

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Mechanical engagement between implant threads and host bone contributes to primary implant stability after implant placement [1]. The host bone adjacent to the implant surface undergoes remodeling over time, resulting in secondary implant stability, which is referred to as osseointegration [2]. Although some studies demonstrated that secondary stability could be achieved even without primary stability [34], good primary stability is generally regarded as a prerequisite for successful osseointegration because it prevents fibrous tissue formation between the implant surface and host bone [5].
Good primary stability also has other advantages, such as reducing the need for surgical interventions and expediting the restoration of esthetic and masticatory functions. For instance, a lack of primary stability requires submerged healing, followed by secondary uncovering surgery after a proper healing period. Moreover, immediate or early delivery of a prosthesis with or without loading requires a certain level of primary stability [67].
Various methods, such as cutting torque resistance analysis, the reverse torque test, the percussion test, the impact hammer method, and resonance frequency analysis, can be used to measure implant stability [1]. Periotest values (PTVs) and implant stability quotient (ISQ) values are the most commonly used parameters because of their clinical correlations. PTVs range from −8 to 50, and the classification of the range is defined as follows: i) −8 to 0: good osseointegration, ii) 1 to 9: a borderline implant requiring clinical examination, and iii) ≥10: insufficient osseointegration [8]. The ISQ (range: 0–100) is a conversion of the resonance frequency value (3,500 to 8,500 Hz) [9]. Generally, ISQ values are interpreted as follows: i) >70: high stability, ii) 60–69: medium stability, and iii) <60: low stability. Specifically, implants with an ISQ value <60 should be carefully monitored, a traditional loading protocol should be applied for implants with an ISQ value of 60–65, and early loading is considered feasible if the ISQ is >65 [101112].
Implant stability can be affected by the extent and the location of peri-implant bone defects [1314]. Peri-implant bone deficiency over a certain threshold may hinder proper primary stability. Peri-implant bone deficiency is generally compensated using bone augmentation, and implant stability may increase immediately after augmentation in cases of an extraction socket defect [15] and over time due to bone consolidation [16]. Moreover, an important point to consider is that stability measurements are generally made in a specific direction, mainly the buccal aspect, regardless of the location of the bone defect. This is due to presence of adjacent structures (the tooth, implant, and other anatomical structures) and the inappropriate angulation of the other aspects (mesial, distal, and lingual aspects). Information regarding the influence of the measurement direction on implant stability is scarce in the literature.
Therefore, the aim of the present study was to evaluate the effect of the extent of peri-implant bone defects on implant stability (evaluated using PTVs and ISQ values), with respect to the measurement direction. Additionally, the effect of using bone cement to fill peri-implant defects on implant stability was evaluated.
MATERIALS AND METHODS
Implant placement and defect preparation
This study included 10 bovine rib bones with 4 dental implants placed in each of them (total number of placed implants: 40).
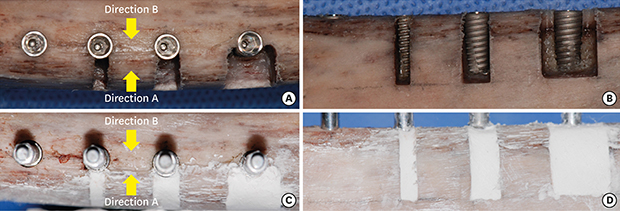
To place the bone-level implants (Ø4.0×10 mm, Luna, Shinhung Co., Seoul, Korea), osteotomies were performed according to the manufacturer's protocol. Varying sizes of box-type dehiscence defects were made on 1 side of the 3 osteotomies using a high-speed diamond bur, thus forming 4 groups: i) no dehiscence (D0), ii) a 2-mm-wide dehiscence defect (D2), iii) a 4-mm-wide dehiscence defect (D4), and iv) an 8-mm-wide dehiscence defect (D8). The height of all defects in groups D2, D4, and D8 was 10 mm. After preparing these defects, implant placement was performed with a maximum insertion torque of 25 N⋅cm (Figure 1A and B).

Measurement of ISQ values and PTVs
In order to measure ISQ values and PTVs, the rib bones were firmly fixed using a vise. Subsequently, a #7 Smartpeg was connected to the implant with hand-tightening force, and ISQ values were measured in 2 directions (Osstell Mentor®, Osstell AB, Gothenburg, Sweden): i) from the aspect with the defect (direction A), and ii) from the aspect opposite to that with the defect (direction B). The PTVs (Periotest M, Medizintechnik Gulden e. K., Modautal, Germany) were then measured from the aforementioned 2 directions after connecting a healing abutment (Ø4.5×3 mm, Luna, Shinhung Co.) Three measurements from each direction were made and averaged.
