

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Postoperative nausea and vomiting (PONV) is the most common postoperative complication after orthognathic surgery. Forty percent of patients experience PONV within 24 hours after surgery [1]. To maintain the postoperative occlusion, intermaxillary fixation is performed using an elastic band or wire. In this condition, the risk of airway obstruction is increased because it is difficult to effectively remove intra-oral secretions and bleeding [2]. Therefore, control of PONV is essential.
Bimaxillary orthognathic surgeries are associated with a higher level of pain compared to other oral and maxillofacial procedures [3]. Patient-controlled analgesia (PCA) is widely used for pain control after orthognathic surgeries [45]. PCA using a microprocessor-controlled infusion pump is highly effective in lowering patient anxiety caused by the gap between the patient's pain recognition and time of analgesic administration [6]. Intravenous PCA is used with several types of narcotic analgesics such as morphine, fentanyl, pethidine, piritramide, nalbuphine, and tramadol [7]. These opioids increased the risk of nausea, vomiting, and respiratory depression in some studies [8].
Nefopam is associated with lower incidences of gastrointestinal tract injury, coagulopathy, antipyretic effect, and nephrotoxicity, which are known side effects of Nonsteroidal anti-inflammatory drugs (NSAID) [91011121314]. Recently, clinical use of the nonopioid agent nefopam has increased due to relatively higher safety on hemorrhage, infection, and nephrotoxic patients. Nefopam has also been reported to decrease respiratory depression and PONV, which are adverse effects of opioids [151617]. Furthermore, recent reports suggested that NSAIDs may impede bone healing after orthopedic surgeries [1819], and nefopam does not induce this side effect [20].
This study aimed to investigate whether using nefopam to control postoperative pain following orthognathic surgeries lowered the incidence of PONV with similar pain control effects as fentanyl.
METHODS
1. Trial design
We conducted a single-center, prospective, randomized, double-blind study from August 2015 to December 2017 at Seoul National University Dental Hospital, Republic of Korea. Permission to conduct this study was granted by the institutional review board of Seoul National University Dental Hospital (approval number, CME15001). Written informed consent was obtained from all participants. All aspects of participant privacy and confidentiality were preserved. The investigation was registered with the Clinical Research Information Service (https://cris.nih.go.kr/KCT0001592) and performed according to the guidelines for the proper conduct of medical research on human participants.
2. Participants
Patients undergoing bimaxillary orthognathic surgery with intravenous PCA for postoperative pain control were enrolled. All patients had an American Society of Anesthesiologists (ASA) patient status of I or II and were between 20 and 40 years of age. Exclusion criteria were as follows: (1) urgent or emergent case, (2) re-do case, (3) ASA status of at least III, (4) allergic to fentanyl or nefopam, (5) history of drug abuse, (6) chronic pain (≥ 3 months), (7) use of analgesic or hypnotic medication within 2 weeks, (8) hepatic, renal, or cardiac insufficiency, (9) pulmonary diseases such as chronic obstructive pulmonary disease, asthma, and upper respiratory infection within 2 weeks, (10) smokers, (11) pregnant or breastfeeding, (12) refused to participate, (13) diabetes or neuropathic diseases, (14) unable to use the PCA device, (15) others who the investigator judged to be inappropriate candidates for participation in the clinical study. All patients received a general explanation of the study process, including instruction in the use of the visual analogue scale (VAS) ranging from 0 (no pain) to 10 (worst pain imaginable). The patients were also carefully instructed in use of the Accumate® 1100 PCA device (Wooyoung Medical Co. Ltd., Jincheon, Korea) that was used in the study.
3. Randomization and Blinding
The patients were randomly assigned to one of two groups using a computer-generated random number table (available at http://www.randomization.com/). The patients were allocated to receive either nefopam-based (nonopioid; N group) or fentanyl-based (F group) PCA for postoperative pain control using sealed envelopes containing the treatment options (N and F) before induction of anesthesia. All anesthesiologists, surgeons, nurses, and patients were blinded to the study. All data were collected by trained observers who also were blinded and did not participate in patient care.
