

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Following tooth loss, resorption of the alveolar bone and subsequent remodeling of the alveolar ridge are inevitable. After the extraction of maxillary posterior teeth, pneumatization of the maxillary sinus also becomes problematic [1]. These processes are associated with a decrease in vertical bone height and a low-density trabecular pattern of the maxillary posterior edentulous area used for implant placement [2]. Sinus floor augmentation is considered to be a safe and predictable procedure that compensates for the atrophic alveolar process of the maxilla and facilitates implant placement [3456].
Various bone grafting materials have been introduced for usage in maxillary sinus augmentation to accelerate the process of bone healing and to prevent re-pneumatization of the sinus after grafting. Autogenous bone has been widely used in sinus augmentation, but it has some limitations, such as additional surgical site morbidity and a rapid resorption rate [47]. Recently, a systematic review demonstrated the effectiveness of synthetic bone materials, including biphasic calcium phosphate (BCP), as substitutes for autogenous bone [8]. BCP consists of hydroxyapatite (HA) and β-tricalcium phosphate (β-TCP). In contrast with stable HA, β-TCP is highly resorptive and is replaced by newly formed bone; therefore, the resorption rate of BCP could be influenced by the ratio of HA and β-TCP.
An ideal bone substitute for maxillary sinus augmentation should have dimensional stability to prevent sinus pneumatization [9]. An additional characteristic required for the long-term success of implants is the ability to facilitate as much formation of new bone as possible, while simultaneously providing space maintenance. The dimensional stability of BCP in maxillary sinus augmentation has been investigated in many previous preclinical and clinical studies [101112]. Most clinical studies using a radiographic analysis showed that volume decreased over time, mainly during the initial healing period [13]. According to a recent randomized controlled study, 15%–18% of BCP with 40% β-TCP was resorbed after 6 months [14]. Although previous studies showed initial positive results, the evidence is still currently weak regarding the long-term dimensional stability of BCP used for sinus augmentation.
Our research group evaluated the resorption rate of BCP containing 70% HA and 30% β-TCP radiographically in 20 patients who underwent sinus augmentation and reported minimal resorption of BCP (<1 mm of height resorption) [15]. However, it was found that BCP resorption occurred regardless of the healing period, and the mean follow-up period was only 19.4 months after surgery (range, 12–42 months). Therefore, we concluded that further study would be needed to confirm the long-term dimensional stability of BCP used for sinus augmentation.
The objective of this retrospective follow-up study was to observe the resorption pattern of BCP over a 3- to 6-year healing period after maxillary sinus augmentation, and to investigate factors affecting the resorption of BCP.
MATERIALS AND METHODS
This study was designed as a retrospective, observational study with a single arm, and it was approved by the Institutional Review Board of Yonsei University College of Dentistry (Approval No. 2-2016-0014).
Patient selection
The subjects included patients who received maxillary sinus augmentation using BCP and implant placement at Yonsei University Dental Hospital during the 4-year period from 2009 to 2012. The exclusion criteria were as follows: 1) heavy smoking (>20 cigarettes/day), 2) a debilitating systemic disease such as uncontrolled hypertension or diabetes mellitus, 3) presence of maxillary sinus disease, and 4) presence of periodontal disease on the residual dentition.
A total of 47 implants were placed in 27 maxillary sinuses of 22 patients (11 males, 11 females) with less than 5 mm of residual alveolar bone height. The choice of technique for sinus augmentation was access via a lateral window osteotomy. The demographic information of all patients is presented in Table 1. All implants were followed-up for at least 6 months of prosthetic loading time.
Table 1
Demographic and clinical information of cases

![]()
Materials
Bone substitutes
Osteon (Genoss, Suwon, Korea) was used in all patients. Osteon is a synthetic bone substitute consisting of 70% HA and 30% β-TCP, and its porous structure is known to aid in new bone formation.
Implants
Of the implants, 21 were Implantium (Dentium, Seoul, Korea); 5 were Osstem GSII (Osstem Implant, Busan, Korea); 5 and 3 were ITI BL and ITI Standard (Straumann, Basel, Switzerland), respectively; 4 were Xive (Dentsply Friadent, Mannheim, Germany); 3 were Luna (Shinheung, Seoul, Korea); 2 were Astra (Astra Tech AB, Mölndal, Sweden); 2 were Branemark-MKIII (NobelBiocare AB, Gotenborg, Sweden); and 2 were unknown.
