

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Prostate cancer (PCa) is the most common cancer and the second leading cause of cancer death in men in the USA and Europe.1 In Korea, its rate of incidence has increased 20 times over the past two decades.2 Currently, the American Urological Association (AUA) does not recommend routine prostate specific antigen (PSA) screening in men under 54 years of age and considers screening only for men who are at an increased risk for PCa, such as those with positive family histories or African-American men between the ages of 40 and 54 years.3 Similarly, the European Association of Urology (EAU) recommends offering PSA testing in men > 50 years.4 For men > 45 years of age, the EAU recommends screening for individuals who have a family history of PCa or African-Americans.
As for PCa in young men, prior reports have shown differences in pathological characteristics between younger and older men, although the results have been contradictory.567 Studies conducted before the PSA era have suggested that younger patients harboured more aggressive tumour characteristics than older people.5 More recent reports, however, have shown that younger patients with PCa had more favourable pathologic features on the radical prostatectomy (RP) specimen than older people.67
Currently there is a paucity of studies on the clinicopathological characteristics of PCa in individuals under 50 years of age in Asians, especially Korean men. Generally, it is well-known that patients with PCa in Asian countries present with more aggressive pathologic behaviours, in contrast to Western men.89 Accordingly, it is crucial to determine the pathologic features and prognosis of young patients with PCa in the Asian population. To address these issues, using a recent prostatectomy database, we analysed the clinicopathological characteristics of a multi-centre cohort of Korean men with PCa, comparing patients < 50-year-old to patients ≥ 50-year-old. To the best of our knowledge this is the first report on this issue in the Korean population.
METHODS
Demographics and clinicopathological data
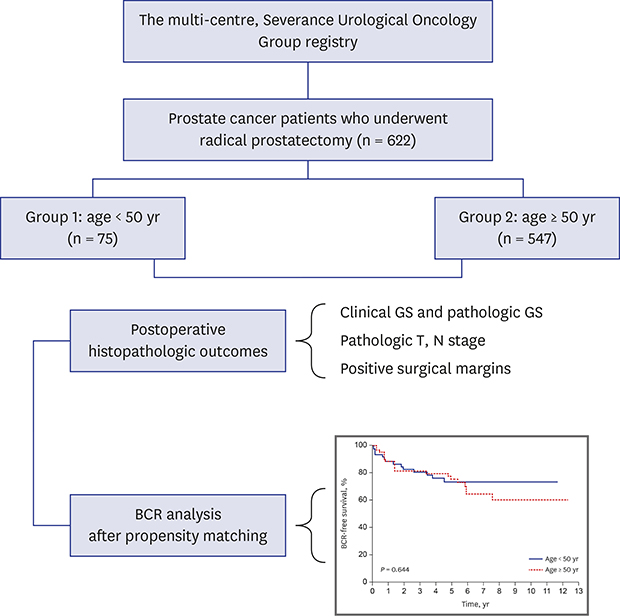
A total of 639 consecutive Korean patients with localized or locally advanced PCa who were treated by RP between 2001 and 2017 were selected from the multi-centre, Severance Urological Oncology Group PCa registry. Of these individuals, patients with missing demographic variables and inadequate follow-up data were excluded. Patients who received preoperative androgen deprivation or radiation therapy were also excluded. This resulted in a final study population of 622 men, of whom 75 (11.3%) were aged < 50 years at diagnosis. PSA testing was performed in patients with unspecific LUTS, a family history of PCa, or as part of a routine check-up examination by referring urologists.
We obtained data on patient demographics and clinical characteristics, including preoperative PSA values, clinical T stage, and biopsy Gleason score (GS) (Table 1). PSA values were collected at baseline, six weeks, and then every three months for the first year after surgery, and every six months during years two and three, and yearly thereafter. As for adjuvant therapy (radiation or androgen deprivation therapy) for patients with postoperative adverse pathologic features (e.g., positive surgical margin [PSM], seminal vesicle invasion, extracapsular extension) or for pathological node positive patients, we performed radiation therapy when the patient showed biochemical recurrence (BCR) during follow up.
Table 1
Demographic and preoperative characteristics between the 2 groups

SD = standard deviation, BMI = body mass index, CAD = coronary arterial disease, CVA = cerebrovascular accident, IPSS = international prostatic symptom score, TRUS = transrectal ultrasound, PSA = prostate specific antigen, GS = Gleason score.