4. Anesthesia and PCA
All patients arrived at the operation room without premedication and were not given any preanesthetic medications. Anesthesia was induced after establishing routine patient monitoring (pulse oximetry, electrocardiography, and noninvasive blood pressure monitoring) and bispectral index monitoring. Following preoxygenation, anesthesia was induced with a 5 µg/mL effect site concentration of propofol and 5 ng/mL of remifentanil using an Orchestra Base Primea target-controlled infusion system (Fresinius Kabi, Bad Homburg, Germany). Anesthesia was maintained with propofol (2–4 µg/mL) and remifentanil (3–10 ng/mL) depending on bispectral index level (bispectral index was maintained between 40–60) and vital signs. Rocuronium (0.6 mg/kg) was administered for muscle relaxation following anesthesia induction and additional doses were administered as necessary (self-respiration is restored or the operator wished). After nasotracheal intubation, patients were ventilated with 50% oxygen in air. The tidal volume was 6–8 mL/kg (lean body mass), and positive end expiratory pressure was utilized as necessary. Respiratory rate was adjusted to maintain end-tidal carbon dioxide partial pressure from 30 to 35 mmHg. Invasive blood pressure monitoring and arterial blood gas analysis were performed by placing the catheter on the dorsalis pedis artery. Upon completion of the operation, residual neuromuscular paralysis was reversed using sugammadex (200 mg) and the PCA (Group N, 120 mg nefopam; Group F, 700 mcg fentanyl in total normal saline 120 mL) machine was connected. After recovery of self-respiration, patients were transferred to a postanesthetic care unit. After confirmation of complete recovery of consciousness, self-respiration (with sustained spontaneous respiration rate > 12/min), and an open airway, the tracheal tube was removed.
Twenty milligrams of nefopam provides an analgesic effect equivalent to 6–12 mg morphine, and 10 mg of morphine provides equivalent analgesia to 100 µg fentanyl [21]. Therefore, PCA was set as follows: 120 mg of nefopam for the N group and 700 µg of fentanyl for the F group in total volumes of 120 mL with normal saline. Continuous basal infusion of nefopam or fentanyl was provided (1 mL/hour). The PCA machine allowed for a 1 mL bolus, with a 15 minutes lockout time, and a 5 mL maximum per hour. Drugs were infused using an Accumate 1100®. The PCA device time was synchronized with Korea Standard Time at the national metrology institute. All labels on the PCA devices were hidden so that patients and medical staff who had direct contact with the patients did not know which drug was being administered. If postoperative pain was not controlled by continuous PCA infusion, ketorolac was administered intravenously as a rescue analgesic. If PONV occurred, antiemetics were administered.
5. Outcome Assessments
The primary outcome was the incidence and number of PONV events after surgery. PONV was assessed using a 4-point ordinal scale (0 = none, 1 = nausea, 2 = retching, 3 = vomiting) upon arrival at the Post-anesthesia care unit 0.5, 1, 8, 24, 48, and 72 hours after surgery. Nausea was defined as a subjectively unpleasant sensation associated with awareness of the urge to vomit. Retching was defined as labored, spasmodic, rhythmic contraction of the respiratory muscles without expulsion of gastric contents. Vomiting was defined as the forceful expulsion of gastric contents from the mouth.
The secondary outcomes were pain score, sedation, shivering, difficulty sleeping, and other unwanted symptoms. Pain was assessed using the visual analogue scale (VAS) ranging from 0 (no pain) to 10 (worst pain imaginable) at 0.5, 1, 8, 24, 48, and 72 hours after surgery, both at rest (VASr) and during movement (VASm). Total PCA volume, need for rescue analgesics, and dose of rescue analgesics and antiemetic injections were recorded at 0.5, 1, 8, 24, 48, and 72 hours after surgery. The PCA discontinued if the respiratory rate was < 12/min, oxygen saturation was < 95%, sedation score was ≥ 4, or when other side effects caused by the PCA were suspected. If use of the PCA was discontinued, the reason for discontinuation, and the time at which discontinuation occurred was noted by medical personnel who did not have information about this study. The occurrence of side effects was assessed by checking for sedation, shivering, difficulty in sleeping, constipation, hypotension, and other unwanted symptoms for 72 hours postoperatively. Degree of sedation was scored as follows using the Ramsay sedation assessment scale [22]: 1 = anxious, agitated, or both; 2 = cooperative, oriented, and tranquil; 3 = responds to commands only; 4 = a brisk response to a light glabellar tap; 5 = a sluggish response to a light glabellar tap; 6 = no response. Patient satisfaction scores were also evaluated using a 5-point Likert scale. The Likert scale was scored as follows: 1 = not at all satisfied; 2 = slightly satisfied; 3 = moderately satisfied; 4 = very satisfied; 5 = completely satisfied. All outcomes were collected and analyzed by a biostatistician who was not a participant in the study and only knew details of study design.