Surgical technique
Preoperative cone-beam computed tomographic images were used to measure residual bone volume, in order to identify patients who needed sinus augmentation prior to implant placement and to aid in the choice of procedure [16]. All patients were given premedication for antibiotic prophylaxis. All implants were placed either on the day of sinus augmentation surgery (1-stage) or post-surgically (2-stage). The timing of implantation was determined based on the predicted primary stabilization of implants. In the 2-stage approach, implants were placed 5–7 months after augmentation of the maxillary sinus.
A modified Caldwell-Luc sinus lift procedure was performed under local anesthesia (2% lidocaine hydrochloride-epinephrine 1:100,000; Huons Co., Seoul, Korea) [23]. The posterior side of the maxilla was exposed after elevation of a full-thickness mucoperiosteal flap. Osteotomy was performed on the lateral wall of the sinus using a diamond round bur and piezoelectric device (Piezosurgery, Mectron s.p.a., Carasco, Italy). The sinus membrane was lifted with care using membrane elevators. The sinus cavity was then packed with bone substitute, and an absorbable sponge (Collatape, Zimmer Dental, Carlsbad, CA, USA) was used to cover the lateral window. The mucoperiosteal flap was sutured for primary closure with absorbable suture material (Monosyn 4.0 Glyconate Monofilament, B. Braun Melsungen AG, Melsungen, Germany; Vicryl 5.0 Polylactim, Johnson & Johnson, New Brunswick, NJ, USA). The prosthodontic procedure was finished after a mean healing period of 6–12 months.
Radiographic analysis
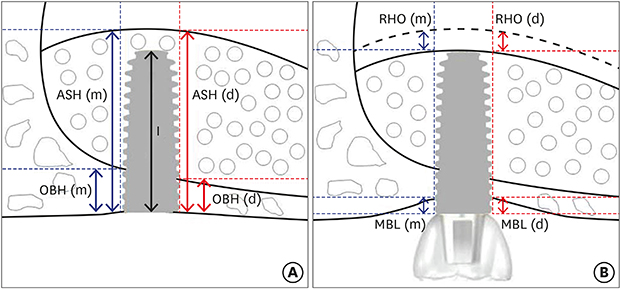
All radiographic measurements were identical to those of the previous study of our research group [15]. Panoramic and intraoral radiographs were taken and an analysis was performed using software (ZeTTA PACS, TaeYoung Soft. Co., Seoul, Korea). At least 2 serial panoramic radiographs were taken; once immediately after sinus augmentation, and the next on the last follow-up visit. The radiographs were taken every 6 to 12 months throughout the follow-up period. The linear measurements made using the radiographs are illustrated in Figure 1.
 | Figure 1Schematic drawing illustrating the linear measurements taken from radiographs. (A) Immediately after the sinus augmentation. (B) Follow-up after the sinus augmentation. Figure 1 is modified from a figure in our previous study [15].ASH(m): mesial augmented sinus height, ASH(d): distal augmented sinus height, OBH(m): mesial original alveolar bone height, OBH(d): distal original alveolar bone height, RHO(m): mesial reduced height of augmented sinus, RHO(d): distal reduced height of augmented sinus, MBL(m): mesial marginal bone loss, MBL(d): distal marginal bone loss, I: implant fixture length.
|
In brief, for each implant site, the original residual bone height—from the alveolar crest to the base of maxillary sinus floor—was calculated on a digital radiograph. The augmented sinus height (ASH) was measured from the implant platform to the base of the maxillary sinus membrane, which was elevated with bone substitute at the mesial and distal aspects of the implants, and then the mean value was calculated and used as a representative value. The reduced height of the augmented sinus (RHO) was calculated as the difference between the ASH between immediately after surgery and at the last follow-up visit. The marginal bone level (MBL) was measured on intraoral radiographs, taken from the most mesial and distal points of the implant platform to the crest of the alveolar bone, corrected according to the known height of each implant. The mean values of MBL were calculated using mesial and distal bone changes at each follow-up visit.