Application of bone cement
To simulate bone grafting, bone cement (Polybone, Kyungwon Medical, Cheongju, Korea) was mixed according to the manufacturer's protocol and applied to the defect area up to the level of the adjacent bone (Figure 1C and D). Once the bone cement hardened, ISQ values and PTVs were measured.
Statistical analyses
A statistical software program (SPSS Statistics 21.0, IBM Corp., Armonk, NY, USA) was used for all statistical analyses. The data are presented as mean±standard deviation. The Shapiro-Wilk test was applied to test the normality of the distribution. Then, the paired t-test or the Wilcoxon signed rank test was used to assess the statistical significance of differences between the measurement directions and differences before and after bone cement application. Repeated-measures analysis of variance or the Friedman test was used to assess the statistical significance of differences between groups with various defect widths, followed by the post hoc Bonferroni or Dunn test for intergroup comparisons. The level of statistical significance was set at P<0.05.
RESULTS
Implant stability in the presence of bone defects
As the defect size increased, the ISQ value decreased, irrespective of the measurement direction. These values ranged from 84.5±2.1 (group D0) to 60.3±5.9 (group D8) for direction A, and from 84.8±2.4 (group D0) to 61.2±6.2 (group D8) for direction B. An opposite tendency was observed for PTVs, which ranged from −6.2±0.3 in group D0 to −0.3±2.5 in group D8 for direction A, and from −6.4±0.5 in group D0 to 1.8±2.8 in group D8 for direction B. Statistically significant differences were found between groups D0 and D8, D0 and D4, and D2 and D8 for both measurement methods and both measurement directions (P<0.05) (Table 1).
Table 1
ISQ values and PTVs before and after bone cement application (mean±standard deviation)
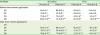
D0: group with no dehiscence; D2: group with a 2-mm-wide dehiscence defect; D4: group with a 4-mm-wide dehiscence defect; D8: group with a 8-mm-wide dehiscence defect; Direction A: from the aspect with the defect; Direction B: from the opposite aspect of the defect. To analyze the directions before bone cement application, the paired t-test was used in groups D0 and D8 for ISQ values, and in groups D0, D2, and D4 for PTV (the Wilcoxon signed rank test was used for the other comparisons). To analyze the directions after bone cement application, the paired t-test was used for all comparisons. The Friedman test was used to assess intergroup statistical differences before bone cement application, and repeated-measures analysis of variance was used to assess intergroup statistical difference after bone cement application. The Wilcoxon signed rank test was used to analyze intragroup statistical differences in groups D2 (ISQ value in direction A) and D8 (ISQ value in direction B, PTV in direction A), and the paired t-test was used for the other intragroup comparisons.
ISQ: implant stability quotient, PTV: Periotest value.
a)Statistically significant difference compared to D0; b)Statistically significant difference compared to D2; c)Statistically significant difference compared to direction A; d)Statistically significant difference between before and after bone cement application; e)Statistically significant difference compared to D4.
![]()
In terms of the measurement direction, there was no statistically significant difference in any of the groups when ISQ values were measured. However, there was a statistically significant difference in the D8 group (P<0.001) and a borderline significant difference in the D4 group (P=0.058) when PTVs were measured (Table 1).
Implant stability after bone cement application
Once the bone cement hardened, increased ISQ values and decreased PTVs were observed compared to the values obtained without bone cement. With increasing defect size, ISQ values decreased and PTVs decreased. The ISQ values ranged from 84.0±1.8 (direction B in group D2) to 77.9±2.1 (direction B in group D8), and there were statistically significant differences between groups D2 and D4 and between groups D2 and D8 (P<0.05) in both directions. The PTVs for direction A were −6.3±0.7 in group D2, −5.1±1.1 in group D4, and −3.1±1.4 in group D8, with statistically significant differences in all intergroup comparisons (P<0.05). The PTVs for direction B showed the same trends as direction A, with statistically significant differences between groups D2 and D8 and between groups D4 and D8 (P<0.05) (Table 1).
The ISQ values demonstrated a statistically significant difference between directions A and B in all groups, although the differences were numerically small (P<0.05). The PTVs only showed a statistically significant difference between the 2 directions in the D8 group (P<0.05) (Table 1).
Changes of implant stability before and after bone cement application
Larger defects were associated with greater increases in both ISQ values and PTVs. In group D8, the ISQ values increased by 17.9±4.3 and 16.7±4.9, and the PTVs increased by −2.8±2.4 and −4.1±2.1 for directions A and B, respectively. All changes between before and after bone cement application were statistically significant (P<0.05).