![]()
Pathological outcomes were assessed using the American Joint Cancer Committee (AJCC) 2010 staging system.10 Tumour grading was classified using the Gleason grading system (1992–2005) and the revised 2005 Gleason grading system afterwards.11 Pathological analysis of RP specimens was performed as follows: prostates were inked along their surface area, and surgical margins were considered positive when carcinoma cells were in contact with the inked specimen surface. BCR was defined as PSA rising above 0.2 ng/mL after the post-treatment nadir.
Study endpoints
The main goal of this study was to compare the pathological characteristics (including pathologic GS, pathologic T stage, rate of PSM and BCR) of PCa between Korean men < 50-year-old and men ≥ 50-year-old.
Statistical analyses and propensity score matching
Patient preoperative and pathologic characteristics were calculated using means for continuous variables and proportions for categorical variables. Student's t-test was used for continuous variables, and χ2 tests or Fisher's exact tests were used to compare categorical variables between groups. Median and interquartile range were used for follow-up data.
For BCR analysis, propensity score matching was conducted, because the number of patients in each group was quite different. We adjusted for differences between the groups in patient characteristics that are directly related to BCR. Propensity scores were obtained using binary logistic regression with covariates of baseline PSA, pathologic GS, pathologic T stage, pathologic N stage, and surgical margin status. Subsequently, 65 well-matched pairs were created. The propensity scoring and matching process were performed with the R statistical software (R Foundation for Statistical Computing, Vienna, Austria) essential package for SPSS. The matching procedure was performed using the “MatchIT” package in R. Matching with replacement was performed, and propensity score with an absolute bias measure of < 0.2 was obtained. To compare BCR-free survival (BFS) among the two groups, the Kaplan–Meier method with the log-rank test was used.
Statistical analyses were performed with the SPSS for Windows software (version 13.0; SPSS Inc., Chicago, IL, USA). Values of P < 0.05 were considered to indicate statistical significance.
RESULTS
Of the patients who underwent RPs, 622 had clinical, demographic, and follow-up data that were eligible for the analyses. Of the patients who were eligible for the study, 75 (11.3%) were 50 years of age or younger, and 547 (88.7%) were older than 50 years. In the younger cohort, prostate biopsies were performed for elevated PSA in 23 patients (30.5%) and abnormal digital rectal examination in 52 patients (69.5%). The mean age of the younger cohort was 45.9 ± 0.3, compared with 64.5 ± 0.2 in the older group. There were no significant differences in body mass indexes (BMIs) and comorbidity distributions between the two groups. A family history of PCa was present in a larger proportion of the younger cohort than the older cohort, although this difference was not statistically significant. The younger patients had a lower total IPSS score (P = 0.020) and a lower prostate volume on TRUS (P < 0.001), compared to the older group. The baseline PSA value, biopsy GSs, and clinical T stages-are shown in Table 1.
Histopathologic characteristics were similar between the two cohorts, with the exception of lower prostate weight in younger patients (31.8 ± 1.9 vs. 37.2 ± 1.6; P < 0.001). Specifically, patients in the younger cohort had similar GSs after pathologic evaluations, as shown Table 2. Pathologic T stage and PSM rates were similar between the two cohorts. Although upgrades in GSs after pathologic prostatectomy tissue examinations were present in a larger proportion of the younger cohort than the older cohort (32.0% in younger and 24.9% in older patients), this difference did not achieve statistical significance (P = 0.088). Pathologic upstaging rates were similar between the two groups (Table 2). In the younger age group, 49.4% of the patients had a pathologic GS of 7, 13.3% had a pathologic GS ≥ 8, and 30.7% had locally advanced stages (≥ pT3).
Table 2
Postoperative histopathologic outcomes between the 2 groups
SD = standard deviation, GS = Gleason score, PSM = positive surgical margin, IQR = interquartile range.
![]()
Before propensity matching, BFS was observed in 82.4% and 75.6% (2- and 5-year, respectively) of patients in the younger age group and 86.9% and 77.7% (2- and 5-year, respectively) in the older age group. Table 3 shows the patients characteristics after further analysis with propensity score matching, to compare BCRs between the two groups. The created 65 pairs showed an almost equivocal distribution, compared with the initial distribution (before propensity matching, PSA in Table 1 and pathologic GS, pathologic T, N stage and PSM in Table 2). Biochemical disease-free survival was not different in the matched dataset (P = 0.644) (Fig. 1).
Table 3
Patient characteristics after propensity matching for BCR analysis
BCR = biochemical recurrence, PSA = prostate specific antigen, SD = standard deviation, GS = Gleason score, PSM = positive surgical margin.
