

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Stress urinary incontinence (SUI), a common health problem in women, affects approximately 2.1 million Korean women [1]. Female sexual dysfunction (FSD) is another common condition with a prevalence of 43% in sexually active women between the ages of 18 and 59 [2]. The reported prevalence of FSD in women with and without urinary incontinence (UI) is 59.6% and 43.5%, respectively [3]. Loss or disruption of supportive structures such as the pelvic musculature or the periurethral vascular plexus, dysfunctional urethral closure, and/or loss of urethral integrity, contribute to SUI [456]. Surgical procedures for SUI treatment aim to provide support in the mid-urethral region similar to ligamentous support. Mid-urethral sling procedures, such as tension-free vaginal tape (TVT) and transobturator tape (TOT) operations, are gold standards for the surgical treatment of SUI.
In TOT surgery, a sling is placed such that it traverses the obturator foramen whereas TVT surgery involves placing a sling posterior to the pubic bone. Results of studies on the effect of TOT surgery on FSD have been conflicting. A few studies reported improvement in sexual function following TOT [789] while others reported overall improvement without statistical significance [101112] or no change at all [131415]. No study has investigated the relationship between TOT surgery and sexual function using disease-specific validated questionnaires in the Korean population. The purpose of this study was to evaluate the effect of TOT surgery on sexual function in women with UI.
Materials and methods
This retrospective cohort study included women who underwent TOT surgery between March 2010 and December 2014 at the Kyung Hee University Hospital at Gangdong. The same surgeon performed all the procedures. Women were excluded from the study for any of the following: 1) sexual inactivity before surgery; 2) major gynecological surgery affecting sexual function (hysterectomy or surgery for pelvic organ prolapse) at the same time as TOT surgery; or 3) cancer diagnosis before or after TOT surgery. Of the 206 women who underwent TOT surgery, 82 (39.8%) met the inclusion criteria. The demographic details of all eligible women were obtained from their medical records. The information included age, parity, body mass index, duration of UI, history of hysterectomy, menopausal status, history of menopausal hormone therapy, and history of hypertension, diabetes and thyroid disorders. All the women underwent urogynecological examination, assessment of pelvic organ prolapse using the International Continence Society's Pelvis Organ Prolapse Quantification system [16], and the multichannel urodynamic study.
The validated Korean versions of the Pelvic Floor Distress Inventory-20 (PFDI-20) and the Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12 (PISQ-12) were used to assess pelvic floor and sexual dysfunction, respectively [1718]. All questionnaires were completed preoperatively and at least 6 months postoperatively. The PISQ-12 consisted of 3 domains: behavioral-emotive (items 1–4), physical (items 5–9), and partner-related (items 10–12) domains. The response to each item was assigned 0–4 points, with a total score of 0–48 points. The higher the PISQ-12 score, the better the quality of sexual function. Question 6 of the PISQ-12 was used to identify patients with leakage of urine during sexual intercourse (coital incontinence [CI]). The women who chose 1 of “usually, always or sometimes” in response to question 6 of PISQ-12 and women with CI were assigned to the CI group. The PFDI-20, a shorter version of the PFDI, is a comprehensive questionnaire designed to assess symptoms of pelvic floor disorders in women. This 20-item questionnaire comprises 3 scales: a urinary, a colorectal, and a pelvic organ prolapse scale. Each item is assigned 0–4 points. The higher the PFDI-20 score, the worse the symptoms.
The TOT operation was performed under spinal or general anesthesia with a vertical incision made along the middle of the urethra on the anterior vaginal wall. The obturator foramen was palpated, and a skin incision was made in the medial cranial region of the obturator foramen on both sides. An introducer was inserted, and the tape was threaded and withdrawn from the opposite side. After cutting the tape remnant, the vaginal wall and both skin incisions were sutured.
Data are presented as mean±standard deviations, medians (ranges), or numbers (percentages). All statistical analyses were performed using the SAS software, version 22.0 (SAS Institute, Cary, NC, USA).
