

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Syphilis is an ancient sexually transmitted disease (STD) caused by exposure to the bacterium Treponema pallidum. To date, syphilis remains a public health concern despite the availability of improved screening tests and effective and inexpensive antibiotic treatment. Early diagnosis of primary and secondary (P&S) syphilis cases is important because immediate treatment will prevent transmission and development of new cases. In Florida, where syphilis is a reportable disease, the number of P&S syphilis cases has increased by 63%, from 3,266 in 2008–2010 to 5,340 in 2013–2015 [1]. The diagnosis of syphilis is based on a combination of clinical history, risk assessment, symptom presentation, and serological test results [2]. A presumptive diagnosis of syphilis requires the use of two tests: a non-treponemal test (e.g., the rapid plasma reagin [RPR] test or the venereal disease research laboratory [VDRL] test) plus a treponemal test (e.g., enzyme immunoassay [EIA], chemiluminescence microparticle immunoassay [CMIA], or multiplex flow immunoassay [MFI]). Other acceptable treponemal tests include fluorescent treponemal antibody-absorbed or Treponema pallidum particle agglutination (TP-PA) [3].
The Florida Bureau of Public Health Laboratories (FBPHL) currently uses the traditional syphilis algorithm, in which a non-treponemal (RPR) screening test is followed by a confirmatory treponemal (EIA) test. This is currently the algorithm recommended by the U.S. Centers for Disease Control and Prevention (CDC), because non-treponemal tests are inexpensive, relatively easy to perform, and strongly correlated with disease status [4]. However, these tests are interpreted subjectively, require manual processing, and more importantly, are less sensitive than newer U.S. Food and Drug Administration (FDA)-approved treponemal screening alternatives [4]. Currently, a growing number of clinical and public health laboratories have adopted a reverse algorithm for syphilis testing, consisting of a treponemal test (most often EIA, CMIA, or MFI) followed by confirmation of screen-positive specimens with RPR. Discordant specimens that are positive according to the treponemal screening test but negative by RPR are then tested by a second, orthogonal treponemal test to confirm true-positive results.
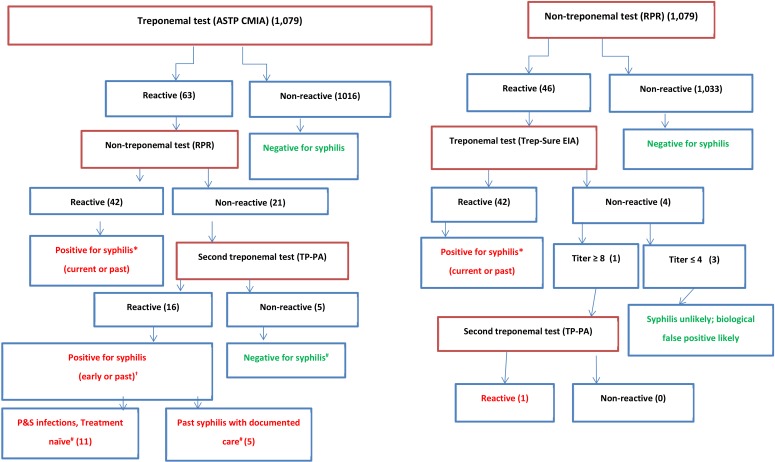
The objective of this study was to compare the performance of the reverse algorithm (Abbott Architect Syphilis TP [ASTP] CMIA screen (Abbott Diagnostics, Chicago, IL, USA)/RPR confirmation/TP-PA if discordant) and the traditional algorithm (RPR screen/Trep-Sure Total EIA [Trinity Biotech, Jamestown, NY, USA] confirmation/TP-PA if discordant) and to determine which algorithm demonstrates greater sensitivity in detecting specifically P&S (infectious) syphilis cases in the FBPHL study population.
Between March 8, 2017, and April 5, 2017, the FBPHL, Jacksonville, retrospectively examined 1,079 well-characterized clinical serum specimens from individuals who self-referred to county public health clinics for syphilis testing. This study was exempted from approval by the Institutional Review Board of the Florida Department of Health, Tallahassee, FL, USA. All specimens were processed within 1–3 days post-collection (no freeze/thaw cycles), according to the traditional algorithm and then additionally tested using the ASTP CMIA. If the ASTP was reactive, the specimen was further tested according to the reverse algorithm. Positive syphilis cases were determined based on a serological profile of two concordant positive treponemal antibody tests or concordant positive treponemal and non-treponemal antibody tests [2]. To differentiate between past/latent or early infections, clinical and treatment data from the Florida Department of Health Patient Reporting Investigation Surveillance Manager (PRISM) database was reviewed. If PRISM did not indicate a latent, sero-fast, or treated status, a positive syphilis case was classified as a P&S infection. Algorithm sensitivity and specificity with respective 95% confidence intervals were calculated.