The variables affecting RHO (e.g., healing period, amount of graft material, number and length of implants, timing of implantation [simultaneous or staged], position of implant [lateral or middle], shape of maxillary sinus base [flat or ovoid]) were selected and analyzed statistically.
Statistical analysis
All measurements were evaluated by 1 experienced and calibrated investigator (J.H.K). The number of patients and sinuses from all observation periods were grouped together for the purpose of the statistical analysis. Each sinus was treated here as a separate unit of analysis due to the limited sample size. The statistical analysis was conducted on the implant level and all implants placed on augmented sinuses were included, regardless of whether they were single or multiple implants. A linear mixed regression model was used to determine the effects of various variables on RHO (e.g., healing period, amount of graft material, number and length of implants, timing of implantation [simultaneous or staged], position of implant [lateral or middle], shape of maxillary sinus base [flat or ovoid]). SPSS version 22.0.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses.
RESULTS
Clinical findings
A total of 47 implants placed in 27 sinuses of 22 patients were investigated in the present study. The mean follow-up period after sinus augmentation was 53 months (range, 20–72 months). Implants were placed simultaneously in 11 sinuses and staged after 6 months in 16 sinuses. The amount of graft material used ranged from 0.5 g to 3 g.
Sinus membrane perforation occurred in 1 patient, but no complications such as wound dehiscence or infection were observed in any patients. During the follow-up period, no implant loss was found, corresponding to a 100% survival rate (Figure 2). One patient received flap surgery for treatment of peri-implantitis 5 years after implant placement and healed successfully.

Radiographic analysis
In 27 sinuses, an ovoid shape of the sinus base was observed in 11 sinuses, and the remaining 16 sinuses were flat. The original sinus height was 4.27±1.78 mm, and the ASH immediately after surgery was 13.74±2.97 mm. The changes of ASH in all individuals are presented in Figures 3 and 4. The mean RHO up to 36 months was 0.27±1.08 mm for 23 sinuses in 19 patients, and the mean RHO at 72 months postoperatively was 0.89±1.39 mm for 3 sinuses in 2 patients. Three maxillary sinuses showed over 2 mm of RHO, 7 sinuses showed 1–2 mm of RHO, and 17 sinuses showed less than 1 mm of RHO; on the implant level, those amounts of RHO were found for 3, 8, and 36 implants, respectively. In no cases did the implant apex protrude beyond the maxillary sinus membrane. The MBL was 0.27±1.07 mm at 36 months and 0.90±1.30 mm at 72 months.
 | Figure 3Graph showing changes of augmented sinus height over the follow-up period in all participants.
|

None of the suspected influencing factors had a significant influence on RHO, except for the amount of grafted material and the healing period (P=0.021 and P=0.035, respectively; Table 2). There was a significant relationship between a healing period longer than 40 months and RHO.
Table 2
Effects of the investigated factors on reduced height of sinus augmentation
CI: confidence interval of the difference between means, BCP: biphasic calcium phosphate.
a)Significantly different from the control group (P<0.05).
![]()
DISCUSSION
This retrospective study was designed to investigate the resorption of BCP and to elucidate which factors affected the resorption of BCP used for maxillary sinus augmentation. The most notable finding of this study was that the BCP was merely resorbed and its volume was well maintained over the course of a long-term healing period. Moreover, the amount of BCP and a healing period longer than 40 months influenced the proportion of BCP resorption.
The space in the maxillary sinus cavity augmented by bone substitute mimics a type of contained defect surrounded by basal bone and the Schneiderian membrane. Due to this morphology, it has an excellent potential for healing even in the absence of bone graft materials [17]. At the same time, it is constantly under pressure exerted by the intra-sinus air, promoting resorption of the bone grafts, which might result in volumetric shrinkage after sinus augmentation [18]. For those reasons, synthetic or xenogeneic bone materials, which are more stable over time, are considered to be a better choice of material in terms of resorption [19], and a long-term study is needed to evaluate the dimensional stability of grafted material.