The changes of scores of PFDI-20 and PISQ-12 were analyzed with paired t-test. And the plot was analyzed for correlations between pre- and postoperative sexual functions. To identify the factors affecting postoperative sexual function, multivariate regression analysis using forward selection and backward elimination was conducted to find the best model for postoperative PISQ-12 scores and a P-value less than 0.05 was considered statistically significant.
Results
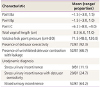
Eighty-two women (39.8%) met the inclusion criteria and completed the PFDI-20 and PISQ-12 questionnaires pre- and postoperatively over a mean period of 9 months (range: 6–17 months). Table 1 shows the baseline characteristics of the patients. The mean age of the study group was 51 years and approximately 50% of the women were menopausal. Table 2 shows the results of pelvic organ prolapse quantification measurements and urodynamic study. The majority of the study population were diagnosed with mixed UI.
Table 1
Baseline characteristics

![]()
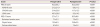
Table 2
Anatomical and urodynamic findings
Points Ba and Bp are defined as the lowest points of the prolapse of anterior and posterior vagina respectively. Point C is location of cervix or vaginal cuff. Each point is measured in centimeters above or proximal to the hymen (negative number) or centimeters below or distal to the hymen (positive number) with the plane of the hymen being defined as zero.
![]()
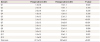
Statistically significant improvements were observed in the PFDI-20 and PISQ-12 scores (Table 3). The PFDI-20 score decreased significantly from 92.3±63.2 preoperatively to 30.2±30.9 postoperatively (P<0.001), and the PISQ-12 score increased significantly from 27.1±7.3 preoperatively to 30.5±6.8 postoperatively (P<0.001). The improvements were prominent in the physical and partner-related domains of the PISQ-12 questionnaire and were notably found in questions 1, 6, 7, 8, 11, and 12 (Table 4).
Table 3
Changes of Pelvic Floor Distress Inventory-20 and Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12 outcomes after transobturator tape surgery
Data are presented as means±standard deviations.
PFDI-20, Pelvic Floor Distress Inventory-20; POPDI, Pelvic Organ Prolapse Distress Inventory; CRADI, Colorectal-Anal Dysfunction Inventory; UDI, Urinary Distress Inventory; PISQ-12, Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12.
![]()
Table 4
Changes in each item score of Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12 after transobturator tape surgery
![]()
Fig. 1 shows the paired profiles for pre- and postoperative PISQ-12 scores. The paired postoperative PISQ-12 scores showed a tendency to increase. Fig. 2 shows the linear relationship between the pre- and postoperative PISQ-12 scores. A positive linear relationship is observed with a concurrent increase in both variables. The scatterplot shows a positive correlation of 0.492 between the 2 variables (P<0.001). This means that the overall postoperative sexual function improved with statistical significance even though women with low levels of preoperative sexual function continued to show low levels of sexual function postoperatively, and women with high levels of preoperative sexual function continued to show high levels of sexual function postoperatively.
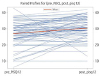 | Fig. 1Plot of paired profiles for pre- and postoperative Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12 scores.PISQ-12, Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12.
|
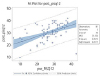 | Fig. 2Linear relationship between the pre- and postoperative Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12 scores.DF, degrees of freedom; MSE, mean squared error.
|
CI and preoperative Urinary Distress Inventory (UDI) score significantly affected postoperative sexual function in women who underwent TOT surgery for UI as shown in the multivariate regression analysis (Table 5).
Table 5
Multivariate regression analysis performed for factors affecting changes in the

| Variable | β | SE | t | P-value |
|---|---|---|---|---|
| Preoperative UDI-6 | −0.07 | 0.03 | −2.55 | 0.013 |
| CI group | −4.15 | 1.57 | −2.64 | 0.010 |
Pelvic Organ Prolapse/Urinary Incontinence Sexual Function Questionnaire-12 scores after transobturator tape surgery
UDI-6, Urinary Distress Inventory-6; CI group, the women have responded as “usually or always or sometimes” in the question 6 of PISQ-12 who leaks urine with sexual activity were regarded as C group; SE, standard error.
