

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spirochetes were reported in 1719 by van Leeuwenhoek who detected lively moving spiral “animalcules” in his own feces [1]. Spirochetes are classified into 3 phylogenetic groups: Spirochaetaceae (including Borrelia, Spirochaeta, Spironema, and Treponema), Leptospiraceae (Leptonema and Leptospira), and Brachyspiraceae (Brachyspira aalborgi and Brachyspira pilosicoli). B. aalborgi and B. pilosicoli are most commonly associated with human intestinal spirochetosis. B. aalborgi was first recognized in Denmark in 1982 [2]. During the 90s, stools of patients examined by multilocus enzyme electrophoresis showed a predominance of B. pilosicoli [34].
Intestinal spirochetosis is a rare infection in children. The term intestinal spirochetosis was used for the first time by Harland and Lee in 1967 [5]. They described a “forest of organisms” on the surface of the epithelium of an adult patient with chronic diarrhea lasting for more than 3 years based on electron microscopy. Adhesion of spirochetes to the brush border mucosa results in thickening of the brush border. Histological appearance is the hallmark of this infection [6].
We performed a search between 2004 and 2014 in the database of our pediatric gastroenterology unit for all cases of intestinal spirochetosis. We also performed a review of the literature through PubMed search using terms of “Human intestinal spirochetosis” and “Children” (filter English). This search resulted in 39 publications. We limited our search to the last 20 years.
CASE REPORT
Case 1
A 4-year-old boy was referred because of a history of bloody stools for 8 months. Before referral, a stool culture had shown Campylobacter jejuni which was adequately treated with antibiotics (Table 1). Control culture was negative. There was no history of diarrhea or hard stools. However, the boy continued to complain of abdominal pain and the bloody stools persisted. Laboratory investigations showed no biological markers for anemia, a slightly elevated sedimentation rate (27 mm/h), normal C-reactive protein (CRP, 1 mg/L), and normal coagulation. Serology for celiac disease was negative. Colonoscopy revealed rectal irritation. Histology of rectal biopsies showed a few lymphocytes and signs of intestinal spirochetosis confirmed by Warthin-Starry staining (WSS). A 10-day course of amoxicillin-clavulanic acid (50 mg/kg/day) was administered. The blood in the stool disappeared as well as abdominal complaints.
Table 1
Characteristics of patients with intestinal spirochetosis (case reported in this manuscript)

However, 2 months later, he presented at the emergency ward with complaints of bloody diarrhea for 2 days without abdominal pain. A new diagnostic work-up with colonoscopy revealed the presence of a juvenile polyp (JP) at 3 cm from the anal margin and a second one at 20 cm. There were no longer signs of intestinal spirochetosis on biopsies. These polyps were removed. They showed an histology compatible with juvenile polyposis. His symptoms disappeared after removal of polyps. The patient remained asymptomatic during 3 months of follow-up.
Case 2
An 8-year-old boy was presented because of a history of hyperphagia, abdominal pain, chronic diarrhea, and perianal irritation. His complaints started after a recent vacation in Egypt (Table 1). A blood sample showed no signs of anemia or inflammation. A colonoscopy seemed normal. However, biopsies revealed an intestinal spirochetosis.
A treatment with metronidazole was started for 2 weeks. The abdominal pain and hyperphagia disappeared almost immediately. However, diarrhea and perianal irritation resolved gradually in the following weeks. Fifteen months after the initial presentation, the patient had again complaints of hyperphagia, diarrhea, and perianal irritation for 3 weeks. A treatment with metronidazole was administered without performing an endoscopy. After this treatment, he had no longer complaints for 1 year. Afterward, he relapsed, suffering from chronic diarrhea and hyperphagia again without abdominal pain. Therefore, he was treated with metronidazole. This time, metronidazole was administered for 4 weeks. After 4 weeks of treatment with metronidazole, an endoscopy was performed. It showed no signs of intestinal spirochetosis.
Case 3
A 7-year-old boy had non-bloody diarrhea, encopresis, abdominal pain, and peri-anal rash for 18 months. A stool culture was negative. An ultrasound of the abdomen showed no abnormalities (Table 1). Blood results revealed no signs of anemia or inflammation with normal tissue transglutaminase. A lower GI-tract endoscopy revealed mild rectal irritation. Histology of biopsies from the rectum and sigmoid showed signs of intestinal spirochetosis. A treatment with metronidazole at 30 mg/kg/day for 10 days was administered. At a follow-up visit 2 months later, the boy no longer suffered from diarrhea or abdominal pain. However, he still had some complaints of encopresis and anal rash. Control endoscopy showed disappearance of intestinal spirochetosis.
Case 4
A 12-year old boy complained of episodes of abdominal pain, non-bloody diarrhea, and loss of appetite for the last year (Table 1). During initial presentation, a stool culture was negative. Blood sample showed some signs of mild inflammation (CRP, 16.6 mg/L; erythrocyte sedimentation rate, 16 mm/h) and discrete anemia (hemoglobin, 12.1 g/dL; normal range, 13–16.5 g/dL). Although the macroscopic aspect of colonic mucosa was normal, histology showed discrete signs of colitis. No spirochetes were found. His symptoms improved without treatment.