Several human biopsy studies have investigated xenografts used for maxillary sinus augmentation with a long-term healing period, and most of them have showed minimal resorption of the xenograft. Sartori et al. [20] presented a case report with 10 years of follow-up after maxillary sinus augmentation with anorganic bovine bone. That histologic study showed that the amount of newly formed bone was 69.7% after 2 years and 86.7% after 10 years, indicating the slow resorption process of bovine bone. Similarly, it was observed that the bovine bone particles were well-integrated with mature compact bone after sinus augmentation in humans, with no significant changes in particle size found even after 11 years [21]. Iezzi et al. [22] reported slow resorption of anorganic bovine bone in sinus augmentation, finding that the mean amount of mature bone was 71.0%±2.28% and that the mean amount of ABM was 22.1%±3.18% 14 years after sinus augmentation.
In contrast, to the best of our knowledge, only a few studies have reported the long-term outcomes of implants placed after sinus augmentation using BCP. Recently, a human autopsy study was published to characterize the histologic and micro-computed tomographic results of maxillary sinus augmentation using BCP and simultaneous implant placement at 6 years [23]. In that study, the BCP in the maxillary sinus showed well-maintained volume and was surrounded by lamellar bone, confirming its dimensional stability and the success of bone formation.
Mordenfeld et al. [24] compared the grafted sinus height using either BCP or anorganic bovine bone in bilateral maxillary sinus augmentation at different time points. In that study, the graft height reduction after 6 years was limited to 6.6% for BCP and 5.8% for bovine bone, and there was no statistically significant difference between the groups. The BCP used in that study was composed of 60% HA and 40% β-TCP, which appeared to be one of the reasons for the minimal resorption rate of BCP at 6 years, as was also the case in the present study.
In contrast, previous studies using only β-TCP as the augmented material showed a significant decrease of sinus augmented height. Okada et al. [25] reported the volumetric changes of β-TCP in 30 patients based on cone-beam computed tomography. In that study, the volume of β-TCP decreased by 75.6% at 6 months after implant placement, and it decreased further at 2.5 years. The implant apex protruded beyond the maxillary sinus floor in approximately 70% of the implants at 2.5 years after surgery. Likewise, Zijderveld et al. [18] performed a 5-year radiographic analysis to evaluate the changes of β-TCP with autogenous bone, and reported that most β-TCP resorption took place within 7.5 months. Although some studies have shown a high implant success rate, these results suggest that it may be difficult to prevent maxillary sinus pneumatization by β-TCP. Thus, the results of the present study further imply that BCP may be preferable for dimensional stability in sinus augmentation procedures.
Among the various factors analyzed in the present study, only the amount of BCP and the healing period affected the resorption of BCP in the regression analysis. The timing of implantation (simultaneous or staged), length and position of implants, and shape of the maxillary sinus base (flat or ovoid) did not have any influence on the resorption of BCP. A greater amount of BCP was related to a greater reduction of RHO. Since the amount of BCP is directly related to the volume of the augmented maxillary sinus, this is considered to have been a major factor influencing the resorption of BCP.
Only healing periods longer than 40 months had a significant influence on RHO. This result is not in agreement with prior studies, which evaluated the changes in vertical height of different graft materials used for sinus augmentation. In previous studies, a significant decrease in augmented height was observed between baseline and approximately 2 years, and subsequent changes were minimal [182627]. However, regarding BCP specifically, a previous study showed similar results to those of the present study. As discussed above, Mordenfeld et al. [24] evaluated the reduction of graft height after 6 years, and found a reduction of only 6.6% for BCP, but the decrease was statistically significant between baseline and 6 years. The MBL in this study at 72 months was 0.90±1.30 mm, which is in accordance with previous studies [2428].
In the present study, all radiographic parameters were evaluated using digital panoramic and periapical images. To improve the accuracy of the measurements, cone-beam computed tomography could be used. Three-dimensional volumetric analysis could supply more detailed information about the anatomy of the augmented sinus, thereby enhancing the quality of the study. Moreover, the sample size and healing period were limited in the present study. Therefore, it seems to be necessary to conduct a long-term prospective study with a larger number of subjects.
Within the limitations of this study, it can be concluded that BCP can achieve proper dimensional stability with minimal reduced grafted height in a 3- to 6-year healing period after maxillary sinus augmentation.
 XML Download
XML Download