After the IV PCA device was collected, information regarding patient self-administration (the time of starting the device, the number of bolus attempts, the amount of bolus drug delivery, and the end of device usage) was downloaded to personal computers loaded with an IV PCA device-specific download program, Eventlog Viewer version 1.1 for Accumate1100 (Wooyoung medical, Inc., Seoul, Korea).
6. Sample Size
To determine appropriate sample sizes, we assumed that incidences of PONV in the F group and the N group of 25% and 10%, respectively, would be significant on the basis of previous publication [16]. Seventy-nine patients per group were required for a power of 80% with a type I error rate of 5%. Considering a drop-out rate of 10%, 174 patients were planned to be included. However, interim analysis after including 89 patients showed a high incidence of PONV in the N group, and the study was stopped.
7. Statistical Analysis
Measured values were presented as mean ± SD or as a number (%). Intra-group distributions of variables were evaluated for normality using the Kolmogorov-Smirnov and histogram tests. Fisher's exact test or χ2 test was used to evaluate categorical variables and Student's t-test or Mann-Whitney U test were used to evaluate continuous variables. P < 0.05 was considered statistically significant. SPSS version 25.0 for Windows was used for statistical analyses.
RESULTS
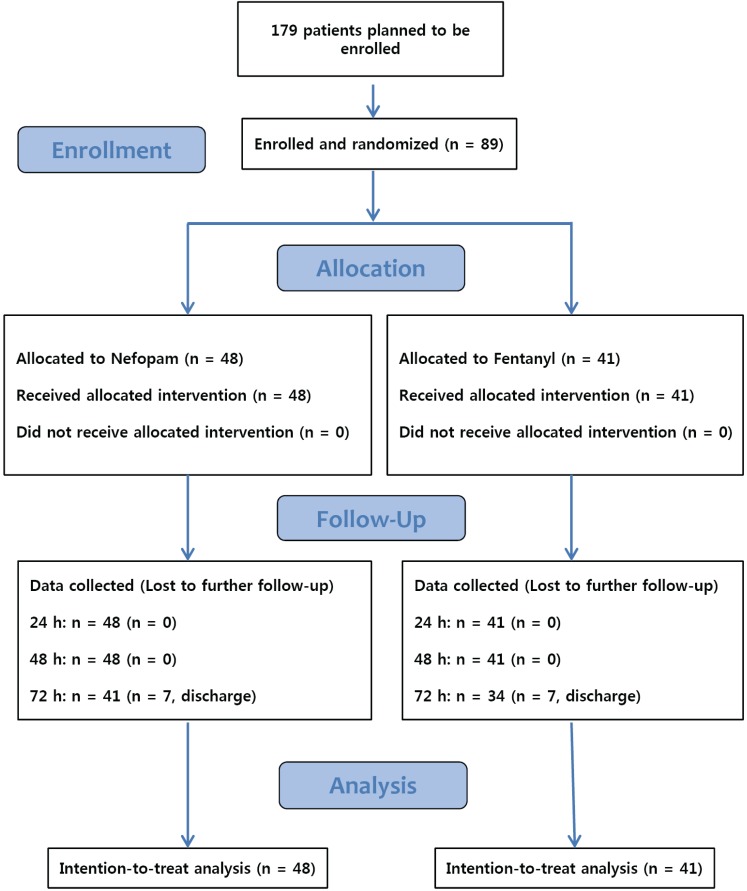
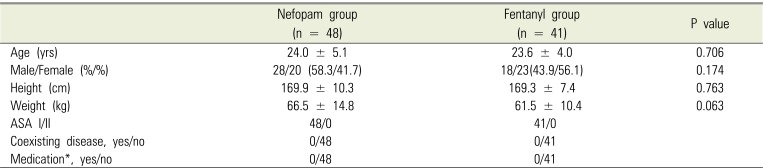
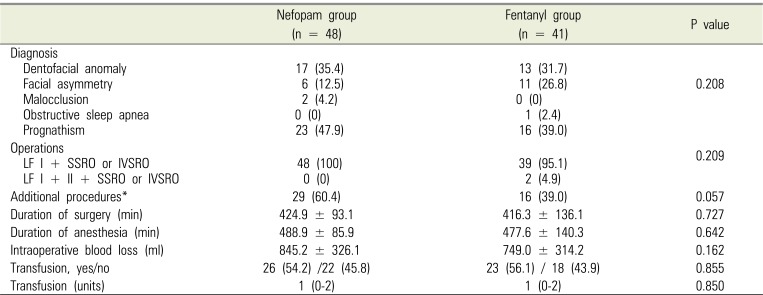
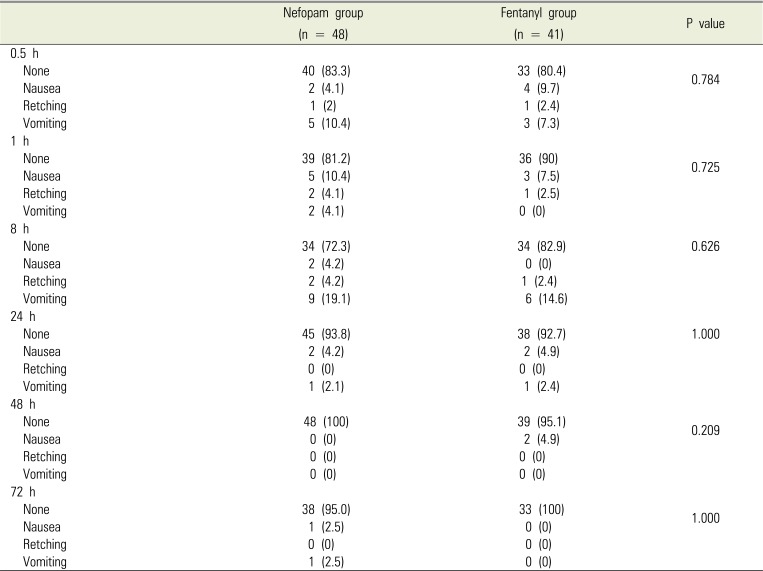
Eighty-nine patients were examined from August 2015 to December 2017, with 48 in the nefopam (N) group and 41 in the fentanyl (F) group. During the 72-h period after surgery, 7 patients in the N group and 7 patients in the F group were discharged, and thus lost to follow-up (Fig. 1). Baseline demographic and perioperative characteristics are shown in Tables 1 and 2, respectively, and there were no significant differences between the two groups. Table 3 shows the incidence of PONV at each time point. In contrast to our hypothesis, in the interim survey of 89 participants, the incidence of PONV was higher in the N group (n = 13, 27.7%) than in the F group (n = 7, 17.1%; P = 0.568) at 8 hours after surgery, so we stopped the study.
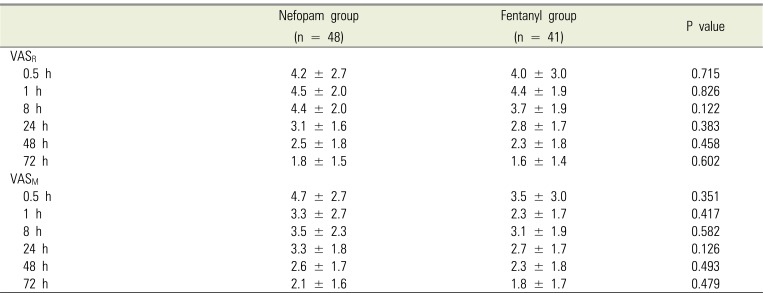
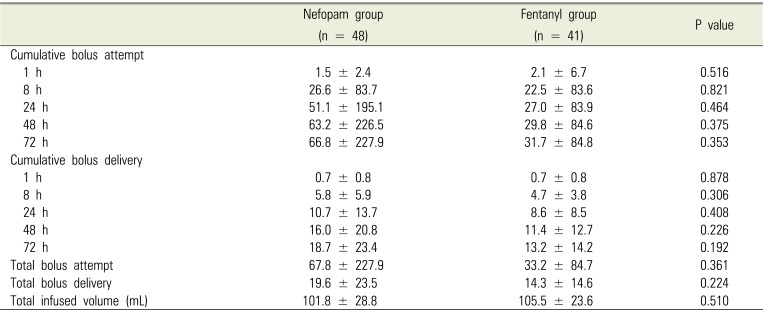
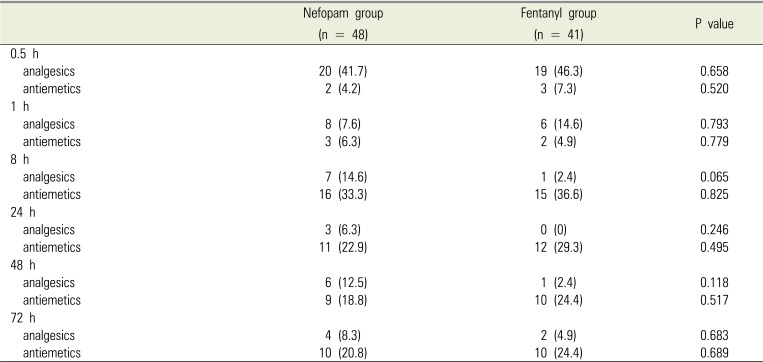
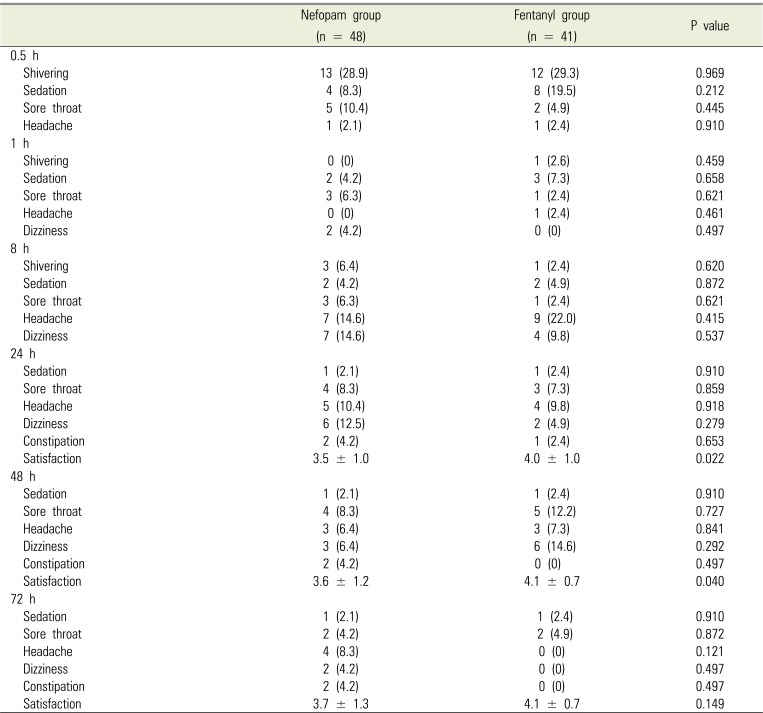
Postoperative pain intensity was measured using VAS (Table 4), with no significant differences between the two groups. In addition, there were no significant differences in total bolus attempts, bolus delivery, and infused volume, all of which were collected from the PCA device at all time points (Table 5). The incidence of use postoperative rescue analgesics and antiemetics at each time point is shown in Table 6, and there were no significant differences between the two groups. The incidence of adverse events and patient satisfaction at different time points following bimaxillary orthognathic surgery in patients receiving PCA with nefopam or fentanyl is shown in Table 7. There were significant differences in patient satisfaction at 24 and 48 hours after surgery between the two groups, with no significant differences for other parameters.
DISCUSSION
Postoperative pain is the greatest fear of patients planning to undergo bimaxillary orthognathic surgery. In general, control of postoperative pain is accomplished by PCA, which can be controlled by patients with low side effects. Opioids are the most common drugs used for PCA [523], and opioids are either used alone or are mixed with NSAIDs [4]. With PCA, postoperative pain intensity is known to decrease to an average VAS score of 4 or below by 8 hours after surgery and to a VAS score of 3 or below by 24 hours after surgery [4]. The amount of analgesics required to control pain following bimaxillary orthognathic surgery has been shown to be less than the amount required following oral cancer surgery [24].