![]()
DISCUSSION
Before the PSA era, it was traditionally believed that the early onset of PCa is biologically different from late onset PCa. In 1972, a study12 firstly reported worse prognosis for men who are diagnosed with PCa before 50 years of age. Subsequently, similar studies demonstrated that younger patients with PCa have more aggressive phenotypes. Regarding the mechanism underlying the worse prognosis of the younger age group, several authors have suggested that germline mutations associated with aggressive PCa are more common in younger men than in older age groups.
More recently, however, several authors pointed out that most of the previous studies supporting such hypotheses mainly included patients before the PSA era. They reported that their analyses revealed contradictory results,67131415 demonstrating that younger patients had better oncologic outcomes than corresponding older cohorts. Becker et al.7 reported that men aged < 50 years were more likely to present with organ-confined (84.2% vs. 68.4%; P < 0.001), low-grade (GS < 7) tumours (33.1% vs. 28.7%; P < 0.001), as well as lower rates of PSMs (11.5% vs. 16.8%; P = 0.002) on their RP specimen, compared to the older group. Parker et al.6 also showed that younger (< 50–year-old) cohort more commonly had organ-confined disease and pathologic GS ≤ 6 than older cohort. Similarly, Smith et al.13 reported that patients (< 50–year-old) in the PSA era who underwent RP more commonly had organ-confined disease and had a more favourable disease-free outcome compared to older men.
On the other hand, for patients with metastatic PCa at diagnosis, several reports1617 have found that younger (< 50-year-old) patients have more aggressive tumours and higher cancer-specific mortalities (CSS) than older men. Some authors emphasized that prior reports predominantly examined only RP outcomes, and such studies may have underestimated the disease aggressiveness of young patients with PCa over time.15 Thorstenson et al.16 reported a striking association between younger age and higher CSS among patients aged < 50–55 years with metastasis at diagnosis. They suggested that metastatic PCa diagnosed before this age is often biologically different from that of older people, and a rapidly metastasizing form of PCa seems to be more common in younger age groups than in older populations. A recent report from the STAMPEDE (Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy) trial also revealed a worse prognosis in younger men than in older men with metastatic PCa.17 Therefore, several authors have worried about the recent increase in the incidence of young patients with PCa who were diagnosed at a metastatic stage.1518
For Asian patients with PCa, there has been limited data. Huang et al.19 compared the pathological characteristics and prognosis of patients with PCa in Taipei, between young and old age groups, and reported that patients with PCa aged < 50 years showed similar tumour grades, stages, PSA values, overall survival (OS), and BFSs to the older aged group. The Chinese study of Xu et al.8 reported that patients with PCa aged < 55 years are more likely to be diagnosed at an advanced stage, and their pathologic patterns were mostly complicated and associated with a high degree of malignancy. They demonstrated that the five-year OS of their younger group was significantly lower than that of European and American populations. The authors emphasized the need for a screening system for Chinese population suitable for clinical practice focusing on high-risk people aged ≤ 55 years.
It is well known that patients with PCa in Asian countries present with more aggressive pathologic features, compared with Western men.89 Man et al.9 reported that a greater proportion of Asian people had a high risk PCa compared with non-Asian men. The percentage of PCa with GS ≥ 8 was twice as high in Asian patients than in non-Asians at presentation (26.5% vs. 13.8%, respectively). Especially for Korean patients, PCa in Korean men is known to be more aggressive and exhibit poorer differentiation, regardless of the initial serum PSA level or clinical stage at presentation, compared to Western men.20 This finding was supported by subsequent studies, which analysed the application of the Epstein criteria to Korean patients with PCa. Several studies reported that Korean patients with PCa who fulfilled the Epstein criteria might not always behave as clinically insignificant PCa.2122 Similarly, Lee et al.23 reported that almost 50% of their patients who were initially regarded as active surveillance (AS) candidates had significant PCa after pathologic examination, although the authors used a combination of four factors (biopsy GS ≤ 6, volume of the largest cancer < 50%, PSAD ≤ 0.15 ng/mL/mL, and serum PSA ≤ 10 ng/mL).