After 7 months, he was reevaluated because of relapsed symptoms. Blood results showed again a moderate elevation of inflammation parameters. Stool culture was positive for Salmonella. Ultrasound and abdominal computed tomography scan showed mesenteric adenitis and colitis. A new endoscopy was performed and the macroscopic aspect of the colon mucosa was normal However, histology showed colon mucosae with proximal and distal zones of mild inflammation and cryptitis. WSS was positive in the caecum and colon transversum. A treatment with amoxicillin and metronidazole was commenced for 10 days. His symptoms disappeared after this treatment.
DISCUSSION
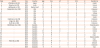
The prevalence of intestinal spirochetosis is correlated with living in a developing region. Prevalence rates of over 30% are seen in Australian aboriginal children. In Australian non-aboriginal children, the prevalence rate is only 1.2% [7]. Several studies have reported prevalence rates ranging from 1.1 to 5% in developed countries [8]. A recent retrospective review from Japan found an even lower prevalence of 0.2% in patients aged less than 20 years [9]. All 4 children described in this article were born and raised in Belgium. None of these children had immigrated to Belgium. Nevertheless, the patient in case 2 developed complaints after a recent stay in Egypt. There seems to be no sex or age prediction except for age under 2 years [7]. This was supported by the finding in our review of the literature that 12 of 27 patients were girls and 15 of 27 patients were boys (Table 2, overview of pediatric cases reported in literature). However, in to our series, all patients were boys. The reason for this remains unclear. It is probably a coincidence.
Table 2
Characteristics of patients with intestinal spirochetosis from literature
| Case | Author | Year | Country | Age | Sex | AP | D | N/V | B | Duration Sx |
|---|---|---|---|---|---|---|---|---|---|---|
| 5 | Ichimata et al. [9] | 2017 | Japan | 9 | F | 1 | 0 | 0 | 0 | >1 (wk) |
| 6 | Ghosh et al. [27] | 2014 | India | 10 | M | 1 | 1 | 0 | 1 | 3 (mo) |
| 7 | Helbling et al. [13] | 2012 | Switzer land | 13 | M | 0 | 1 | 0 | 1 | 1 (mo) |
| 8 | Carpentieri et al. [19] | 2010 | USA | 11 | F | 1 | 0 | 0 | 1 | Unknown |
| 9 | - | 2010 | USA | 6 | M | 1 | 1 | 1 | 1 | 2 (mo) |
| 10 | - | 2010 | USA | 11 | F | 1 | 0 | 0 | 0 | 1 (day) |
| 11 | - | 2010 | USA | 17 | F | 1 | 0 | 0 | 0 | Unknown |
| 12 | - | 2010 | USA | 10 | M | 1 | 0 | 1 | 0 | 1 (wk) |
| 13 | Calderaro et al. [23] | 2007 | Italy | 4 | F | 1 | 0 | 0 | 1 | Unknown |
| 14 | King et al. [26] | 2005 | USA | 9 | M | 0 | 1 | 0 | 1 | 3–4 (mo) |
| 15 | Nodit et al. [28] | 2004 | USA | 9 | M | 1 | 1 | 0 | 1 | Unknown |
| 16 | Marthinsen et al. [16] | 2001 | Sweden | 5 | F | 1 | 1 | 0 | 1 | Several years |
| 17 | - | 2001 | Sweden | 7 | M | 1 | 1 | 0 | 0 | >1 (y) |
| 18 | - | 2001 | Sweden | 4 | F | 0 | 1 | 0 | 1 | 2 (mo) |
| 19 | - | 2001 | Sweden | 10 | F | 0 | 1 | 0 | 1 | 2 (mo) |
| 20 | - | 2001 | Sweden | 13 | M | 1 | 0 | 1 | 1 | 1 (y) |
| 21 | - | 2001 | Sweden | 8 | M | 1 | 0 | 0 | 0 | >1 (y) |
| 22 | - | 2001 | Sweden | 15 | F | 1 | 0 | 0 | 1 | Several weeks |
| 23 | - | 2001 | Sweden | 14 | F | 1 | 0 | 0 | 0 | >1 (y) |
| 24 | Heine et al. [29] | 2001 | Australia | 12 | M | 0 | 1 | 1 | 0 | 3 (mo) |
| 25 | - | 2001 | Australia | 12 | M | 1 | 0 | 0 | 0 | Uknown |
| 26 | - | 2001 | Australia | 16 | F | 1 | 0 | 0 | 0 | Unknown |
| 27 | - | 2001 | Australia | 9 | F | 0 | 1 | 0 | 1 | 1 (y) |
Prevalence rates of intestinal spirochetosis in adult patients of developed countries are the highest among HIV patients or homosexual males [6,10,11]. Spirochetes are probably transmitted by fecal-oral route. Sexual transmission has also been suggested because of its higher incidence in homosexual males [12]. In children and adult patients, intestinal spirochetosis can be asymptomatic. It can be an incidental discovery during an endoscopy [13-15].
