

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Basal cell carcinoma (BCC) of skin is most commonly diagnosed malignancy in many countries, especially in those with a large Caucasian population1. A recent analysis shows that the incidence of BCC has rapidly increased in South Korea, although it is still lower than in Western countries2. Because BCC rarely metastasizes, treatment is focused on local control1. However, in certain populations, local treatment is not feasible and systemic treatment is needed, due to a patient's condition or tumor characteristics, including location, burden, and aggressiveness3. However, a standard chemotherapy is not established for BCC and only case reports serve to support various regimens. Therefore, we report here the first case of BCC treated with capecitabine and oxaliplatin combination therapy. The study was approved by the Institutional Review Board of the Jeju National University Hospital (IRB no. JEJUNUH 2017-08-003). We received the patient's consent form about publishing all photographic materials.
CASE REPORT
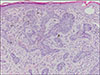
In February 2014, a 57-year-old man visited our out-patient clinic to discuss adjuvant chemotherapy for colon cancer. He had undergone anterior resection on a descending colon cancer in January 2014 and was diagnosed with American Joint Committee on Cancer stage IIIB (T4aN1a) moderately differentiated adenocarcinoma in the colon. Because of the risk of recurrence, we recommended adjuvant chemotherapy (capecitabine and oxaliplatin [XELOX]). After the first cycle of XELOX, we detected a 1-cm crusted ulcerative lesion with an elevated margin on his upper lip, with a vermillion border. He said the lesion had appeared a year prior and continued to grow (Fig. 1A). We obtained a punch biopsy from the skin lesion, and he was diagnosed with BCC in histopathologic examination (Fig. 2). No additional lesions were found in a skin exam.
We consulted a surgeon for treatment of high risk BCC, and he recommended radiation therapy. We believe this recommendation was due to the tumor location and underlying comorbidities, including a history of right middle cerebral artery infarction, diabetes mellitus, asymptomatic myeloma, and colon cancer. However, the patient refused treatment for BCC at that time and postponed the radiation therapy. During discussion of BCC treatment, he continued to receive the XELOX regimen for colon cancer and we found the BCC lesion was improved (Fig. 1B). However, systemic chemotherapy is not the standard treatment for localized BCC. Therefore, after completion of adjuvant XELOX therapy (8 cycles over 6 months), we recommended the radiation therapy for the BCC lesion to the patient again. But he continuously refused the treatment. While he delayed radiation therapy for BCC, the crusted ulcerative tumor lesion gradually normalized, leaving only scarring (Fig. 1C). At his most recent visit, in September 2017, he had no evidence of BCC recurrence (Fig. 1D).
DISCUSSION
Systemic treatment of BCC has mainly been reported in a small number of patients with metastatic or advanced disease34. The limited findings of systemic treatment may be due to the high success rate of local treatment1. However, research for systemic treatment of BCC is essential when considering the increasing incidence of BCC world-wild, the existence patients who are not candidates for local treatment and the lack of improvement in metastatic BCC survival since the 1980s345.
Since a 1978 phase I~II clinical trial for a reported cisplatin response in metastatic BCC, there have been case studies on systemic chemotherapy in BCC with cisplatin containing regimens, combination with 5-FU, bleomycin, doxorubicin, methotrexate, and other regimens3467. However, only platinum-based chemotherapy has been shown to have some efficacy in BCC and no randomized clinical trial have been conducted36. Additionally, vismodegib, an inhibitor of the hedgehog pathway signal transducer protein Smoothened, recently showed a response in BCC, but it is not approved in some countries and is costly with limited evidence of clinical benefit891011. Although the XELOX regimen in this report was not administered for BCC treatment, but was used for colon cancer treatment, this is the first case report of BCC chemotherapy with capecitabine and oxaliplatin. Notably this treatment achieved a complete response in BCC. Because this regimen is widely used for other solid tumors as an alternative to 5-FU and cisplatin to reduce the inconvenience of infusion and potential toxicities (e.g., renal toxicity and emesis), this therapy is known to be well tolerability and toxicity is manageable121314. And previous several reports suggested that low-dose capecitabine (500~1,500 mg/m2 per day for 14 days of a 21-day cycle) has a chemopreventive effect for basal cell carcinoma, squamous cell carcinoma, and actinic keratosis in solid organ transplant recipients who have higher incidence of nonmelanoma skin cancer than the general population151617. Considering these findings, capecitabine and oxaliplatin combination therapy should be studied as treatment for BCC patient who require a systemic chemotherapy option.

 XML Download
XML Download