The findings of the present study are in line with previous studies,1924 which demonstrated similar GS and disease stages between the two age groups. In our study, the biopsy GS in the young age group was significantly lower than in old age group (Table 1). However, GS upgrades after pathologic prostatectomy specimen examination was present in a larger proportion of the younger cohort than in the older cohort. Hence, the pathologic distribution of GS (Table 2) in our study was similar between the two groups. Such findings (high incidence of GS upgrading) are consistent with a previous study of a large, single-surgeon cohort.25
Additionally, we analysed the rate of upgrading of GS or T stage in men who fulfilled AS criteria, in the younger age group. Of the 75 patients in the younger age group, 15 men fulfilled AS criteria (such as protocol from Memorial Sloan-Kettering Cancer Center [MSKCC])26 or Prostate Cancer Research International: Active Surveillance (PRIAS)27, with a combination of six factors (biopsy GS ≤ 6, clinical stage T1c-T2, serum PSA ≤ 10 ng/mL, PSAD ≤ 0.2 ng/mL/mL, number of positive cores ≤ 2 and single core involvement ≤ 50%). Notably, of the 15 men who fulfilled the AS criteria in the younger age group, five patients (33%) showed upgrading of GS or T stage in the final pathology. This finding suggests the need for caution when physicians recommend AS for young patients with PCa.
Currently, AUA and EAU recommend routine PSA screening in men ≥ 54 years of age and > 50 years of age, respectively.34 For younger population, both guidelines do not recommend routine PSA tests, but only for men with positive family histories or African-Americans. As for the role of PSA screening, the United States Preventative Service Task Force (USPSTF) has commented against the wide-spread use of PSA for the general population as a cancer screening tool, owing to ineffectiveness in lowering mortality.28 However, the USPSTF recommendation was argued by subsequent reports, which demonstrate its methodological flaw (inaccurate interpretation of data)25 and the potential harmful effect that can be caused by it. For example, Pompe et al.15 recently examined the Surveillance, Epidemiology, and End Results (SEER)-database (from 2004 to 2013) and reported an increased incidence of de novo metastatic disease at presentation, which might result from the decreased use of PSA screening after release of the USPSTF.
The main objective of this study was to analyse pathological characteristics of PCa on RP specimen in Korean men < 50 years of age. In our analysis, young patients with PCa did not exhibit more favourable tumour characteristics than older men. Adverse pathologic features were not rare in the younger group, including 30.7% with locally advanced disease, 49.4% with a pathologic GS of 7, and 13.3% with pathologic GS ≥ 8. These features were similar to those of the older group of patients (Table 2). Accordingly, a possible explanation may be that PSA screening in men younger than 50 years can identify significant PCas with a considerable proportion. In addition, a considerable number of patients in the younger group revealed postoperative GS upgrading or pathologic upstaging, although they were initially regarded as AS candidates. Taken together, these findings suggest that young (< 50-year-old) patients with PCa in the Korean population should not be omitted, nor underestimated, when deciding treatment options.
The present study had several limitations. 1) While the number of participants in the present study is quite large, the actual number of patients aged < 50 years is small, although we included a higher proportion (11.3% in present study) of younger patients with PCa than previous studies.71425 In the report of an Australian study,14 only 2.6% of the primary patient population were included in the younger (< 50–year-old) group. Similarly, other studies included 3.3%7 and 10.8%25 of patients in younger age groups. Moreover, we conducted propensity score matching to overcome the inevitable selection bias when analysing BCR between the two groups. 2) Despite the large number of patients, patients are usually referral based. Consequently, it is impossible to make epidemiologic conclusions from our data. 3) It is possible that younger patients with PCa with more advanced disease were referred for surgery, whereas others with very low-risk diseases were put on AS protocols. Likewise, it is possible that older patients with PCa with higher-risk diseases were referred for radiotherapy. Future studies with a larger number of patients (especially younger men aged < 50 years) will be needed to confirm our results.
As for adjuvant therapy for pathological node positive patients, 2018 National Comprehensive Cancer Network (NCCN) guideline recommend observation as category 2A option (for patients with very-low risk or low risk PCa) or category 2B option (for patients with intermediate, high, or very-high risk PCa).29 This recommendation was based on the previous report which demonstrated that initial observation could be a safe option in men with N1 disease at RP, during postoperative 10-year follow-up.30 For these reasons we did observation for these patients until they showed BCR, although category 1 recommendation is adjuvant androgen deprivation therapy.
In conclusion, this study represents the first description of the pathologic characteristics of Korean men < 50 years with PCa. Contrary to prior reports, young patients with PCa did not exhibit more favourable tumour characteristics on RP specimen than older men, in the Korean population. BCR-free survival rates were also similar between the two groups. Adverse pathologic features were not rare in the younger group. Moreover, the younger age group showed postoperative upgrading of GS frequently. We suggest that these findings should be kept in mind when deciding the treatment options for young (< 50-year-old) patients with PCa in the Korean population.
 XML Download
XML Download