![]()
Discussion
The strength of our study is that it evaluated sexual function using disease-specific validated questionnaires and used multivariate analysis to determine the factors affecting sexual function.
The limitation of our study is that a single disease-specific validated questionnaire cannot sufficiently reflect the multidimensionality of sexual function. In addition, our study was hospital-based, retrospective, and had a small study sample meaning that our findings cannot to be applied to the general population.
There has been much concern that placing a sling between the urethra and the anterior vaginal wall may adversely affect neural pathways and could lead to disturbances in sensation, lubrication, and orgasm or that the sling itself, consisting of synthetic tape, may alter the pliability of the vagina, thereby causing dyspareunia or even pain for the partner. Furthermore, it is likely that the tape placement methods (TVT and TOT) affect postoperative sexual function differently. Most of the articles on postoperative sexual function show mixed results with TVT, TOT, and TVT inside-out approaches using heterogeneous questionnaires. Jha et al. [19] reported their review of a meta-analysis that included 1,578 women who underwent a mid-urethral sling operation. They observed that sexual function improved in 33.9%, deteriorated in 9.4%, and remained unchanged in 56.7% of the women postoperatively. With regard to exclusive TOT surgery, a few studies reported improved sexual function postoperatively [891013], while others reported no improvement or difference [1415]. The study by Liang et al. [14] evaluated sexual function after TOT surgery using the PISQ questionnaire and reported no overall change in sexual function but significant delay in orgasm attainment. In contrast, our study showed statistically significant improvement in sexual function after TOT surgery.
Our study results show that the overall sexual function significantly improved after TOT surgery based on the total PISQ-12 score. Of the 3 domains of the PISQ-12 questionnaire, significant improvements were observed in 2, namely the physical and partner-related domains, but not in the behavioral-emotive domain. CI and preoperative UDI-6 score were found to affect postoperative sexual function. In other words, the presence of CI and preoperative urinary distress symptoms are grounds to predict significant improvement in postoperative sexual function in women undergoing TOT surgery. The subsidence of CI or significant improvement of urinary distress symptoms after TOT surgery relieves distress from sexual activity in many women with UI.
CI is an underrated symptom with a reported incidence of 10–27% [20]. In our study, the rate of CI expressed as “always, usually or sometimes” in the PISQ-12 questionnaire was 47% (38/81). The rate of CI was surprisingly higher in our study because the PISQ-12 questionnaire was self-administered.
The exact pathophysiology of CI is unclear. Hilton [21] classified CI into 2 groups: CI on penetration and CI at orgasm. The incidence of SUI and the incidence of detrusor instability were found to be high in CI on penetration and CI at orgasm, respectively. Serati et al. [22] also reported a strong correlation between CI at orgasm and detrusor overactivity (DO). Khan et al. [23] suggested that this correlation can be explained by the fact that CI is essentially a severe form of DO and that orgasm triggers involuntary contraction of the detrusor. In our study, we did not determine whether the time of CI occurrence was on penetration or at orgasm. Contrary to the results of the aforementioned studies, the functional study by El-Azab et al. [24] revealed that CI prevalence was significantly higher in women with SUI than in those with DO. They also found that CI was strongly associated with parity, prolapse, and SUI. Furthermore, CI showed a strong positive correlation with SUI severity and a strong negative correlation with abdominal leak point pressure [24]. This means that CI is an extension of SUI and an involuntary symptom caused by urethral sphincter insufficiency. The improvements in DO and SUI observed in UI patients who underwent surgery may be associated with improvement in CI which may help improve sexual function. Our study results agree with those of previous studies in this regard.
In conclusion, TOT surgery provides support to the mid-urethra and reduces UI and DO leading to significant improvements in CI and UDI scores which translate into significant improvements in sexual function.
 XML Download
XML Download