Of the 1,079 clinical specimens tested using the reverse and traditional algorithms, 59 were classified as positive for syphilis (infectious and non-infectious). The sensitivity of the reverse algorithm was greater than that of the traditional algorithm; however, the specificities of the two algorithms were similar (Table 1). Based on the PRISM database review, of the 16 traditional algorithm-negative but reverse algorithm-positive cases, 68.8% (11/16) were classified as missed P&S infections (treatment naïve), and 31.2% (5/16) were classified as missed past syphilis (latent or infections with documented linkage to care) infections (Fig. 1). Of the 42 specimens positive by both algorithms, 11 were determined to be P&S infections, and 31 were classified as non-infectious stages (early/late latent or treated infections).
In this study, the traditional algorithm failed to detect syphilis in 16 of 59 positive syphilis cases (27.1%), similar to a previous study of approximately 2,700 positive syphilis cases that had found a missed diagnosis rate of 24.2% [5]. Our comparison of the results of the reverse and traditional algorithms highlighted substantial differences in their abilities to detect P&S infections. In 2016, the Florida Department of Health STD Program reported 2,407 infectious cases of P&S syphilis, of which 20.6% (496/2,407) were reported by the FBPHL alone, using the traditional algorithm [6]. Had the FBPHL used the reverse algorithm, an additional 496 P&S cases might have been detected. This would change the state-wide estimate (based on the 2016 data) to a minimum of 2,903 (2,407+496) P&S cases per year.
Laboratories transitioning from the traditional to the reverse algorithm will experience several challenges, including an increase in testing cost. Earlier studies found that initial treponemal screening facilitates identification of probable latent infectious syphilis and its early diagnosis, thus warranting careful communication regarding serological interpretation [78]. The impact of increased laboratory costs and reassessing serological interpretations may be lessened through collaborations between prevention and patient care programs or shared service models between other public health laboratories. Moreover, the additional costs of reagents and automation associated with the reverse algorithm can be mitigated by cost savings due to averted downstream transmissions, as more P&S cases are detected and treated early. A 2008 study examining costs averted by STI prevention programs in the U.S. estimated the direct and indirect P&S treatment cost to be USD 572 and USD 112, respectively, or a total of USD 684 per person per year [9]. The early detection and prompt treatment of an additional 496 P&S cases, assuming a linear relationship of only one downstream transmission per case, would result in 496 averted cases. The total savings in treatment costs due to averted infectious syphilis cases can be conservatively estimated at USD 339,264 (496×684).
We focused on infectious syphilis detection and any determination of syphilis staging, previous testing, and treatment history was limited to data derived from the PRISM database. Sero-fast and reinfection cases are typically identified in PRISM; therefore, all newly reported cases were determined to be P&S infections. Cost analysis was limited to a conservative estimate based on treatment savings associated with averted subsequent transmissions due to P&S cases missed by the traditional algorithm. We do not intend to provide cost estimates for the two algorithms, as this is dependent on laboratory testing volume, possible need for automation, and whether testing can be integrated with another STD testing. Automation of the screening test could result in faster reporting (turn-around-time). Furthermore, we did not examine the sensitivity and specificity of all FDA-cleared automated TP immunoassays. We did not evaluate Trep-Sure or TP-PA as the primary screening test because they do not lend themselves to automation in our high-volume laboratory.
The reverse algorithm enables the detection of syphilis cases missed by our current traditional algorithm. The 63% state-wide increase in acute syphilis cases in 2008–2015 is highly concerning [1]. This increase in P&S syphilis, together with a three-year high HIV transmission rate (as of 2015), suggests a comorbidity and a synergistic relationship [110]. The common means of transmission for these two STDs and the clear evidence that syphilis infection facilitates HIV transmission is a public health concern [1011]. Additional cost data related to algorithm transition is needed to assess overall cost savings or burden to public health STD programs and laboratories, bearing in mind that the objective of testing is to enable early diagnosis of disease and facilitate timely access to medical care for infected persons and their sexual partners.

 XML Download
XML Download