in early pregnancy has a low risk of causing malformations, there is insufficient data to conclude that there is no danger; thus, more research is needed.
Among pregnant women with preterm labor, the duration of pregnancy was prolonged in MH- and UU-negative group than in positive groups [23]. Prepregnancy and early pregnancy screening for genital mycoplasmas and subsequent treatment may reduce preterm deliveries [24]. In our study, erythromycin and azithromycin were still active against UU. However, quinolone derivatives such as ciprofloxacin were inactive against UU. Only doxycycline was active against both MH and UU.
Compared to that in previous studies, the susceptibility to ciprofloxacin and azithromycin was significantly reduced in UU only and both MH and UU infections in this study. However, erythromycin and azithromycin were inactive against MH. Although small in number, the positive culture rates of MH, UU, and both MH and UU in pregnant women in Cheonan with preterm labor or PROM were 0%, 26.5% and 11.8%, respectively. In 2009, Koh et al. [25] reported that 44.2% of pregnant women in Jinju had genital mycoplasma infection. In 2004, Kim et al. [26] reported that infection with MH was a significant factor in preterm labor and PROM. Further, in 2014, Kwak et al. [27] reported that the prevalence of positive vaginal fluid cultures for genital mycoplasma was 62.5% (112/179). This group included 99 patients infected with only UU and 13 patients infected with both MH and UU. No patients were found to be infected with only MH. Compared with patients only positive for UU, patients with positive for both organisms showed significantly decreased gestational age at birth and neonatal birth weight, and significant increases in the incidences of preterm birth, neonatal intensive care unit admissions and histologic chorioamnionitis [27]. In pregnant women, UU and both MH and UU infections were resistant to ciprofloxacin but susceptible to doxycyline. Characteristically, the susceptibility of UU to erythromycin and azithromycin was 77.8% and 88.9%, respectively. Azithromycin is the empirical treatment regimen for pregnant women in our geographic region.
In our symptomatic non-pregnant women (n=166), the positive culture rate was 6% for MH, 29.5% for UU, and 19.3% for both MH and UU. In 2016, Kwon et al. [28] reported that the positive culture rate in symptomatic non-pregnant women (n=186) from vaginal swab sample was 11.8% for MH and 65.6% for UU. These infection rates are much higher than those in our study. However, the MH infection rate was one-sixth of the UU infection rate, which is similar to our study. UU was still the leading causative pathogen for genitourinary infection in our study, as in other studies [29]. The use of empirical antibiotics can be ineffective owing to resistance to antibiotics. It is difficult to establish common guidelines for empirical treatment of genital MH and UU infections. With respect to the value of this research, we examined symptomatic patients and determined the antimicrobial susceptibilities for genital MH only, UU only, and both MH and UU in Cheonan, which can represent a specific geographic region, rather than the whole country. Nevertheless, we have achieved the following 2 important findings. First, compared with previous studies, the susceptibility to ciprofloxacin was significantly reduced when UU only and both MH and UU infections were present. Moreover, the susceptibility to azithromycin was significantly reduced when MH only and both MH and UU infections were present. Therefore, the empirical use of ciprofloxacin and azithromycin should be avoided in patients infected with MH, UU, and both MH and UU. Second, the MH infection rate was about one-sixth of the UU infection rate, and antibiotics other than doxycycline and ciprofloxacin have less than 10% susceptibility. Efforts should be made to reduce the rate of MH and UU infection by conducting epidemiological studies. Planning pregnancy is the best way to treat infection before pregnancy. However, if only doxycycline is effective during pregnancy, much attention should be paid to which antibiotics should be used.
A nationwide survey may enable us to establish new guidelines for treating genital mycoplasma infections in Korea. This study collected many patients over the past 16 months between January 1, 2017, and April 30, 2018, with age ranging from 10 to 87 years. Empirical treatment without isolation or identification of genital MH and UU would fail in many cases. In vitro determination of antimicrobial susceptibility of genital MH and UU in each clinical case is required to avoid therapeutic failures.
 XML Download
XML Download