In addition to pain, one of the most suffering adverse events following bimaxillary orthognathic surgery is PONV. Although vomiting after orthognathic surgery is not directly life-threatening, it can cause dehydration, esophageal rupture, wound dehiscence, bleeding, hematoma, and aspiration of gastric contents, and in severe cases may lead to death [1]. Furthermore, PONV prolongs hospital stay, increases costs, and contributes to negative feelings regarding anesthesia and surgery [25]. It is known that the orthognathic surgery itself causes PONV to occur at a frequency as high as 30–50% [126]. Furthermore, use of opioids such as morphine after surgery may increase the incidence of PONV.
Various attempts have been made to reduce the incidence of PONV. Factors that influence the incidence of PONV include age, gender, obesity, vomiting history, psychological state, type and duration of surgery, and type of anesthesia. ppropriate use of antiemetics and analgesics with low risk of adverse effects is important.
Nefopam is a drug that induces central analgesia with an efficacy ratio of about 0.2 to 0.6: 1 (nefopam: morphine). The mechanism of nefopam-induced analgesia has not been clearly established. However, it may inhibit reuptake of neurotransmitters such as norepinephrine, serotonin, and dopamine, and may exert anti-hyperalgesic activity through inactivation of the N-methyl-D-aspartic acid receptor [272829]. Nefopam does not cause respiratory depression, does not inhibit the central nervous system, and has a low risk of nephrotoxicity, cardiovascular toxicity, and abuse [151630313233]. Moreover, nefopam has a definite advantage over NSAID in that it does not cause gastric mucosal erosion or affect platelet aggregation [30]. When used for control of postoperative pain, nefopam can reduce complications caused by opioids by reducing the amount of opioids used [3435]. Recent reports have suggested that NSAIDs can impede bone healing [1819], which is not a known side effect of nefopam, which adds to its benefit as a means for postoperative pain control following orthognathic surgery [20].
Although nefopam can induce adverse effects such as tachycardia, sweating, nausea, vomiting, drowsiness, asthenia, light headedness, and pain at the injection site, these symptoms are typically transient and non-severe [35363738]. Nefopam has recently been reported to lower PONV after laparoscopic gynecologic surgery and cardiac surgery [151617].
In this prospective, double-blind, randomized, and controlled study, we investigated the incidence of PONV, postoperative pain, and other adverse effects in patients who used nefopam or fentanyl for PCA after a bimaxillary orthognathic surgery.
In this study, the pain control effects of nefopam were comparable to those of fentanyl in patients who underwent bimaxillary orthognathic surgery, and there were no significant differences in the incidences of other adverse effects. However, nefopam did not lower PONV in our study.
However, other studies have reported that using nefopam in conjunction with opioids for PCA has opioid sparing effects, which can result in a lower incidence of PONV than when using opioids alone [1639404142]. We may not have observed any benefits of nefopam on incidence of PONV because our study population consisted of patients who underwent orthognathic surgery. A previous study also reported that there were no significant differences in postoperative pain control and incidence of PONV following administration of nefopam or fentanyl [43].
In our study, although incidence of PONV was similar between the groups, patient satisfaction was higher in the F group than in the N group at 24 and 48 hours after surgery. However, previous studies reported no significant differences in satisfaction between the two drugs [43], while other studies reported that patients who received nefopam via PCA were more satisfied [9343944]. Thus, additional studies are needed to further clarify these discrepancies.
This study had several limitations. First, we could not meet our planned sample size. However, we do not believe that having met the planned sample size would have led to different results, and terminating the study due to a higher incidence of PONV in the N group with 89 patients in the interim analysis was the correct ethical decision. Furthermore, based on these findings, we could conclude that the incidence of PONV did not differ between the nefopam and fentanyl groups. Second, we could not standardize the type of rescue analgesics used in the recovery room and in the ward after surgery, and various analgesics, such as fentanyl, pethidine, and ketorolac were used. Furthermore, we could not administer antiemetics in proportion to the actual intensity of nausea and vomiting.
In conclusion, using nefopam for PCA after bimaxillary orthognathic surgery did not significantly reduce the incidence of PONV compared to fentanyl. Furthermore, there were no significant differences in postoperative pain control between nefopam and fentanyl. Based on these results nefopam is a safe drug that can be used to control postoperative pain.
 XML Download
XML Download