In pediatric patients, an endoscopy is only performed in the setting of important abdominal complaints. Therefore, intestinal spirochetosis is rarely an incidental discovery. Symptomatic intestinal spirochetosis is associated with abdominal pain, diarrhea, rectal bleeding, weight loss, constipation, and nausea. Based on our review, 81.4% (22/27) of children had complaints of abdominal pain, 51.8% (14/27) suffered from diarrhea, 48.1% (13/27) patients with intestinal spirochetosis suffered from rectal bleeding (Table 1), and 14.8% (4/27) had nausea and vomiting. In 85% (17/20) of cases from the literature, the duration of symptoms prior to diagnosis was at least 1 month.
Particularly, children can develop severe symptoms [16-19]. Due to a variety of symptoms, differential diagnosis should include inflammatory bowel disease, infectious, and ischemic or even pseudomembranous colitis [13,20].
Intestinal spirochetosis is reported to be associated with polyps [8]. However, the overall prevalence of polyps in patients with intestinal spirochetosis is not different from that in the general population [21]. A potential association between intestinal spirochetosis and sessile serrated adenomas or polyps was reported and rejected in adults [8,22]. In a Swedish study, 2 out of 8 pediatric patients with intestinal spirochetosis also had JPs [16]. Calderaro et al. [23] have reported a pediatric case of intestinal spirochetosis and JP. In our case series, 1 out of 4 patients had a JP. According to literature review, 5/27 (19%) patients had JP. This is much higher than the prevalence of JP in the general population (1/100). Intestinal spirochetosis might be a risk factor for JP in children. Intestinal spirochetosis is often diagnosed after several months of abdominal complaints. Could this chronic infection/inflammation be a trigger for developing JP?
A study in adults suggested that intestinal spirochetosis was associated with non-constipation irritable bowel syndrome [8]. Co-infection with other micro-organisms was also reported. Helicobacter pylori, Enterobius vermicularis, Shigella Flexneri, Neisseria gonorrhaeqa, Entamoebia histolytica, Blastocystis hominis, Giardia intestinalis, Hymenolepisd nana, and Ascaris are all reported to be associated with spirochetosis [1,21]. In our patients, we found a co-infection with Salmonella and C. jejuni. Hygiene and/or co-infection with other pathogens could be a risk factor. However, this hypothesis needs further research.
Endoscopy is reported to be often macroscopically normal. Erythematous or unspecific lesions are also observed. In half of our patients, irritation of the rectal mucosa was reported. The diagnosis of intestinal spirochetosis is based on histological appearance of a diffuse blue fringe seen on hematoxylin-eosin staining that is approximately 3–6 µm thick along the border of the intercryptal epithelial layer (Fig. 1). This finding is referred to as “false brush border”. It is more clearly seen in a silver WSS (Fig. 2). The surrounding cytostructure can show signs of inflammation (e.g., edema, infiltrate of monocytes, lymphocytes, plasma cells, and neutrophils in the lamina propria and elongated and hyperplastic crypts). On electron microscopy, spirochetes are attached perpendicularly to the epithelial membrane of enterocytes. Microvilli can be shortened or depleted. Defect of the glycocalyx and swelling of the mitochondria can be noticed [2,5,6]. Colonization of several parts of the intestinal is common. The location of the highest colonization rate differs from patient to patient [8]. A recent study has suggested that intestinal spirochetosis is more frequent in the right-side large intestine [24]. Involvement of the appendix has also been reported [25]. Although spirochetes are reported to be most predominant in colon ascendens, symptoms involve the distal colon more.
Fig. 1
Diffuse blue fringe seen on hematoxylin-eosin staining. It is approximately 3 to 6 µm thick along the border of the intercryptal epithelial layer, suggesting the diagnosis of spirochetosis.

Fig. 2
The diffuse fringe is referred to as “false brush border”. It can be more clearly seen in a silver Warthin-Starry staining.

There is a lack of evidence on which is the therapy of choice in children with intestinal spirochetosis. Several treatment strategies have been proposed in the past 2 decades, including macrolide antibiotic, macrolide combined with metronidazole, metronidazole alone, and clindamycin. However, metronidazole seems to become the antibiotic of choice [13]. In the literature, 7 out of 27 patients at diagnosis were treated with metronidazole in monotherapy and 5 of 27 patients were treated with metronidazole combined with amoxicillin. Nevertheless, relapses are frequently reported in the literature. In the review, we found that more than half of patients (14/27) had no complete recovery or relapsed after a first antibiotic treatment when patient was treated with metronidazole.
Spontaneous resolution of symptoms has also been reported [16,26]. One of our patients was treated with amoxicillin clavulanic acid. Two patients received treatment with metronidazole alone. The last one was treated with metronidazole and amoxicillin because of co-infection with Salmonella.
In conclusion, intestinal spirochetosis is a quite rare infection in children. This might be related to the fact that its diagnosis can only be made on intestinal biopsies. Intestinal spirochetosis can cause diverse symptoms such as abdominal pain, diarrhea, rectal bleeding, weight loss, and nausea. As a consequence, endoscopy and histology are recommended in the work-up of a child chronically presenting a combination of these symptoms.
 XML Download
XML Download