DISCUSSION
The present study evaluated the effects of the extent of peri-implant bone defects and bone cement on implant stability with respect to the measurement direction. The results revealed that i) narrow peri-implant bone defects (group D2) did not affect implant stability; ii) wide peri-implant bone defects above a certain level (group D8) jeopardized implant stability; iii) the PTVs of implants with wide peri-implant bone defects were inconsistent and depended on the measurement direction, unlike the ISQ values (group D8); and iv) application of bone cement significantly increased implant stability, with a greater increase in the groups with larger defects (D4 and D8).
Various forms of bone defects are simultaneously treated with implant placement. However, these bone deficits may affect the primary stability. Lack of primary stability may jeopardize or delay secondary stability. The present study used box-type bony dehiscence to simulate peri-implant bone deficiencies. In group D2, with narrow bony dehiscence defects, good implant stability was achieved because most of the implant surface was embedded in the bone. However, there was a tendency for the implant stability to decrease in group D4, where approximately 25% of the implant surface was not embedded in the bone. Despite this tendency, implant stability in group D4 was still clinically acceptable (ISQ: 73.9–74.0, PTV: −3.0 to −1.5). In group D8, where approximately 50% of the implant surface was not embedded in the bone, implant stability demonstrated a statistically significant drop as compared to that in groups D0 and D2, resulting in unacceptable ISQ values and PTVs for early loading, as 3 specimens from group D8 demonstrated ISQ values <60. A similar significant decrease was demonstrated in a previous study. In a formalin-fixed cadaver model, the removal of peri-implant bone along up to a 180º perimeter in the presence of a 6-mm-long dehiscence led to a significant decrease of implant stability, compared to what was observed before bone removal [13]. This observation indicates that above a certain threshold of bone deficiency around the implant, primary stability is hampered.
A particularly remarkable finding was the difference in PTVs in the presence of peri-implant defects according to the measurement direction, which has rarely been reported in previous studies, especially in clinical studies [12713151620212223]. In groups D4 (P=0.058) and D8 (P<0.001), the PTV measured from the aspect of the defect (direction A) was lower than that measured from the opposite direction (direction B). This may be derived from the principle of stability measurements made using Periotest. This device delivers several impacts to the implant abutment to measure the contact time between the test object and tapping rod, and then converts the measurement to PTVs [1]. When PTVs were measured in direction A, there was a bony wall supporting the implant from the other side, but there was limited support for the implant when PTVs were measured in direction B. Thus, the impact in direction B from the Periotest device may have delivered a dislodging force to the implant, possibly contributing to the different PTVs between the 2 directions. Even though the ISQ values were constant in groups D4 and D8 irrespective of the directions, this finding leaves room for discussion regarding which value is clinically more trustworthy. Moreover, in a clinical setting, clinicians can only measure PTVs from the buccal aspect.
In the present study, bone cement was used to simulate bone grafting and subsequent consolidation. After hardening of the bone cement, the ISQ values and PTVs showed a statistically significant increase, with varying amounts. Especially in the D8 group, the ISQ values and PTVs were approximately 77–78 and −3 to −2, respectively, which were suitable for loading. Previously, the effect of bone cement on achieving greater implant stability in circumferential peri-implant defects was tested in vitro [23]. In that study, circumferential defects with depths of 2.5 mm and 5 mm were used. The mean ISQ value changed from 69.42 to 73.72 in the group with 2.5-mm-deep defects and from 57.43 to 67.88 in the group with 5.0-mm-deep defects. Considering those findings, it should be clinically emphasized that sufficient healing time for new bone formation around an implant should be provided before prosthetic loading in cases with large peri-implant defects. However, the duration of healing may be case-specific due to variations in individual healing potential, bone quality, and material characteristics.
A limitation of the present study was the relatively thick cortical bone of the rib bone (approximately 3–4 mm). In a human cadaveric study, the mean thickness of the buccal and lingual cortical bone ranged from 1.04 to 2.06 mm and from 1.36 to 2.39 mm, respectively [24]. In a computed tomography study, the cortical bone plate was measured as between 1.3 and 2.0 mm in premolar and molar areas [25]. Therefore, the ISQ values and PTVs in the present study may not correspond to the values from human alveolar bone. Moreover, even though the hardening of bone cement material is a convenient way to simulate bone graft material consolidation, it should be noted that healing dynamics in vivo are more complex, meaning that this study should be further supported by clinical studies. Lastly, the quality of the regenerated bone on the implant surface may be different from that of bone cement.
In conclusion, a wide peri-implant bone deficit (over 50% of the implant surface) could compromise the primary stability of the implant. In terms of the measurement direction, Periotest showed inconsistent values for implants with peri-implant defects above a certain threshold. Bone grafting using bone cement contributed to an increase in the implant stability.
 XML Download
XML Download